Article Text

Abstract
Background/context Unnecessary laboratory testing leads to considerable healthcare costs. Aspartate aminotransferase (AST), commonly ordered with alanine aminotransferase (ALT) and blood urea nitrogen (BUN), commonly ordered with creatinine (Cr), often add little value to patient management at significant cost. We undertook a choosing wisely based quality improvement initiative to reduce the frequency of testing.
Objectives To reduce the ratio of AST/ALT and BUN/Cr to less than 5% for all inpatient and outpatient test orders.
Measures Absolute number and ratio of AST/ALT and BUN/Cr; AST, ALT, BUN and Cr tests per 100 hospital days; projected annualised cost savings and monthly acute inpatient bed days.
Improvements We created guidelines for appropriate indications of AST and BUN testing, provided education with audit and feedback and removed AST and BUN from institutional order sets.
Impact/results The ratios of AST/ALT and BUN/Cr decreased significantly over the study period (0.37 to 0.14, 0.57 to 0.14, respectively), although the goal of 0.05 was not achieved due to a delay in adopting the choosing wisely strategies during the study time period by some inpatient units. The number of tests per 100 hospital days decreased from 20 to 7 AST (95% CI 19 to 20.5, 5.6 to 8.7, p<0.001) and from 72 to 17 BUN (95% CI 70 to 73.4, 16.6 to 22.9, p<0.001). The initiative resulted in a projected annualised cost savings of C$221 749.
Discussion A significant decrease in the AST/ALT and BUN/Cr ratios can be achieved with a multimodal approach and will result in substantial healthcare savings.
- quality improvement
- laboratory medicine
- educational outreach, academic detialing
Statistics from Altmetric.com
Introduction
Since the inception of the Choosing Wisely initiative, overutilisation of healthcare resources has been a focus of healthcare institutions worldwide.1 Unnecessary laboratory tests are an important contributor to overutilisation. Unnecessary laboratory tests cost approximately C$40 million dollars in Eastern Ontario, Canada and over US$5 billion in the USA.2 3 Two of the most routinely ordered laboratory tests are the aspartate aminotransferase (AST) and blood urea nitrogen (BUN). In 2006, nearly 5 million AST tests were performed in Ontario provincial community laboratories.4 Many of these AST tests are unlikely to have resulted in changes to patient management. The 2017 American College of Gastroenterology (ACG) Clinical Guidelines for Evaluation of Liver Chemistries reported that alanine aminotransferase (ALT) is a more specific marker of hepatocellular injury, whereas an elevation in AST could represent injury to other tissues that contain this enzyme, including cardiac and skeletal muscle, kidney and brain.5 6 The ACG guideline outlined specific indications where ordering AST may be appropriate, including establishing a diagnosis of alcoholic hepatitis as a cause of liver disease when the AST/ALT ratio exceeds 2.6 7 AST may also be useful in validated scoring systems for assessment of hepatic fibrosis.6 8 A large prospective study of liver testing strategies suggests that the majority of severe liver disease can be detected by the combination of ALT (for hepatocellular disease) and alkaline phosphatase (ALP) (for hepatobiliary disease).9 Due to its limited utility as a specific marker of liver injury, various groups have questioned the routine testing of AST and have implemented interventions to reduce its use.4 10–12 In 2007, AST was removed from the Ontario Provincial Laboratory Requisition and non-hospital affiliated labs commenced charging patients for AST testing.4
