Article Text

Abstract
Background A growing body of peer-reviewed studies demonstrate the importance of safety culture in healthcare safety improvement, but little attention has focused on developing a common set of definitions, dimensions and measures.
Objectives Specific objectives of this literature review include: summarising definitions of safety culture and safety climate, identifying theories, dimensions and measures of safety culture in healthcare, and reviewing progress in improving safety culture.
Methods Peer-reviewed, English-language articles published from 1980 to 2009 pertaining to safety culture in healthcare were reviewed. One hundred and thirty-nine studies were included in this review.
Results Results suggest that there is disagreement among researchers as to how safety culture should be defined, as well as whether or not safety culture is intrinsically diverse from the concept of safety climate. This variance extends into the dimensions and measurement of safety culture, and interventions to influence culture change.
Discussion Most studies utilise quantitative surveys to measure safety culture, and propose improvements in safety by implementing multifaceted interventions targeting several dimensions. Conversely, very few studies made their theoretical underpinnings explicit. Moving forward, a common set of definitions and dimensions will enable researchers to better share information and strategies to improve safety culture in healthcare, building momentum in this rapidly expanding field. Advancing the measurement of safety culture to include both quantitative and qualitative methods should be further explored. Using the expertise of traditional culture experts, anthropologists, more in-depth observational and longitudinal research is needed to move research in this area forward.
- Safety culture
- safety climate
- patient safety
- healthcare
- literature review
- safety culture
Statistics from Altmetric.com
Introduction
The term ‘safety culture’ first appeared after the Chernobyl nuclear power disaster in 1988. Since then, the concept has been embraced by several industries to improve safety, especially in high-reliability organisations (HROs) otherwise known as extremely safe, high-risk organisations (ie, aviation and nuclear power). More recently, the focus on building a culture of safety has moved to the healthcare domain. Since the Institute of Medicine's landmark To Err is Human report, a growing body of peer-reviewed studies have demonstrated the importance of safety culture in healthcare safety improvement; however, little attention has focused on developing a common set of definitions, dimensions and measures of safety culture in healthcare.1 The purpose of this literature review was to identify and summarise previous studies which define, explore and assess safety culture as the concept applies to healthcare. Specific objectives include: summarising definitions of safety culture and safety climate, identifying theoretical underpinnings, dimensions and measures of safety culture in healthcare, and reviewing progress in improving culture via interventions. Considering the publication word limit and comprehensiveness of presented material, sources of included studies are summarised alphabetically in online appendix 1. Online appendix 1 is designed to be useful for both researchers and healthcare practitioners, providing a resource of available primary research articles on basic safety culture concepts and interventions to improve culture.
Methods
Literature search
Studies were identified by searching Scopus, Web of Science, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PubMed, and PsycINFO electronic databases. Search terms included (safety culture* or safety climate* or culture of safety*) and (healthcare* or hosp* or long term care* or nursing home* or community*) and (patient safety* or public safety*). The searches were limited to English-language studies published between 1980 and 2009.
Inclusion and exclusion criteria
To be eligible for inclusion in the review, the studies had to be peer-reviewed, published before 1980 and written in English. They also had to focus on healthcare and describe one or more of the following: definition of safety culture or climate as a concept, provide dimensions of safety culture, measures, and/or intervention(s) and progress in the study of safety culture in healthcare.
Selection process
The final searches yielded 1341 articles. After 17 duplicates were excluded, a total of 1324 titles were reviewed. Of these, a total of 1124 unique abstracts were rejected, as they did not meet inclusion criteria. This resulted in 200 retrieved full-text papers. Using the inclusion criteria, articles that did not provide sufficient information on safety culture as a concept in healthcare were excluded, resulting in a total of 139 studies. Two reports and two books were also included, as secondary sources from the studies reviewed. Figure 1 shows a flow chart of the search strategy and selection process.
