Article Text

Abstract
Background Substantial evidence demonstrates comparable cure rates for oral versus intravenous therapy for routine osteomyelitis. Evidence adoption is often slow and in our centre virtually all patients with osteomyelitis were discharged on intravenous therapy.
Objective For patients with acute osteomyelitis admitted to the hospital medicine service, we aimed to increase the proportion of cases discharged on oral antibiotics to at least 70%.
Methods The setting for our observational time series study was a large academic children's hospital. The model for improvement and plan-do-study-act cycles were used to test, refine and implement interventions identified through our key driver diagram. Our multifaceted intervention included a shared decision-making tool, an order set in our electronic health record, and education to faculty and trainees. We also included an identify and mitigate intervention to target providers caring for children with osteomyelitis in near-real time and reinforce the evidence-based recommendations. Data were analysed on an annotated g-chart of osteomyelitis cases between patients discharged on intravenous antibiotics. Structured chart review was used to identify treatment failures as well as length of stay and hospital charges in preintervention and postintervention groups.
Results The osteomyelitis cases between patients discharged on intravenous antibiotics increased from a median of 0 preintervention to a maximum of 9 cases following our identify and mitigate intervention. The direction and magnitude of successive improvements observed satisfied criteria for special cause variation. Improvement has been sustained for 1 year. Treatment failure and complications were uncommon in preintervention and postintervention phases. No significant differences in length of stay or charges were detected.
Conclusions Even for uncommon conditions, rapid and sustained evidence adoption is possible using quality improvement methods.
- Antibiotic Management
- Continuous Quality Improvement
- Paediatrics
- Decision Making
- Evidence-Based Medicine
Statistics from Altmetric.com
- Antibiotic Management
- Continuous Quality Improvement
- Paediatrics
- Decision Making
- Evidence-Based Medicine
Introduction
Osteomyelitis is a bacterial infection of the bone that accounts for approximately 1% of all paediatric hospitalisations and affects 1 of 5000 children less than 13 years of age in the USA each year.1 ,2 Traditionally, treatment of acute haematogenous osteomyelitis, the most common form of childhood osteomyelitis, has consisted of initiating antibiotic therapy intravenously in the hospital followed by 4–6 weeks of outpatient parenteral antibiotics administered through a central catheter.3 However, more recent studies have shown that home oral antibiotic therapy for routine, uncomplicated acute haematogenous osteomyelitis is equally effective.4 ,5 In addition, oral treatment avoids the risk of catheter-associated complications such as malfunction, displacement, infection at the insertion site or blood stream infection.6 In our institution, this new evidence had not been adopted into widespread practice.
The purpose of this quality improvement project was to increase the proportion of patients with acute haematogenous osteomyelitis admitted to the hospital medicine service who were discharged on oral antibiotics within 120 days.
Methods
Setting
Cincinnati Children's Hospital Medical Center (CCHMC) is a large, free-standing, quaternary care children's hospital with 523 beds and over a million patient encounters per year. At this project's start, 23 attending physicians supervised and trained 180 paediatric residents and 180 medical students annually on the hospital medicine service. Approximately 20 patients per year diagnosed with acute haematogenous osteomyelitis are admitted to the hospital medicine service. At the project's start, most of these patients were managed with consultations from infectious diseases and orthopaedics. Patients who were discharged with peripherally inserted central catheters (PICC) lines were managed through the Outpatient Antibiotic Therapy service run by the Division of Infectious Diseases. We did not have set discharge criteria for patients with osteomyelitis when this project began, but these criteria now include no fevers for 24 h, inflammatory markers trending down, antibiotic regimen confirmed and pain well controlled with oral medications. CCHMC has a history of implementing quality improvement and evidence-based guideline initiatives. This work was the first project for the newly established Rapid Evidence Adoption to improve Child Health (REACH) core at CCHMC.7–9 The aim of REACH is to decrease the time to reliable adoption of evidence.