Similarly, many BUN tests are potentially unnecessary. The use of BUN as a marker of renal function is controversial as numerous factors unrelated to glomerular filtration rate (GFR) may influence levels including protein intake and use of diuretics.13 14 Serum creatinine (Cr) is a more reliable measure of GFR and a more valuable test of renal function.14 The BUN does offer value in certain clinical indications including determining urea clearance for patients on dialysis, as well as helping to support a diagnosis of occult upper gastrointestinal bleeding (BUN/Cr ratio >30).15 16 The relationship between BUN and Cr at the initiation of dialysis may also have prognostic value as a predictor of all-cause mortality.13 Further, some clinicians recommend the use of the fractional excretion of urea to differentiate between prerenal acute kidney injury and acute tubular necrosis as a cause of renal failure.17
Reasons for overutilisation of laboratory testing include: (1) ordering tests in panels; (2) limited knowledge of guidelines or education of healthcare professionals; (3) defensive testing; (4) unnecessary repetition of inpatient blood work and (5) lack of appreciation of laboratory costs.18 Common intervention strategies for curtailing laboratory testing include administrative changes, guideline formalisation, education and audit and feedback.10 12 19 20 Interventions that have implemented both educational and process changes to reduce unnecessary laboratory testing have achieved modest decreases between 7% and 21% in testing.20 21 A previous study reported an estimated cost savings of US$247 000 for 12 biochemistry tests that were addressed by an administrative intervention, reducing AST testing by 17.9% and BUN testing by 7.8%.20
We suspected that the majority of the AST and BUN tests ordered in our institution were unnecessary due to a lack of knowledge of appropriate indications for test ordering and outdated processes of ordering. Our multidisciplinary team estimated that five AST and five BUN tests would provide useful information for every 100 ALT and Cr tests, respectively. The goal of 5% was chosen a priori as a reasonable target where the vast majority of tests would be expected to be within guidelines. The primary objective of this study was to reduce AST and BUN testing to a ratio of 0.05 AST/ALT and BUN/Cr.
Methods
Context
Our quality improvement initiative was conducted at a tertiary care institution (590 active-treatment beds) in Canada. Our institution is a academic centre with expertise in trauma, cardiology, high-risk obstetrics, specialised intensive care, medical oncology and cardiovascular surgery. This study was exempt from ethics review according to institutional guidelines as a quality improvement activity.
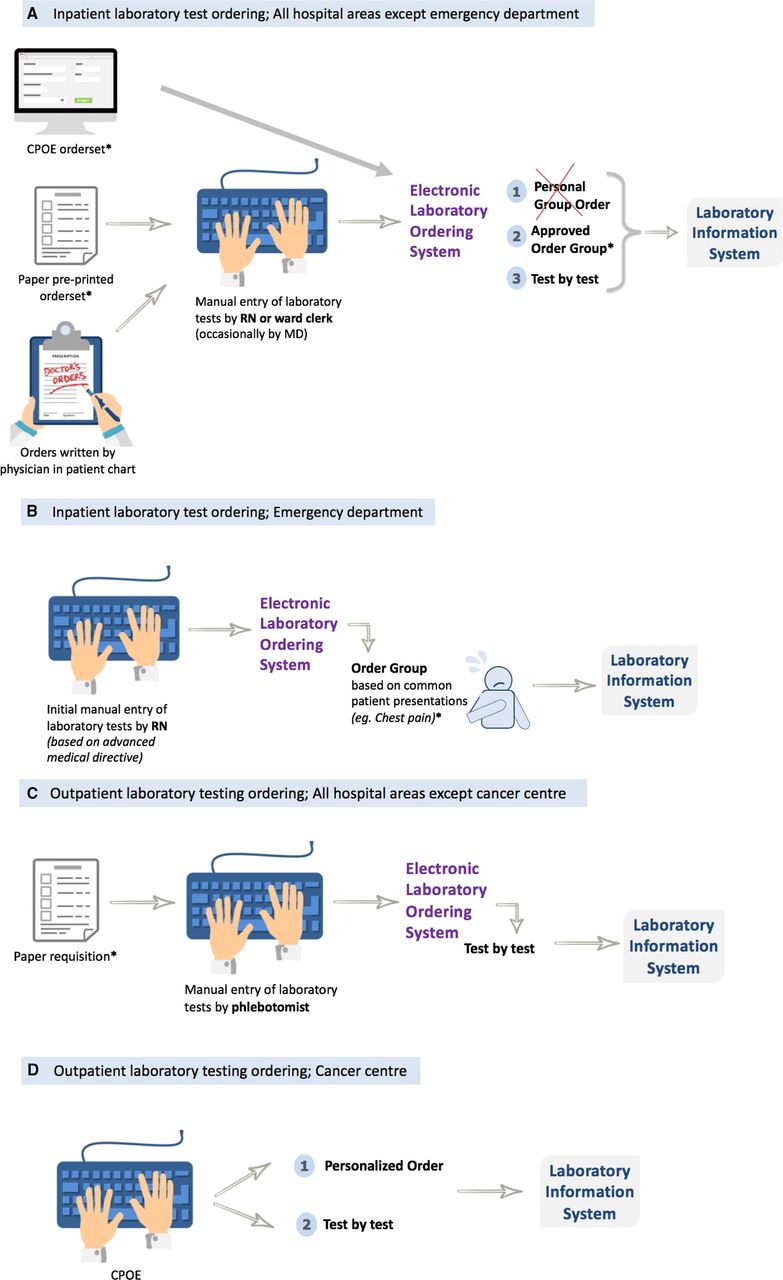
