Article Text

Abstract
Background Suboptimal communication within healthcare teams can lead to adverse patient outcomes. Team briefings were previously associated with improved communication patterns, and we assessed the impact of briefings on clinical practice. To quantify the impact of the preoperative team briefing on direct patient care, we studied the timing of preoperative antibiotic administration as compared to accepted treatment guidelines.
Study design A retrospective pre-intervention/post-intervention study design assessed the impact of a checklist-guided preoperative team briefing on prophylactic antibiotic administration timing in surgical cases (N=340 pre-intervention and N=340 post-intervention) across three institutions. χ2 Analyses were performed to determine whether there was a significant difference in timely antibiotic administration between the study phases.
Results The process of collecting and analysing these data proved to be more complicated than expected due to great variability in documentation practices, both between study sites and between individual practitioners. In cases where the timing of antibiotics administration was documented unambiguously in the chart (n=259 pre-intervention and n=283 post-intervention), antibiotic prophylaxis was on time for 77.6% of cases in the pre-intervention phase of the study, and for 87.6% of cases in the post-intervention phase (p<0.01).
Conclusions Use of a preoperative team checklist briefing was associated with improved physician compliance with antibiotic administration guidelines. Based on the results, recommendations to enhance timely antibiotic therapy are provided.
- Collaborative
- communication
- patient safety
- surgery
- teamwork
Statistics from Altmetric.com
Introduction
Each profession has distinct roles and responsibilities on the healthcare team. Patient safety depends on the coordinated care provided by multiple healthcare professionals. Communication and teamwork are important aspects of ensuring patient safety,1 2 and communication breakdown is the most frequent cause of adverse events across all healthcare settings.3–5
Organisations that face intrinsic hazard but perform successfully do so by systematically addressing safety issues.1 For example, race car crews6 and the aviation industry7 8 are organizations that face extreme risk, but they manage this risk through systematic processes and routine communications. In medicine, efforts to implement and evaluate such systems are growing.7 9–11 The use of a preoperative ‘time out’ before every surgical procedure has become increasingly mandated, and recently the WHO has launched a worldwide patient safety initiative based on a one-page operative checklist.12–15 Given the increasing emergence of such initiatives, we urgently require empirical evidence of the relationship between altered communication routines and clinical practice in order to support decisions regarding widespread implementation.
We implemented a systematic inter-professional preoperative team briefing in the operating room. This checklist-guided briefing was previously associated with a decline in communication failures in the operating room,2 and the goal of this study was to assess whether this impact would replicate in a large-scale, multi-institutional design and whether the checklist briefing had an impact on clinical practice. The timing of prophylactic antibiotic administration was used as an outcome measure to test the team briefing's impact on a well-established patient care variable, based on the evidence of an association between properly timed antibiotic prophylaxis and lower rates of surgical site infection.15–25 Antibiotic administration timing is an important outcome to measure, and additionally acts as an indicator of the checklist briefing's potential for changing clinical practice.
Methods
Setting and participants
This multi-institutional study was conducted in the operating rooms of three Toronto-based research and teaching hospitals. Each surgical centre managed between 10 and 26 operating rooms each week day and performed between 18 500 and 33 265 inpatient and outpatient surgical procedures yearly. All general surgery procedures scheduled during the study period were eligible for inclusion in the study. Approval for the study was granted by the research ethics board of the Hospital for Sick Children, Toronto, Ontario, Canada, and by the research ethics boards of all local study sites. Consent was obtained from all participating members of the operating room team on an ongoing basis as new team members entered the operating room throughout the study. In total, 11 general surgeons, 48 surgical residents and fellows, 87 operating room nurses, 3 nursing trainees, 60 staff anaesthesiologists, 26 anaesthesia residents and fellows, 3 respiratory therapists and 5 technical assistants participated in the study. Three staff members withdrew from the study, providing a participation rate of 98.8%.