Planning the intervention
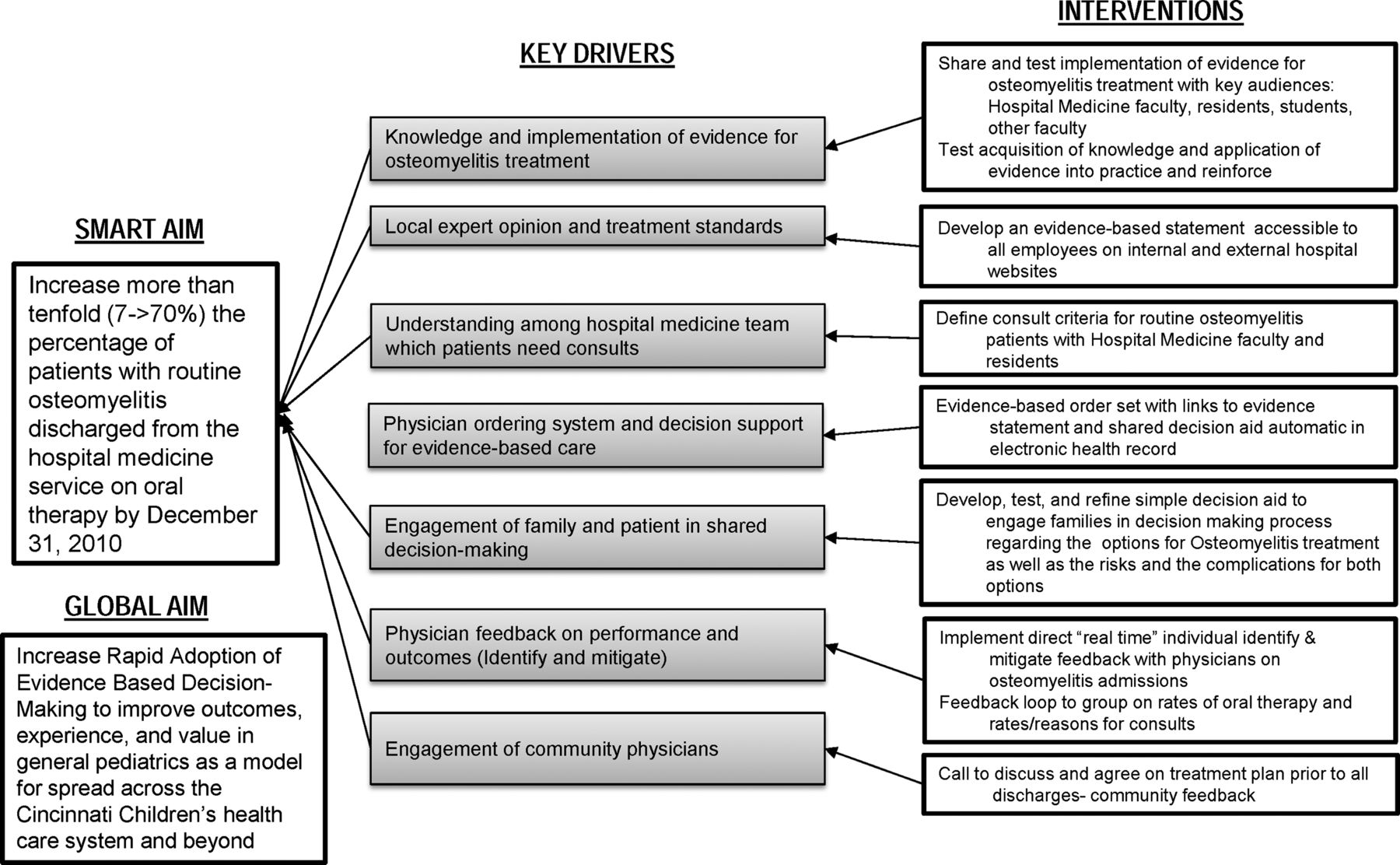
Our specific aim was to increase rapidly to >70% the percentage of patients with routine osteomyelitis discharged from the hospital medicine service on oral therapy. Our team identified seven key drivers for rapid adoption of evidence-based care for routine osteomyelitis (figure 1): (1) knowledge and implementation of evidence for osteomyelitis treatment, (2) standardised treatment protocols, (3) understanding need for consultations, (4) electronic decision support and ordering system, (5) family and patient engagement, (6) physician feedback and (7) community physician engagement. Our improvement team, which included several members with previous experience with evidence adoption, determined the key drivers through a series of discussions. The drivers represented the theorised concepts, to be tested in interventions, which our team believed needed to be in place to meet our aim. We targeted most of these key drivers with four improvement activities: (1) education to hospital medicine faculty, residents and students, (2) a process, we term ‘identify and mitigate,’ where a research assistant used the electronic health record to identify patients with potential osteomyelitis and then contacted the faculty and residents caring for the patient to remind the providers about decision support tools to promote evidence adoption, including, (3) a shared decision making (SDM) tool to engage patients and families in decision and (4) a computerised order set linked to an evidence statement.