The overall process of laboratory test ordering for different areas of our institution is presented in figure 1A–D. For general inpatient testing, physicians order tests on a blank paper order sheet or using preprinted paper order sets (example shown in online supplementary appendix 1). Some order sets are available electronically with the content identical to that of the paper order sets. Prior to our initiative, many paper and electronic order sets had a fixed option requiring ordering to AST and ALT together or BUN and creatinine together. The nurse or ward clerk who receives the physician’s lab order enters the test into the electronic laboratory ordering system, OACIS (Telus Health, Montreal, Canada). Rarely a physician enters the order into the electronic laboratory ordering system. Within the system, the tests can be ordered individually or grouped (AST and ALT grouped as a ‘liver profile’; BUN and Cr grouped as a ‘renal profile’). In addition, any clinical department can request a shared computer order set within the electronic laboratory ordering system that may be used by any user. For example, staff in the emergency department (ED) use a shared order set for patients with a suspected gastrointestinal bleed which included BUN. Individual users may also create a personal order set to expedite the order entry process. For example, an ED triage nurse might create a panel of tests for patients arriving with abdominal pain that might include AST. Outpatient laboratory tests, including those within family practice, are ordered by a physician using a paper requisition with all tests listed separately (AST and BUN were listed on the requisition prior to intervention). The patient brings the requisition to outpatient collection areas, where the phlebotomist collects the sample. Physicians are able to preorder monthly or quarterly tests for a particular outpatient population up to a maximum of 1 year into the future.
Supplemental material

(A–D) Process of ordering inpatient and outpatient laboratory tests with implemented interventions. *AST and BUN removed from paper order sets, CPOE order sets, shared order groups and individual order groups from within the electronic laboratory ordering system. AST, aspartate aminotransferase; BUN, blood urea nitrogen; CPOE, computerised provider order entry system (electronic version of paper order set).
Outpatient tests within the cancer centre are ordered using a separate electronic system called eSheet. Within eSheet, ordering providers enter tests by selecting from either a personal eSheet order group or test-by-test up to a maximum of 2 years into the future.
Intervention
The intervention was comprised of three main components: the creation of clinical guidelines, education alongside audit and feedback and system changes to the ordering process. We first set clinical practice recommendations for appropriate ordering of AST and BUN. We formed a committee of general internal medicine, nephrology, gastroenterology, laboratory medicine physicians, laboratory medicine technologists and trainees along with information technology experts. The team formalised clinical practice recommendations for appropriate indications of AST and BUN testing at our organisation (online supplementary appendix 2; tables 1 and 2).