Study design and intervention
The data presented in the current paper, which is specifically attending to the timing of prophylactic antibiotic administration, were collected in the context of a larger study that used a pre-intervention/post-intervention design, with the implementation of both pre-intervention and post-intervention data collection phases staggered across the study sites. In each site, pre-intervention consisted of a number of months of observation, followed by a period of briefing implementation and feedback to promote uptake of the intervention, followed by post-intervention observations. The data on the timing of prophylactic antibiotic administration presented here, however, were collected using a retrospective design, such that chart review of antibiotic timing for post-intervention and pre-intervention cases was performed simultaneously at the end of the post-intervention observation period, While post-intervention charts were selected based on the observed use of a team checklist, pre-intervention chart selection was based on criteria (described below) designed to facilitate the comparison of pre-intervention and post-intervention antibiotics practices rather than on specific efforts to use the charts of the cases observed in the pre-intervention phase of the study.
Using the baseline estimate of 60% timely antibiotic administration established by Classen et al16 and Silver et al,26 it was calculated that a sample of 600 pre-intervention and 600 post-intervention cases was needed (α of 0.05, and a power of 0.80). Part way through the data collection, a preliminary analysis was performed and it was determined that a sample of 300 pre-intervention and post-intervention cases would be sufficient to detect a significant increase in the proportion of cases with timely antibiotic prophylaxis.
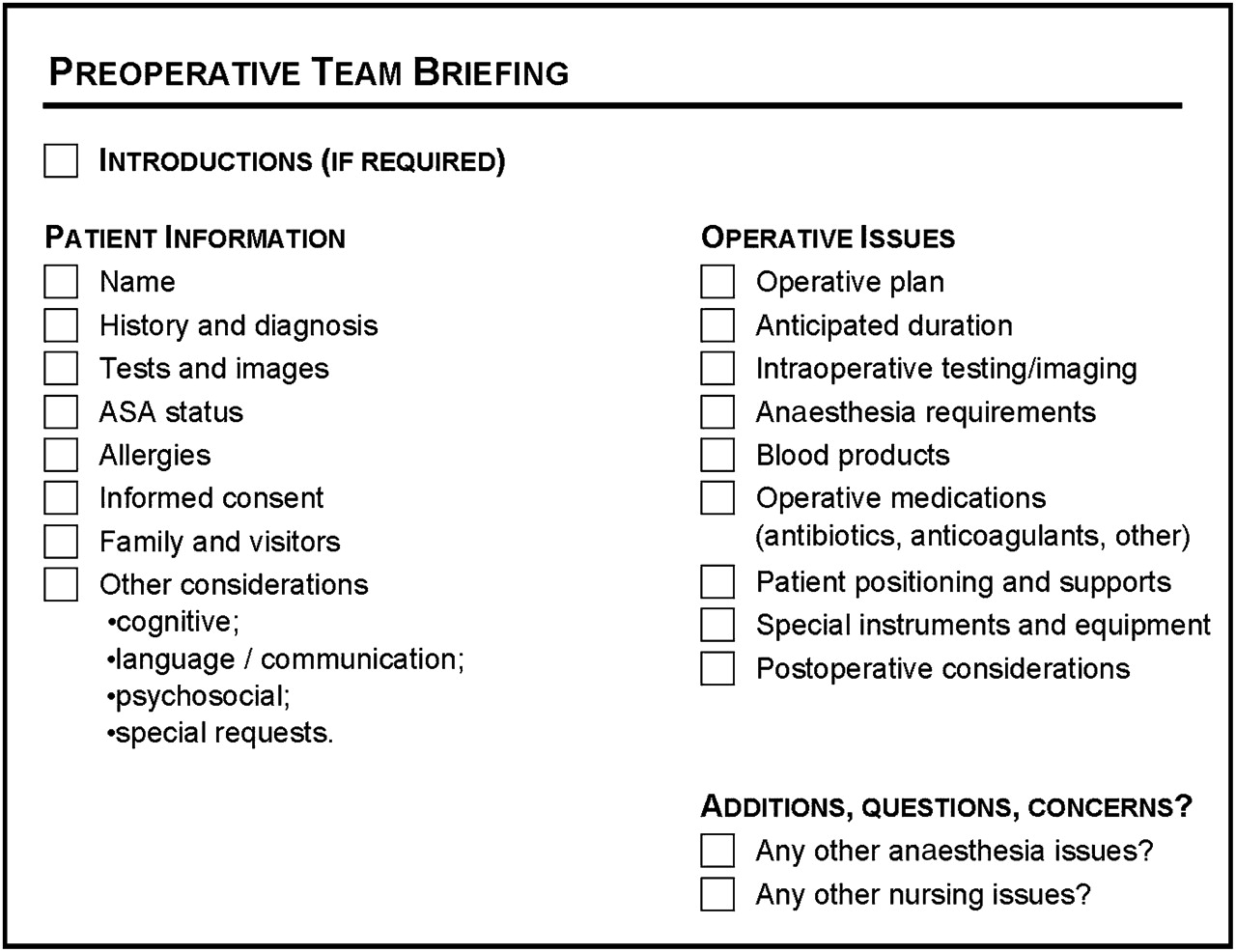
As previously described,2 the intervention involved the execution of a preoperative team briefing before the surgical procedure. During each team briefing, surgeons, nurses and anaesthesiologists gathered in the operating room for a discussion of the upcoming procedure and patient. Briefings tended to be led by staff or resident surgeons, although not exclusively. The briefing was intended to allow team members to share their knowledge of the case and to resolve knowledge gaps and discrepant assumptions regarding how the case would proceed. The briefing was structured by a half-page checklist of prompts for patient information and procedural issues. The prompt for medication requirements included a sub-prompt for peri-operative antibiotic requirements (figure 1). The team briefing was designed to be more comprehensive than the traditional surgical ‘time out’; the ‘time out’ confirms