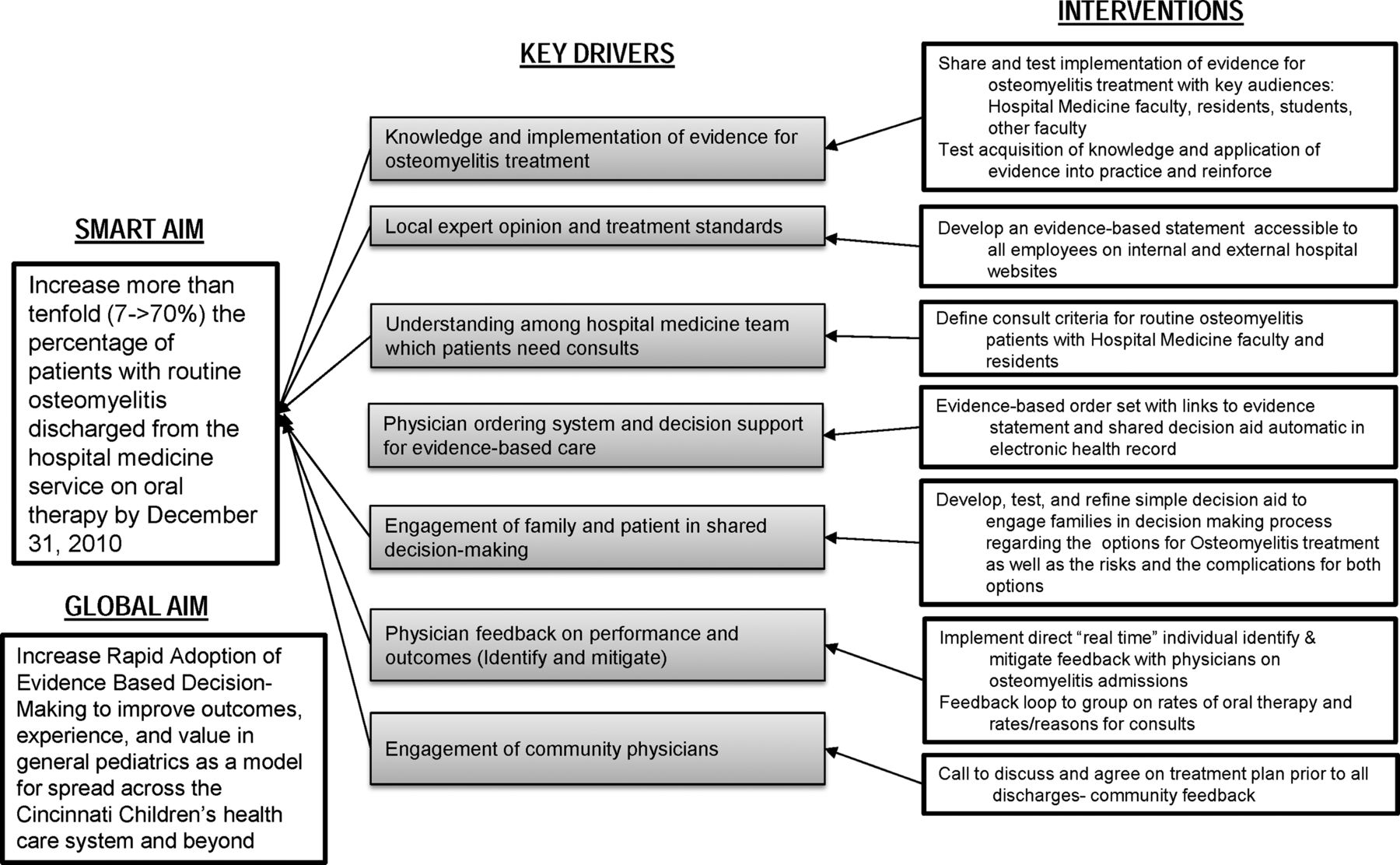
Key driver diagram illustrates the drivers and individual interventions through which our team worked to meet our specific aim.