Supplemental material
Explanation of clinical practice recommendations
In current practice, AST is primarily used to diagnose alcoholic liver disease by calculating the ratio to ALT.7 The American College of Gastroenterology Guidelines for the Evaluation of Abnormal Liver Chemistries suggest that an AST/ALT ratio of at least 2:1 is commonly associated with alcohol-mediated liver injury.6 Other uses of the AST are as a scoring tool for the assessment of hepatic fibrosis and to rule out advanced fibrosis.6 8 Regardless, for determining diagnoses in these clinical situations, only one AST result is necessary to calculate the ratio or score.
BUN levels may be helpful in confirming a diagnosis of acute kidney injury, to differentiate between prerenal acute kidney injury vs acute tubular necrosis, as a component in the decision to initiate dialysis, to calculate the osmolar gap in the context of acute poisoning and to aid in the diagnosis of an occult upper gastrointestinal bleeding.17 22–25 The utilisation of both tests for research purposes was considered an indication conditional on appropriate reimbursement to the laboratory. The clinical practice recommendations noted that physicians were able to add on AST or BUN by contacting the laboratory after a sample was drawn, if the clinical need arose.
Changes to ordering process
In November 2017, we removed AST and BUN from the outpatient laboratory requisition, although both tests could be ordered in a free-text section. Six months after this modification, the majority of outpatient offices were using the new requisition. From May to July 2018, we reviewed monthly outpatient laboratory requisitions to identify physicians using outdated laboratory paper requisitions, with feedback provided to the ordering physician. In February 2018, we removed BUN and AST from 20 hospital-approved shared order sets from within the electronic laboratory ordering system. In April 2018, AST and BUN were removed from eSheet personal order groups within the cancer centre outpatient electronic ordering system (figure 1D).
Academic detailing
Through April and May 2018, members of the committee met with stakeholders in top ordering areas (physicians, nursing staff and hospital administrators) and visited top ordering locations to investigate ordering practices. We identified a knowledge gap within the top 20 ordering physicians regarding appropriate indications for BUN and AST. We circulated clinical practice recommendations to the lead ordering physicians in highest ordering locations and individual high ordering physicians regardless of location. The staff were educated either individually with a committee member and/or through the hospital medical grand rounds in May 2018 with speakers from the committee. The grand rounds were highlighted on the hospital intranet launch page to encourage attendance. All staff working in the top 10 ordering locations as well as the top 20 ordering physicians were invited to these educational rounds focused on the Choosing Wisely Laboratory initiatives at our institution. The same presentation was delivered to clinical department chiefs at the Medical Advisory Committee who circulated the slides to their physician teams.
Audit and feedback
Audit and feedback were provided to the top 20 ordering healthcare professionals for educational purposes and to better understand why they were top users. Patient care managers and clinical department chiefs of top ordering locations were also given feedback on their monthly ordering data in May and June 2018 and were encouraged to circulate the updated guidelines to all physicians, nursing and clerical staff in their respective units.
Additional changes to the ordering process
We searched all paper order sets for: ‘liver profile’, ‘renal profile’, ‘urea’, ‘BUN’ and ‘AST’. We identified 51 order sets, which we adjudicated for appropriateness and revised in conjunction with clinical staff, through June to July 2018. Five order sets were deemed appropriate, 7 were no longer in use (archived), and 38 required revisions. One paper order set was not modified due to the refusal of a physician lead to work with the committee. After additional meetings and involvement of senior hospital leaders, the physician lead for this area agreed to remove the AST and BUN from the order set as a routine test for all patients on this particular ward. Of the identified paper order sets, 25 included the AST alone, 18 included the BUN alone and eight included both tests. AST and ‘liver profile’ were changed to ALT/ALP while BUN and ‘renal profile’ were changed to creatinine. Following approval from the Medical Advisory Committee, all personal order groups from within the electronic laboratory ordering system were disabled in July 2018.