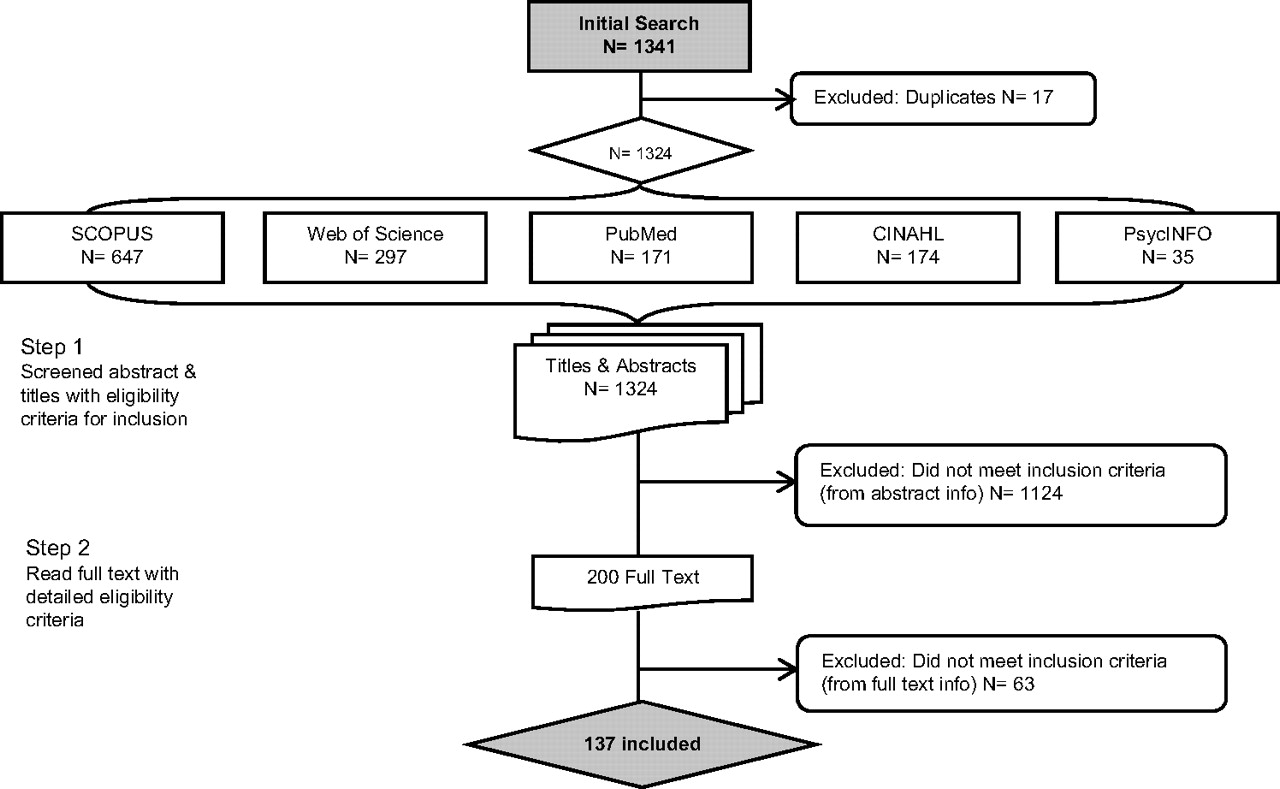
Flow chart of search strategy and selection process.
Results
Of the 139 studies reviewed, most arose from the USA (N=89), followed by Canada (N=15), the UK (N=8) and several other European countries (N=10). One randomised control trial was identified (online appendix 1).2
Theoretical underpinnings
In this review, 58 articles used theory to guide their studies or proposed theories to move research in safety culture forward, and the remainder of studies did not indicate their epistemological or theoretical roots. Within these studies, 32 different theories emerged (online appendix 1 contains a list of theories by article), and some studies employed more than one theory. The five most frequently adopted theories are summarised in table 1.
Five most frequently cited theories in the review
Defining safety culture
Common terminology included safety culture, culture of safety or safety climate. Results indicate considerable variation in the use of terms and definitions. For example, there is an ongoing debate about whether safety culture is inherently different from the concept of safety climate. To complicate the situation, the two terms are often defined the same and are used interchangeably within publications. One researcher suggests that, ‘safety culture has the definitional precision of a cloud.’3 Most researchers prefer the term safety culture (n=42), others adopted the term safety climate (n=8), and still some studies took a more holistic approach defining both terms (n=11) (online appendix 1). An overwhelming majority of studies used, but did not define, either term (n=82). The most commonly (n=17) used definition of safety culture was as follows:
The product of individual and group values, attitudes, competencies and patterns of behaviour that determine the commitment to, and the style and proficiency of, an organisation's health and safety programmes. Organisations with a positive safety culture are characterised by communications founded on mutual trust, by shared perceptions of the importance of safety, and by confidence in the efficacy of preventive measure.8
Meanwhile, safety climate was commonly defined as, ‘surface features of the safety culture from attitudes and perceptions of individuals at a given point in time’ or ‘the measurable components of safety culture.’9 10
Dimensions of safety culture
Much like the disagreement in the definition of safety culture as a concept, this variance extends into the dimensions comprising a positive safety culture. Since researchers have yet to reach consensus on the dimensions that comprise safety culture, several different combinations of dimensions exist. Dimensions often arose from factor analysis of quantitative safety culture questionnaires, and these combinations of dimensions subsequently became a way to conceptualise safety culture. One hundred and thirteen of the reviewed articles provided dimensions (online appendix 1), and the most frequently cited dimensions included:
leadership commitment to safety;
open communication founded on trust;
organisational learning;
a non-punitive approach to adverse event reporting and analysis;
teamwork; and
shared belief in the importance of safety.