Improvement activities
Education
Beginning in May 2010, hospital medicine faculty members were educated on the evidence and application of early transition to oral antibiotic therapy. Sessions were interactive and prompted group discussion about current practice patterns and desired future practice patterns including when consultation with infectious diseases or orthopaedic specialists was indicated. We did not have formal indications for consultations. Consultations were generally indicated for infectious disease specialists’ expertise on differential diagnosis and antibiotic choice and duration and for orthopaedic specialists’ expertise on diagnosis and procedures. In July and August 2010, education was spread to the remaining hospital medicine faculty members. In September 2010, a group of paediatric residents and medical students on their inpatient rotations received the same education in a morning report conference. Later, in December 2010, emergency medicine faculty and fellows were educated.
In February 2011, a Hospital Medicine team developed an evidence-based statement recommending that “transition from intravenous to oral antibiotic therapy be considered within the first 7 days of treatment for haematogenous osteomyelitis” and that “the clinician discuss the risks and benefits of short versus prolonged intravenous therapy with families.” The statement was accessible to all employees on the hospital website.
Identify and mitigate
Beginning in November of 2010, a trained research assistant reviewed the electronic health record system each weekday for new osteomyelitis admissions. Because the diagnosis of osteomyelitis is not always confirmed at the time of admission, patients with chief complaints related to osteomyelitis such as bacteraemia, limp, cellulitis and limb pain were also reviewed. Upon review, if physician progress notes or radiology reports indicated probable osteomyelitis, the research assistant contacted the physician team by email. The email message contained reminders about the evidence for early transition to oral antibiotics and existence of the osteomyelitis order set, the SDM tool and the evidence statement. If the research assistant was unsure of a patient's eligibility, a physician on the study team reviewed the chart for confirmation. The identify and mitigate process allowed for data collection in near-real time. These data were then shared with the hospital medicine faculty through a feedback mechanism. The every weekday identify and mitigate process ended in February 2012.
Shared decision making tool
A shared decision aid was developed by project team members with expertise in SDM (WBB) and evidence-based treatment of osteomyelitis (PHC) using a proven format.10 The decision aid summarised the options for osteomyelitis treatment and potential risks and complications of oral and intravenous antibiotics in plain language at a 6th grade reading level. The decision aid was designed to prompt a discussion between members of the child's family and healthcare team about the option the family preferred. In December 2010, we tested the decision aid with two eligible patients with osteomyelitis, eliciting feedback from parents and physicians following decision aid use. Feedback was universally positive with no revisions suggested. Beginning in January 2011, physicians were encouraged to use the decision aid to engage patients and families in SDM (see online supplementary figure S1). The decision aid described in this article and further information on its development are available in the public domain free of charge at: http://www.cincinnatichildrens.org/shareddecisions.
Order set
An osteomyelitis order set was developed and implemented in March of 2011 in the electronic health record system. Hyperlinks to the evidence statement and the SDM tool were embedded in the order set, as were reminders on recommendations for providers to discuss treatment options with patients and/or families and to consider early transition to oral antibiotics.
Identification of eligible subjects
We aimed to include a strictly defined cohort where the best evidence existed regarding the effectiveness of oral therapy. In preintervention and postintervention phases, inclusion and exclusion criteria mirrored those employed by the studies establishing the efficacy of oral antibiotics in the treatment of acute haematogenous osteomyelitis. Patients eligible for inclusion were otherwise healthy children between 2 months and 18 years of age admitted to the hospital medicine service with the diagnosis of acute haematogenous osteomyelitis. Patients were excluded if they had specific comorbid conditions (congenital and acquired immunodeficiency, sickle cell disease, trauma or osteomyelitis associated with immobilisation or pressure ulcers), postsurgical osteomyelitis, concurrent septic arthritis, osteomyelitis of the head, face, and orbits, complicated osteomyelitis requiring multiple surgical procedures, or required more than 7 days of intravenous antibiotic therapy in the hospital.