Measures
We measured total number of AST, ALT, BUN and Cr tests on a monthly basis from January 2017 to August 2018. Data from September to December 2018 were included to monitor sustainability of utilisation efforts. We calculated AST/ALT and BUN/Cr ratios from these data. We tracked acute inpatient patient volumes to account for a change in test ordering due to a change in inpatient admission volumes. We calculated the cost per AST and BUN test from an estimate of consumable, reagent, analyzer and personnel costs (C$2.49 per test).
Statistical analysis
We used a general linear regression model to evaluate significant changes in test ordering. To control for multiple comparisons of AST/ALT and BUN/Cr ratios by ordering physician and location, the Bonferroni corrected p value <0.001 (alpha 0.05/50 tests) was considered statistically significant. We analysed the change in AST and BUN tests ordered using a run chart according to recommended guidelines.26
Results
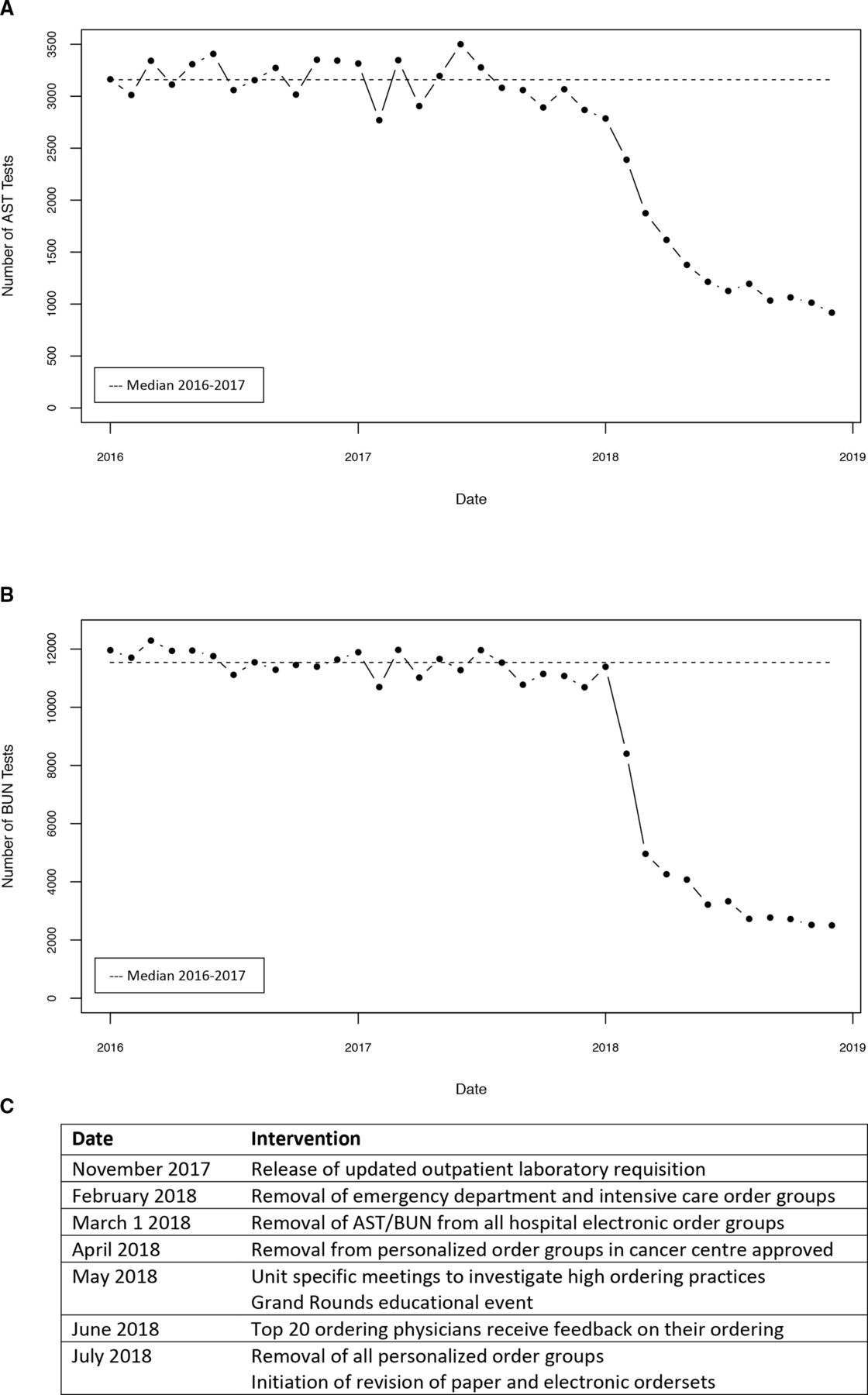
In the year preceding our study (2017), 37 275 AST and 101 264 ALT tests were performed (monthly median 3074 AST tests (IQR 2902–3287) and 8607 ALT (IQR 8270–8738)) and 135 694 BUN and 238 681 Cr tests were performed (monthly median BUN 11 211 tests (IQR 10 958–11 706) and Cr 20 308 tests (IQR 19 418–20 414)). The AST/ALT ratio for 2017 was 0.37 and the BUN/Cr ratio was 0.57. In 2017, 20 AST and 72 BUN tests were performed per 100 hospital days. The utilisation of AST and BUN was stable in the calendar year preceding our intervention (January 2017–January 2018, figure 2). The patient volume throughout the study period remained constant.

{kind=link}
{kind=link}
BUN orders from January 2016 to December 2018. (B) AST orders from January 2016 to December 2018. (C) Detailed intervention steps. AST, aspartate aminotransferase; BUN, blood urea nitrogen; ED, emergency department; ICU, intensive care unit; LCL, lower control limit; UCL, upper control limit.