only the patient's identity, procedure and side or site of surgery, and has become a common safety initiative internationally.13 27 Our briefing also included patient-related issues such as the patient's relevant operative history, psychosocial issues, preoperative tests and procedure-related issues such as special equipment needs, the availability of blood products and team experience. The checklist used in the team briefing was intended as a visual tool and participation in the briefing did not require any documentation or paperwork. Observers recorded the time of each briefing as falling into one of three categories: before patient arrival, after patient arrival and before induction, or after induction.

{kind=link}
A sample checklist used for preoperative team briefing.
As described previously,28 29 the briefing was intended not only as a site for immediate information exchange but also as a vehicle for encouraging a collaborative teamwork environment. Briefing leaders who engaged with the latter objective used the briefing to ‘map out’ the morning, indicating places in the case where decisions might need to be made, or moments when they would prefer to receive status updates from team members. Not all briefings functioned to highlight such teamwork issues; engagement with the teamwork in addition to the informational function of the briefing varied greatly and seemed to be related to a range of factors including leadership style, case complexity, briefing timing and team member enthusiasm.
Data collection
Antibiotic timing data
To constitute a post-intervention chart sample, one of three trained researchers retrospectively reviewed medical charts of all patients for whom a preoperative team briefing had been conducted. Data related to antibiotic administration were extracted from physician order forms, preoperative and day of surgery documents, and the anaesthesia record. The time of surgical incision was retrieved from the operative record. To select a pre-intervention sample, the surgery department provided a list of all procedures (along with associated operative details) that had been performed during the pre-intervention study period. From this set of cases, the research team used both purposive and convenience sampling to select a sample of pre-intervention cases. We sampled purposively to choose cases that provided a similar surgical sample to the post-intervention sample, matching according to type of procedure, surgeon and study site (table 1). An element of convenience sampling was reflected in the influence of chart availability on the sample: some records we sought were off-site and inaccessible during the study period, making it necessary to seek alternate charts that would support our matching criteria.