Preintervention baseline data (from July 2009 to April 2010) was obtained through retrospective chart review of patients generated from a report containing all patients with International Classification of Diseases, ninth revision, Clinical Modification discharge codes for osteomyelitis (730.0–730.19 and 730.2–730.29). Post intervention (from May 2010 to July 2012), every patient identified by the research assistant was recorded in an Excel (Microsoft, Redmond, Washington, USA) spreadsheet. To verify the accuracy of data from the postintervention period, we conducted a retrospective chart review using the same International Classification of Diseases, ninth revision, Clinical Modification codes used to identify the preintervention baseline data.
Outcome assessment
Hospital medicine faculty members, residents and medical students completed a survey before and after the interactive education sessions to assess knowledge and practice behaviour intentions for the medical treatment for a patient with acute haematogenous osteomyelitis described in a clinical vignette. This assessment asked respondents to report on a 5-point Likert scale how likely they typically (pre-education questions) and how likely they were in future (posteducation questions) to: (1) consult infectious disease, (2) consult orthopaedics, (3) treat with long-term intravenous therapy and (4) engage the patient and family in the treatment decision.
For our observational time series study, we performed medical record audits, conducted following patient discharge, for assessment of the following outcomes: procedures during hospital stay, mode of antibiotic therapy ordered at discharge, return to emergency room, readmission for osteomyelitis, PICC complication within 6 months of index hospitalisation, length of hospital stay (LOS) and charges. Charges included those from index admission as well as home health charges and any returns to our emergency department (ED) or hospital. We included LOS as a balancing measure to ensure that physicians were not keeping patients longer due to any perceived belief that oral antibiotics may be less effective.
Analysis
For pre-education and posteducation survey data, the percentage of respondents answering ‘usually’ or ‘almost always’ were calculated for the prequestions and postquestions. These were quantitatively anchored on the survey tool as 75–94% and 95–100%, respectively. Paired presurvey and postsurvey results were compared using the Wilcoxon signed-rank test. Frequency of infectious disease and orthopaedic consultations in the preintervention and postintervention phases were compared using the Fisher's exact test. Analysis of the primary outcome of proportion of patients discharged on oral therapy was performed using a run chart. The research assistant recorded data and created an annotated run chart using Microsoft Excel to assess the impact the interventions had on the outcome measure over time. Our improvement team used a run p-chart with month as the x-axis and percentage of eligible patients discharged on oral antibiotics as the y-axis. Established rules for identifying special cause were employed.11–13 As many months had only one eligible patient, we used a g-chart for our primary analysis. A g-chart or cases-between chart plots the number of cases between a particular outcome.14 ,15 We plotted the number of cases of eligible patients admitted with osteomyelitis between each eligible patient discharged on intravenous antibiotics. We calculated the upper confidence limit using established calculations for a geometric distribution (where gbar=average of cases between, upper limit=gbar+3 × (square root (gbar × (gbar+1)))).15
Counts for postdischarge outcomes were stratified by preintervention versus postintervention phases. No statistical analysis was conducted as our study was not powered to detect a clinically significant difference in these uncommon outcomes. Charge data in preintervention and postintervention periods were compared using t tests. Skewed length of stay data was transformed using the natural logarithm. We used SAS V.9.3 (SAS Institute, Cary, North Carolina, USA) for analysis of the survey, length of stay and charge data.
Human subjects protection
The CCHMC institutional review board reviewed the project and considered it to not be research involving human subjects. Informed consent beyond the standard consent for treatment for all inpatients was not required.