The AST/ALT and BUN/Cr ratios changed from 0.37 in 2017 (95% CI 0.36 to 0.38) to 0.14 (95% CI 0.10 to 0.18, p<0.0001) in August 2018 and 0.57 (95% CI 0.56 to 0.58) in 2017 to 0.14 (95%CI 0.10 to 0.18, p<0.0001) in August 2018, respectively. Our goal to reduce the AST/ALT and BUN/Cr ratios to 0.05 was not achieved. Data from September to December 2018 (figure 2) shows continued sustainability of utilisation efforts.
The number of tests per 100 hospital days decreased to 7 AST and 17 BUN (95% CI 4.4 to 10.1, 16.6 to 22.9) tests performed (p<0.0001). We observed a decrease in monthly BUN and AST from 2786 AST and 11 391 BUN tests in January 2018 to 1195 AST and 2726 BUN tests in August 2018 (figure 2). We estimate an annualised cost savings of C$221 749 for 2018. The average monthly volume of hospitalised inpatient days was 15 772 in 2017 and 16 339 in 2018.
We completed exploratory subgroup analyses by location and top ordering clinicians and found significant decreases in almost all areas (online supplementary appendix 3; tables 1 and 2). We found that in the emergency department, the BUN/Cr ratio decreased substantially (0.92 to 0.04, 95% CI 0.92 to 0.93, 0.04 to 0.05, p<0.0001). The ICUs also fell in the AST/ALT, the largest being the main critical care unit (ICU-1) (0.53 to 0.08, 95% CI 0.52 to 0.55, p<0.0001). In both a smaller ICU (ICU-2) and the cardiovascular ICU, the BUN/Cr ratio also decreased (ICU-2: 0.76 to 0.04, 95% CI 0.61 to 0.90, −0.24 to 0.33, p=0.0003; cardiovascular ICU: 0.82 to 0.15, 95% CI 0.81 to 0.85, p<0.0001). We also observed a fall in the family practice AST/ALT ratio from 0.68 to 0.16 (95% CI 0.63 to 0.72, 0.002 to 0.31, p<0.0001). The general surgery ward increased in AST/ALT ratio from 0.51 in 2017 to 0.56 in June–August 2018 (95% CI 0.45 to 0.57, 0.43 to 0.69, p=0.39); the modification of multiple general surgery order sets was delayed till October 2018 after the measurement time period.