Characteristics of the operative procedures selected for pre-intervention and post-intervention chart review relevant to the assessment of the timeliness of antibiotics
Coding of antibiotic data
Timeliness of antibiotic administration was determined by calculating the difference between the documented time of antibiotic administration based on the chart documents and the time of incision recorded on the operative record. Antibiotic administration was coded as on-time, discordant, not-documented, contra-indicated or ambiguous-timing. A code of on-time was assigned to antibiotics that were documented as being administered within 1 h prior to the documented time of incision (a time period used extensively in the current literature to distinguish timely and untimely antibiotic administration7 9 11 17 30 31). A code of discordant was assigned to antibiotics that were documented as being administered outside of this 1 h window. Not-documented was assigned in situations where preoperative antibiotics were ordered but not documented as given, or where antibiotics were neither ordered nor documented as given but were a requirement of the procedure. A code of contra-indicated was assigned in situations where a contraindicated antibiotic was administered (ie, patient allergy). Ambiguous-timing was assigned when antibiotics were documented as given, but without clear evidence of the associated timing. All cases for which antibiotics were not a preoperative requirement, sufficient documentation was not present in the chart documents or the patient chart was not available for review were excluded from further analysis (table 2).
Codes applied to patterns of antibiotic administration documented in patient charts*
For procedures with more than one antibiotic, each antibiotic was evaluated independently and given an antibiotic code, and then one of these codes was assigned to represent the entire case. To establish this assignment of a single code for the case, a hierarchy of codes was developed and systematically applied to each case with discrepant antibiotic codes. Thus, for a case to obtain a code of on-time, every prescribed or administered antibiotic in a procedure had to be given on time for the entire case. This is similar to the method used by Tourmousoglou et al, where any divergence from guidelines for one drug led to a final assessment of discordant.32 For cases with at least one discordant antibiotic, this code took precedence over all other codes and a code of discordant was selected for the case. For cases where a discordant antibiotic was not recorded, the code of ambiguous-timing took next priority over all remaining codes, and finally the code of not-documented took precedence over the on-time code. Further details of the rationale for designing and implementing this complex coding methodology have been described previously.33
Analysis
Data from all three study sites were aggregated for analysis.
To determine whether there was a significant difference in the probability of timely antibiotic administration between the pre-intervention and post-intervention phases of the study, the frequency with which procedures were identified as having timely versus problematic antibiotic administrations was compared using χ2 analyses. Separate analyses were performed for three different levels of problematic timeliness, which were defined by combining different subcategories of codes to create the ‘untimely’ variable. Table 3 shows the groupings of codes into three levels of timing for analysis. Each level of timeliness reflected a graded measure of certainty about the accuracy and reliability of the data in the chart documentation. A p value of <0.05 was considered significant.
Difference in prophylactic antibiotic administration timing between pre-intervention and post-intervention study phases
Results
Study sample characteristics
As a pool of potential cases with which to assess the effect of team briefings on the timeliness of antibiotic prophylaxis, 454 team briefings were conducted in the post-intervention study phase. Of these cases, 73 did not require prophylactic antibiotics and these procedures were excluded from the current analysis of antibiotic timing. An additional 41 post-intervention cases were excluded because of documents missing from the patient chart or an inability to locate and review the patient chart. Thus, of the procedures for which team briefings were conducted in the post-intervention phase, 340 were included in the analysis. For 340 matched pre-intervention cases, chart data were also reviewed for timeliness of antibiotic administration and included in the analysis for comparison.
The majority of cases included in the analysis were open or laparoscopic colon surgeries. For procedures where antibiotics were administered, between one and three antibiotics were given. The most commonly administered antibiotic regimens were cefazolin alone or gentamicin and metronidazole in combination. Additional sample characteristics are illustrated in table 1.
Difference in antibiotic administration timing between pre-intervention and post-intervention study phases
On-time antibiotic prophylaxis administration increased between pre-intervention and post-intervention study phases for all three levels of untimeliness (table 3). When clearly-not-on-time cases were used as the untimely variable, on-time antibiotic prophylaxis administration increased from 77.6% in the pre-intervention study phase to 87.6% in the post-intervention study phase (p<0.01). On-time antibiotic administration increased from 64.0% to 76.5% between the pre-intervention and post-intervention study phases when clearly-problematic cases were included in the untimely data set (p<0.001), and from 59.1% to 72.9% when potentially-problematic cases were included in the untimely data set (p<0.001).