Results
Preassessment and postassessment surveys were completed by 12 hospital medicine faculty and 53 residents and medical students. Seven of the attending physicians had 0–4 years of experience, four had 5–9 years of experience and one did not complete this section. The 53 residents and students included 11 3rd-year students, 5 4th-year students, 22 interns and 14 senior residents. The questions for experience, typically treat with long-term intravenous and typically engage family in decision, each had incomplete data for one respondent in the resident/medical student group. In both groups significant changes in expectations were found in pre-education versus posteducation use of long-term intravenous antibiotics and family engagement in decision. The residents and students but not hospital medicine attending physicians had significantly reduced pre-education versus posteducation expectations to consult infectious diseases and orthopaedics (table 1).
Pre-education and posteducation survey results for hospital medicine faculty group (n=12) and residents and medical students (n=53) who completed an interactive educational session on the evidence on the early transition to oral therapy for routine osteomyelitis
A total of 9 eligible patients were admitted during the preintervention phase and 22 eligible patients were admitted during the postintervention phase. The percentage of children with osteomyelitis discharged on oral therapy increased from a median of 0% to 100% within 1 month and has been sustained for over 1 year (figure 2). The cases-between patients with osteomyelitis discharged on intravenous antibiotics were zero in each case preintervention and were two, six, nine and zero in the postintervention period (figure 3). One point occurred outside the upper confidence limit and met special cause criteria to indicate a significantly changed process. The upper control limit and the median were calculated based on the entire data set (the preintervention and postintervention data). This was done as the calculated preintervention upper confidence limit was 0 since each cases-between data point was 0 preintervention, and we do not believe that this was an accurate threshold to determine special cause variation.

Annotated run chart showing percentage of eligible patients with acute osteomyelitis discharged home on oral antibiotics by month.

{kind=link}
{kind=link}
{kind=link}
Annotated g-chart showing count of osteomyelitis cases-between patients with osteomyelitis that were discharged on intravenous antibiotics. Note that median and control UCL were calculated based on preintervention and postintervention cases between data. IV, intravenous, UCL, upper control limit.
Once the identify and mitigate intervention began, all patients were found in near-real time (within 1–2 days) through its process. For each of the five patients discharged home with intravenous therapy in the postintervention phase, the research assistant shared the evidence statement with the attending physician, who in consultation with specialists chose intravenous therapy at discharge. In one case, all of the physician teams felt oral therapy on discharge was a reasonable choice, but after use of the shared decision aid, the patient's mother decided the 3 year-old would be unable to tolerate the bitter taste of oral clindamycin. Table 2 describes the patients in the preintervention and postintervention phases by demographic characteristics, site of infection, causative organism, type of antibiotic therapy at discharge, and any procedures that were performed during the index admission. With one exception, all patients were prescribed antibiotics for 4–6 weeks at discharge. One patient in the postintervention group was discharged on 6–8 weeks of oral cefadroxil. All patients were instructed to follow-up with their primary care physician. Infectious disease follow-up was arranged for patients who were seen by infectious disease during index admission but not those where the specialists were not consulted.
Demographics, diagnostic testing, procedures and antibiotics given at discharge for pre and post groups
Infectious disease consultations were placed less commonly in the postintervention (9/22, 41%) period compared with the preintervention (8/9, 89%) period, although this did not meet statistical significance (p=0.11). The frequency of orthopaedic consultations was similar in postintervention (19/22, 86%) and preintervention (8/9, 89%) phases. While it was not part of the initial change package, in October of 2012 leadership of hospital medicine and infectious diseases agreed that patients with acute haematogenous osteomyelitis would have routine infectious diseases consultation. If there was disagreement about the proper route of therapy at discharge, there was to be an attending to attending conversation.
In the preintervention phase, all nine patients were discharged home with a PICC line and intravenous antibiotics. In the 6 months following discharge, one patient returned to the ED for a non-infectious PICC complication that did not result in readmission. In the postintervention phase, 17 patients received oral antibiotics and 5 intravenous antibiotics at discharge. In the following 6 months, five patients had noteworthy events. One patient on oral antibiotics was readmitted for an incision and drainage procedure and nail-bed removal by plastic surgery of the finger with previously diagnosed osteomyelitis. This patient was discharged home on oral antibiotics. A second patient on oral antibiotics was readmitted twice due to an abscess around the site of his osteomyelitis but not within the bone. This patient had culture-negative navicular bone osteomyelitis. He was treated with clindamycin, and he improved during admission. On readmission his abscess was incised and drained and grew Pseudomonas aeruginosa. This patient was eventually sent home on oral antibiotics and was treated for 4 months. Two patients had ED visits that did not result in admission. One patient on oral antibiotics was seen for an unrelated upper respiratory infection while one patient with a PICC line was seen for a non-infectious PICC complication. Another patient returned to infectious diseases clinic for a rash around the PICC insertion site.