Supplemental material
Discussion
We conducted a quality improvement initiative using education, audit and feedback and order process interventions to reduce the unnecessary testing of AST and BUN within our healthcare institution. We observed a significant decrease in the ratio of AST/ALT from 0.37 to 0.14 and BUN/Cr from 0.57 to 0.14. We observed a decrease from 37 275 (3074 monthly median) AST and 135 694 (11 211 monthly median) BUN tests in 2017 to 1195 AST and 2726 BUN tests in August of 2018. Most locations decreased in laboratory test ordering, although we observed an increase in the AST/ALT ratio within the general surgery ward due to failure to implement order set modifications during the study time period. Ten order sets for patients on the general surgery ward required extensive changes to items other than the laboratory testing ordering section as they not been revised in over 5 years. Changes to these order sets came into effect in early 2019. Our study is unique in that it addressed two specific tests that are often ordered unnecessarily, with education that focused on the limited utility of the two tests rather than on the burden of cost that laboratory testing poses in general. The inclusion of audit and feedback was an important component giving the project relevance to ordering physicians and assisted with identifying previously unidentified system issues as the majority of orders were based on historical order sets and laboratory test order groups.
Numerous studies that have attempted to reduce laboratory testing by means of education alone reported that the effects of the intervention lacked durability once education was stopped.27 28 A previous study that implemented an educational intervention to address unnecessary creatine kinase (CK), lactate dehydrogenase (LDH) and thyroid function test ordering, while only modifying the request form for thyroid function testing, found a significant decrease in thyroid function testing (up to 60% decrease from baseline) with no effect on the CK and LDH tests (102% and 96% from baseline, respectively). This might suggest the importance of coupling system changes with education or that physician education alone is unlikely to provide sustained impacts.28
One of the top ordering locations of both tests was the ED. Due to its high volume of testing and patient volumes, others have studied interventions to reduce unnecessary laboratory testing in this setting.21 29 A recent study focused on reducing unnecessary coagulation testing using uncoupling routinely used standardised order panels into individual tests as part of the intervention. This change resulted in a significant decrease in the rate of coagulation testing per 100 ED patients (38.4% to 17.2%).21 In the context of our intervention, we learnt that a large proportion of tests were ordered routinely under medical directives by nursing staff prior to a physician seeing the patient. A previous study investigating whether triage nurse ordering correlated with emergency physician ordering found only a modest correlation between the two along with an estimated 34% of ‘over-ordering’ by triage nurses.30 In this study, after implementation of a set of guidelines, the percentage of over-ordering decreased by sevenfold.30 Our intervention resulted in decreases of both test ratios, in particular the BUN/Cr decreased from 0.92 in 2017 to 0.04 through June–August 2018. The significant decrease in testing within the ED was almost completely due to a removal of both tests from computer order groups. Prior to this study, AST and BUN were removed from the ED medical directive, though inadvertently remained in order groups within the electronic laboratory ordering system. The removal of these tests from the order groups therefore had the greatest impact on ordering, highlighting the importance of complete investigation of the ordering process when system changes are implemented.
Through discussions with staff working in different clinical areas, the heterogeneity of ordering behaviour between healthcare professionals became apparent. For example, family practice physicians may order more screening tests due to the nature of their field or concern for missing a diagnosis. The family practice unit at our institution was one of the highest AST ordering locations by number of AST tests ordered. We therefore added an educational component that included feedback tailored towards staff working in the unit. Similar approaches have been applied at other institutions using an audit and feedback intervention to improve the use of antibiotic prescribing in family practice, resulting in an over 30% reduction in unnecessary use of antibiotics in the intervention group compared with controls.31 We sent physicians their individual ordering data and helped set a plan for reduction. We observed a decrease in the AST/ALT ratio within the family practice of 0.68 in 2017 to 0.16 in August 2018. The unexpected high volume of AST ordering by the family practice unit highlights the importance of investigating practices and educating specialty areas separately due to potentially different perspectives on laboratory test ordering.