Difference in antibiotic administration by timing of team briefing
Of the 340 post-intervention briefings included in the antibiotic timing analysis, three did not include a record of the timing of the briefing. Of the remaining 337 briefings, 36 (10.7%) occurred before patient arrival, 52 (15.4%) occurred after patient arrival and before induction, and 249 (73.9%) occurred after induction. It is worth noting that there were statistically significant differences in the timing of briefings across sites (table 4); however, for the analysis assessing the role of briefing timing on the timeliness of antibiotic administration, data from the three sites were aggregated. For every level of antibiotic untimeliness (clearly-not-on-time, clearly-problematic and potentially-problematic), there was no statistically significant effect of the timing of the team briefing on antibiotic timeliness. In fact, contrary to the initial hypothesis, there was a slight tendency for a lower rather than higher percentage of on-time antibiotic administration in cases where briefings were conducted before patient arrival to the operating room relative to cases where briefings were conducted after patient arrival to the operating room (80.0% vs 88.9% for the clearly-not-on-time analysis). Again, however, these differences were not statistically significant (p>0.05).
Difference in briefing timing across the three sites
Discussion
A preoperative team briefing was assessed as a tool to improve the clinical practice of timely antibiotic administration. The results suggest a strong relationship between the team's adoption of a new communication routine—preoperative briefing—and an improvement in the timing of antibiotic prophylaxis. Consistent with recent studies of the surgical ‘time out’,9 11 we found that getting teams to talk preoperatively about salient case details positively influenced their antibiotic administration practices. Baseline rates of on-time prophylactic antibiotic administration range from 22.3% to 100% in the literature.7 11 21 26 30 31 34–42 Regardless of the level of problematic timing used in this analysis, the baseline rate of on-time administration was within this reported baseline range (77.6% vs clearly-not-on-time ; 64.0% vs clearly-problematic; 59.1% vs potentially-problematic). These baseline rates indicated considerable room for improvement in antibiotic administration practices prior to team briefing implementation. Other interventional studies report final rates of timely administration ranging between 60.6% and 99%.7 11 30 31 34 35 40 43–45 The final post-intervention rates of timely antibiotic prophylaxis (87.6% vs clearly-not-on-time ; 76.5% vs clearly-problematic; 72.9% vs potentially-problematic) in this study was comparable to these figures. We did not reach the final rates of timely administration attained by some interventional studies, with final rates of between 94% and 99% compliance to antibiotic prophylaxis timing guidelines.7 11 35 38 44 This might be explained by the fact that the research protocol used in this study did not include a ‘policing’ or monitoring function intended to directly improve antibiotic timing as those other interventional studies did through computerised recording, implementing new antibiotic documentation practices or team pressure. There was no incentive for operating room staff to participate or improve their performance; in fact, many staff were unaware that the research was tracking antibiotic timing as an outcome measure.
Inter-site variation
One of the study sites contributed a disproportionately large number of clearly-problematic cases to the sample, with approximately twice as many clearly-problematic cases as the other two sites across both study phases. In these instances, the clearly-problematic code was assigned because there was no documented record of antibiotic administration. It is possible that documentation practices were particularly poor at this one site and these clearly-problematic cases were truly a result of recording failure rather than antibiotic administration failure. We note that this could have artificially depressed the ‘on-time’ percentage in our potentially-problematic analysis, but would have remained consistent between the two study phases.
It is also noteworthy that there was inter-site variability in document formats, specifically for the anaesthesia record. This might have had an effect on the documentation practices encountered between sites and the likelihood of encountering cases where the documentation practices were unclear.
There was significant inter-site variability in the timing of briefings, with Site 2 completing a significantly larger proportion of briefings before patient arrival (27.2%) than the other two sites.
This difference may be a reflection of the fact that Site 2 had the smallest number of surgeons involved in the study and, as a consequence, study personnel were able to target direct and regular feedback to these surgeons regarding their briefing timing, managing to successfully encourage earlier team briefings at this site. At the other sites, where more surgeons were involved, feedback was spread more thinly due to study resources, with less success in encouraging early briefings. This experience suggests that implementation of team briefing protocols may necessitate resources for providing both timing feedback and regular reminders, if the goal is to conduct team briefings early enough in the preoperative period to transfer critical information before decisions have been made about issues such as patient positioning and anaesthetic requirements. With the growing popularity of checklist protocols, the issue of how such briefings happen, and what is required to support their effective conduct, is increasingly critical.