Hospital charges and LOS were similar in preintervention and postintervention groups (charge medians of $23 740 vs $25 264, LOS medians of 3.8 days in both). Neither difference was statistically significant.
Discussion
Our bundled improvement intervention increased the osteomyelitis cases between patients with osteomyelitis discharged on intravenous antibiotics. This practice change has been sustained for over 1 year. We used the Model for Improvement and reliability principles to test, scale and implement into clinician work flow broad educational efforts, a decision aid for use with families, an osteomyelitis order set in our electronic health record, and a daily identify and mitigate process.16 Our educational intervention decreased the percentage of resident, medical student and attending respondents that anticipated typically treating with long-term intravenous antibiotics and increased the percentage of respondents who expected to engage the family in the decision. Residents and medical students responded that they were less likely to consult infectious disease and orthopaedics after the education. Overall rates of complications of osteomyelitis and those related to PICC lines were uncommon in the preintervention and postintervention groups. This project is one of four of the REACH core with the aim to reduce the time to reliable adoption of evidence.7–9 Each project used education and evidence statements to build consensus among the multidisciplinary team. Electronic order sets and a process to identify and mitigate cases were associated with success in most projects. This set of interventions is worthy of testing in other organisations and settings.
We achieved significant and sustained improvement through a series of interventions that were tested and implemented into our care process within a 7 month period of time. While our study design does not allow us to speak with confidence to the independent or bundled effect of our different interventions, our results are consistent with reliability science.17 Our education intervention was important in presenting and discussing the evidence with physicians and likely facilitated the success of the identification and mitigation intervention that was delivered through email. As expected, however, with an education intervention the process was not highly reliable and a failure occurred after two successes. Continued success with education only would have been more difficult as new projects competed for the attention of the physicians involved. The more reliable identify and mitigate intervention provided a mechanism to provide the evidence and tools to the clinical team in near-real time. We then were successful in 6 and then 9 straight cases, corresponding to a 15/16 or 93% success rate and reflecting the level 2 reliability (or 10−2 failure rate) of the identify and mitigate process.17
The magnitude of this practice change is noteworthy. Zaoutis et al4 describe broad and significant variation in care of children with osteomyelitis between 29 children's hospitals, with 10% of children being sent home on oral therapy at one hospital and 95% at another. In our study period, our sample moved from the lowest to the highest in this range. Our pace of evidence adoption within 120 days represented a markedly increased rate compared with historical norms.18 Evidence-based clinical practice guidelines have been used for over a decade to promote standardisation and accelerate adoption of evidence. To date these have been most used and have been most successful with more common diseases, such as bronchiolitis and asthma and delivered significant changes over a time course of 1–2 years.19–23 More recent studies have examined the effect of evidence-based clinical practice guidelines combined with an antimicrobial stewardship programme on prescribing practice for patients hospitalised with community-acquired pneumonia.24 ,25
One challenge for the hospital medicine service to adopt new evidence for children with acute haematogenous osteomyelitis was the fact that our infectious diseases specialists, who were frequently consulted at baseline, rarely recommended treatment with oral antibiotics. The study team did directly engage the infectious disease service leadership in a discussion of the new evidence, but no consensus was achieved. Decreased consultations of infectious diseases were not an explicit goal of this project, but we observed an expectation for decreased consultations after education and a decreased number of consultations in practice. We believe there are two likely causes for this. First, hospital medicine physicians may have felt more confident in the evidence-based management for routine osteomyelitis. Second, the hospital medicine physicians may have believed the infectious disease group would recommend prolonged intravenous therapy, leading to tension and confusion for team and family. Infectious disease consultation has been associated with improved outcomes in Staphylococcus aureus bacteraemia which 17 of our 31 patients had.26 ,27 We believe infectious disease consultation and follow-up is valuable for patients with invasive infections such as osteomyelitis. We are currently refining our system to reliably consult infectious disease colleagues in these cases. One effect of these tests may be spread of our interventions to patients cared for by community-based physicians, although we are not testing interventions presently.