The greatest impact from our intervention on test ordering likely occurred due to the system changes that were implemented. Order sets provide structure in clinical settings; however, they also hard code practice by not allowing physicians to alter test ordering when unnecessary. Therefore, it is key that standardised order sets be routinely revised to mitigate the risk of test overutilisation. Many of the identified order sets were over 10 years old and had not been revised since their implementation.
Although we observed a large reduction in test ordering, we did not achieve our goal of 0.05 within the study period. We expect to see a further decrease from 0.14 as the process of altering order sets is lengthy and takes 3–6 months until the new versions become live on hospital units. In addition, several units initially refused to consider a change to their order sets due to either workload or strongly held beliefs that these two tests were necessary as a daily order. We continue to work to bring all hospital areas in line with the clinical practice recommendations for these two tests. We plan to re-evaluate reductions that occur from changes in these order sets. Alternatively, it is possible that the 5% threshold of appropriateness selected by the committee may not represent the true threshold of clinical appropriateness or that it will take greater efforts by the hospital Choosing Wisely committee to improve practice. The appropriateness of AST and BUN ordering in 2019 will be reanalysed to determine if the 5% can be achieved.
In 2017, the annual cost of AST and BUN testing at our institution was C$430 692. Through the reduction of AST and BUN ordering, the intervention resulted in a projected annual cost savings of C$221 749. These substantial cost savings are valuable within a public healthcare system as they can potentially be reallocated to more appropriate testing or treatments. In addition, reducing laboratory test volumes may have a positive impact on laboratory test throughput improving efficiencies in patient management.
Strengths and limitations
Our study had several strengths. We involved multiple stakeholders: physicians, patient care managers, nurses, nurse practitioners, department chiefs, clerical staff, information technology staff, phlebotomists and laboratory technologists, allowing us to generate an intervention with a broad and sustained impact. We utilised multimodal change strategies, with findings based on a large sample size.
Our study had several important limitations. This is a single institution study. The 5% level of clinical appropriateness was chosen a priori by the committee based on expert opinion and therefore may not necessarily be achievable. Patient audits and chart review may be useful in determining the residual proportion of unnecessary tests. Our laboratory system only tracks tests ordered under the name of the attending physician or nurse practitioner regardless of whether the decision to order was made by a medical student, resident, clinical fellow, nurse or ward clerk. We may have missed opportunity for education and system changes among these groups. Since outpatient physicians were able to order testing in advance, despite changes in ordering habits, for a period of time some tests may continue to be ordered inappropriately, potentially reducing the impact of the intervention in the short term. For example, in the cancer centre, physicians are allowed to preorder tests for up to 2 years. The process of revising the order sets is lengthy and will take approximately 3 months until new order sets are in use and approved by the order set committee. Consequently, the true impact of our intervention may not be realised until 1 year after all changes have been made. This intervention addresses only one small component of overall healthcare expenses. The importance of unnecessary laboratory testing should not be underestimated, as it is a problem that impacts all hospitals and can be easily addressed with systemic changes.
Conclusion
The ordering of unnecessary laboratory tests is common in our healthcare system leading to considerable costs. By addressing system issues that improved the physician and nursing compliance with clinical practice guidelines for laboratory tests, along with educational interventions coupled with audit and feedback, we achieved a marked decrease in AST and BUN testing at our institution with an estimated cost savings of over C$220 000. Our systematic approach could be readily applied to other healthcare institutions leading to considerable healthcare cost savings.
References
Footnotes
Contributors RS, AC, CMC, PT, AZ, JC, AW, EE and JR planned and carried out interventions. SW extracted data from the laboratory information system. RS and JC performed data analyses. RS, AC and JC wrote the manuscript with input from all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are available upon reasonable request.