Limitations of the study
This study took place over a period of many months in organisational settings characterised by ongoing innovation and change. Several sources of parallel innovation might have confounded the results of this study. One study site introduced a new anaesthesia record midway through the study. The form included specific cues for documenting the antibiotics administered in the operating room as well as the time of administration. We would expect that the introduction of this form might improve the documenting practices of the anaesthesiologists and reduce the number of clearly-problematic and potentially-problematic cases observed over time, which was the observed trend at this site. However, since the majority of clearly-problematic and potentially-problematic cases in the overall sample did not come from this particular site, we do not believe that this innovation was primarily responsible for the observed effect in this study.
At one site, a separate hospital-sanctioned surgical ‘time out’ was introduced in parallel to our research-based preoperative team briefing, which might confound the effect of our intervention on the improvement observed in antibiotic administration timing. However, although this ‘time out’ was introduced in theory, the research observers for this study never observed a separate ‘time out’ performed in addition to the research-based team briefing in study cases. Thus confounding is probably a non-issue. At a second site, a separate hospital-sanctioned surgical ‘time out’ was present throughout both the pre-intervention and the post-intervention phases of this study. Thus, while it might have influenced team practices, we would expect this influence to be equally distributed across both data collection phases.
It is also possible that over the course of the implementation of our intervention, awareness about the importance of timely antibiotic prophylaxis improved among operating room staff (whether due to our presence in the operating room or due to external influences such as educational exposure). It was not uncommon over the course of this study to observe educational communication between staff about the importance of timely antibiotic administration before surgical incision. Consequently, the observed improvement in antibiotic prophylaxis timing may have been influenced by ongoing educational endeavours.
Recommendations
It is apparent from our observations that the process by which patients receive preoperative antibiotics is, at times, unclear to professionals in the field. This process needs to be standardised so that the operating room team has consistent expectations of who will be administering the antibiotics, when they will be administered and where they will be administered. It is also evident that an identifiable and unambiguous site for the recording of antibiotic administration is required for clear and consistent documentation practices.
Future direction
The team briefing was able to improve the timing of antibiotic prophylaxis administration, but to a level that still allows for further improvement. Data collection methods that do not require retrospective interpretation of patient chart documents would help to further differentiate the effects of the intervention from documentation error.
Sustainability was explored by Rosenberg et al,11 who found that after ‘piggybacking’ an antibiotic prophylaxis safety initiative onto a pre-existing surgical time out compliance dropped by a small amount from 99.1% compliance during the initiative to 96.8% compliance during and 18 months after the initiative. The methodology in this study was not designed to show whether the improvement in antibiotic administration timing in response to the team briefing is sustainable beyond the study period.
Other clinical outcome measures should be studied to determine whether the impact of the briefing is specific to improvement in antibiotic administration timing, or whether the briefing is a tool that has implications for clinical practice in general. For instance, recent work by Haynes et al marks an important step forward in linking briefing practices and morbidity and mortality outcomes.15
In summary, this study showed that routine preoperative team briefing is a communication routine that significantly increases timely antibiotic administration, which has been established as an important measure for patient safety.
Acknowledgments
The authors would like to thank Fauzia Gardezi, Janice Padilla and Sarah Whyte for their assistance with implementation of the study intervention and data acquisition.
References
Footnotes
Access to data: LL had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Role of the sponsor: The funders had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; and preparation, review or approval of the manuscript.
Funding This research was funded by the Canadian Institutes of Health 10 Research (CIHR), reference number 57796. LL is supported by the CIHR New Investigator Research Award and as the BMO Financial Group Professor in Health Professions Education Research at the University Health Network. GR is supported as the Richard and Elizabeth Currie Chair in Health Professions Education Research at the University Health Network. BO's research is supported by a Canada Research Chair. Canadian Institutes of Health Research (CIHR), reference number 57796160 Elgin Street, 9th Floor Address Locator 4809A Ottawa, ON, K1A 0W9, Canada.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.