Being transparent about the evidence and eliciting parent preferences for intravenous versus oral treatment was viewed as an ethical imperative. We used a decision aid to facilitate shared decision making between parents and physicians. To our knowledge, this is the first study to implement such an intervention in the care of a hospitalised child. While there are relatively few examples of decision aids in paediatrics,28–34 there is strong evidence from adult medical settings that use of decision aids leads to patients who are better informed, more involved in choosing and less conflicted about the choice.35 Provider motivation is the most commonly reported facilitator of SDM.36 This may have played a role in the success of our intervention as the decision aid was implemented in a setting where family-centred care is highly valued.37 Family-centred rounds, standard practice at our institution for the past decade, increase parent participation in discussions with the medical team.38 ,39 Decision aids provide an evidenced-based approach to structure parent participation during family-centred rounds. Opportunities exist to apply this approach to other decisions with multiple medically reasonable options.
Given our aim to promote a change in antibiotic delivery, we felt it was important to assess that patients transitioned to oral therapy were not at increased risk for complications. We found no evidence of this. We were able to assess complications related to an ED visit or readmission, but we did not have complete follow-up data and may have missed complications if the child did not return to our hospital. This study has additional limitations. Our interventions, including the identify and mitigate process, targeted patients who were admitted to the hospital medicine service only. Patients admitted to the community physician service or to the orthopaedic service were ineligible for the study, and it is uncertain how effective our intervention would be in this group of patients. Our time series study design also limits our ability to determine which of the intervention components drove improvements in outcome. The process of care for postintervention patients was not observed directly, so it is impossible to discern which components of the intervention influenced care for individual patients. Finally, the identify and mitigate process was resource-intensive and may not be applicable in settings with more limited resources.
Conclusions
Employment of high reliability improvement science methods enabled the successful and rapid implementation of an evidence-based guideline that promoted the use of oral antibiotics in routine osteomyelitis in children on a hospital medicine service. These methods can be applied to other clinical conditions to foster rapid change in practice.
Acknowledgments
The authors would like to thank Suzanne Campanella for her assistance with chart review and drafting of figures and Shelly Miller for her work with data collection and the identify and mitigate intervention. We would like to thank Dr Srikant Iyer and Dr Lloyd Provost for their assistance in appropriate use of a g-chart when the preintervention cases-between mean was 0.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors PWB had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. He contributed to the conception and design of the study and performed the analysis and interpretation of data. He drafted the initial manuscript and contributed in its revision for important intellectual content. WBB contributed to the conception and design, analysis and interpretation of data, drafting of the initial manuscript and its revision for important intellectual content. JMS contributed to the initial conception and design of the study as well as the analysis and interpretation of the data. He also reviewed and edited the manuscript for important intellectual content. CY contributed to acquisition, analysis and interpretation of data. She drafted sections of the initial methods and results section of the manuscript and reviewed the entire manuscript for important intellectual content. CMW contributed to analysis and interpretation of data and reviewed the manuscript for important intellectual content. ESK has made substantial contribution to the intellectual content of the project by assisting with the analysis and interpretation of data, the drafting and critical revision of the manuscript itself and by contributing technical assistance in the implementation of the study's electronic health record-based interventions. JKS contributed to the analysis and interpretation of data and contributed to the manuscript for important intellectual content. PHC led the conception and design of the study. He contributed to the analysis and interpretation of data and revision of the manuscript for important intellectual content. MTV contributed to the design of the study and had access to all of the data in the study. He contributed to the initial manuscript, its intellectual content and its final revision.
-
Competing interests WBB is supported by Award Number K23MH083027 from the National Institute of Mental Health.
-
Ethics approval Cincinnati Children's Hospital Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement We have presented our best data in this submission and do not believe we have additional data of interest to your readership. We do have supporting materials related to shared decision making on our public website (http://www.cincinnatichildrens.org/shareddecisions) that is referenced in the manuscript text.