Measuring safety culture
Safety culture in healthcare settings is typically assessed through quantitative questionnaires based upon any number and combination of the dimensions. A previously published study assessed the psychometric properties of available tools.11 These tools vary in the number of dimensions they measure (three to 12), length (from 30 to 79 items) and reliability (α ranging from 0.63 to 0.86).11 This review identified 12 different survey tools, as listed in online appendix 1. The following four tools were the most frequently cited:
Agency for Healthcare Research and Quality (AHRQ)'s Hospital Survey on Patient Safety Culture12;
Safety Attitudes Questionnaire13;
Patient Safety Culture in Healthcare Organizations Survey (PSCHO)14;
Modified Stanford Patient Safety Culture Survey Instrument (MSI).15
While regulatory and accreditation bodies have been quick to adopt and promote the use of these tools, one researcher cautions that strong evidence of psychometric rigour has not yet been published for the measurement of healthcare safety culture.16 Conversely, among the articles reviewed, 14 utilised qualitative methods to collect data on safety culture (online appendix 1). Of these, seven used semistructured interviews; two employed focus groups, and two used observations.
A few studies adapted Westrum's industry-focused typology of organisational cultures into varying models of cultural maturity for healthcare settings.4 According to Westrum, five phases of safety culture maturity were characterised to be:
Pathological: who cares about safety as long as we are not caught?
Reactive: safety is important—we do a lot every time we have an accident.
Calculative: we have systems in place to manage all hazards.
Proactive: we try to anticipate safety problems before they arise.
Generative: safety is how we do business around here.4
Three studies made use of Westrum's model by adapting it to fit the healthcare context by developing new tools, such as the Manchester Patient Safety Framework (MaPSaF) and the Patient Safety Culture Improvement Tool.17–19 These tools can be used in a collaborative manner to diagnose culture maturity and provide a framework for safety improvement.
While surveys can provide an understanding of staff attitudes and beliefs, it was recommended by several authors to supplement these quantitative data with richer qualitative data through interviews, focus groups and observations to gain a better sense of the underlying culture.6 20 21 Employing ethnographic methods of observation and interviews were also suggested to examine the validity of surveys.20 One study suggested that in-depth, long-term study using qualitative methods longitudinally is the only way to gain a deep understanding of culture.21
Improving safety culture via interventions
Despite the overwhelming rise in healthcare safety culture assessment, description alone cannot improve the safety culture of an organisation. Instead, improving safety culture was most frequently accomplished by implementing any number of interventions, often targeting one or more dimensions of safety culture at a time. Twenty-one studies reported or proposed the improvement of safety culture by implementing multifaceted interventions (online appendix 1). One study suggested that the first step was to assess the current status, normally accomplished via surveys.22 The following stepwise solution to improving reliability was proposed by one group of researchers: (1) assess culture of safety; (2) provide safety science education; (3) identify safety concerns; (4) establish senior leadership partnerships with units; (5) learn from one safety defect per month; and (6) reassess culture.23
Several interventions to improve safety exist, and some are more prevalent than others. Team training, patient safety team creation, leadership ‘walkarounds’ and patient safety education programmes were the most frequently cited interventions; however, other less frequently implemented interventions, such as safety audits, event reporting and analysis systems, and the dissemination of patient safety-related information to staff and patients, were also reported. All articles implementing or proposing interventions are itemised in online appendix 1. None of the articles reviewed assessed the effectiveness of interventions.
Discussion
Despite the increase in peer-reviewed studies on safety culture in healthcare in the past decade, many studies poorly defined the concept, and there was much disagreement on how safety culture should be conceptualised. The most common concepts have been reported here. The number of studies which overlooked the importance of properly defining concepts and guiding research with theory is surprising. The results of this review suggest that a dimension of safety culture is one factor that contributes to the development of a positive safety culture. Researchers and organisations frequently adopted a model of safety culture that featured multiple dimensions, introduced through the use of safety culture questionnaires, or by creation of new tools. However, understanding culture warrants more in-depth study, and better grounding in available theories. Developing and using theory to guide the collection, analysis and evaluation of evidence is a neglected facet of generating the knowledge needed to study safety culture. Perhaps we can assume that most researchers in safety culture come from a postpositivist paradigm, neglecting the importance to be explicit about their underlying epistemologies and theoretical roots.
It is possible that some researchers believe the study of safety culture in healthcare is now commonplace, and basic concepts no longer need to be defined; however, it is unlikely that most healthcare practitioners find safety culture commonsensical. While this review provided an overview of common concepts, the missing piece in the study of safety culture in healthcare is culture itself. None of the reviewed studies were conducted by anthropologists or used ethnography as a methodology. Since anthropologists are considered experts in understanding culture, shouldn't more healthcare agencies and researchers consult these experts when conducting research on safety culture?
Some studies did propose the need for more observational, longitudinal research; however, in practice most organisations were adopting surveys to measure culture. The multitude of available survey tools points to a lack of synergy in the healthcare safety culture improvement movement, since no tool has emerged as the gold standard for use, despite the adoption of certain tools by regulatory and accreditation bodies (eg, in Canada, Accreditation Canada requires participating organisations to use the MSI). While surveys are a pragmatic means of collecting data, these tools at best provide a superficial snapshot of climate, not culture. Compared with HROs, who have evolved and now focus on using qualitative methodologies to explore underlying culture, healthcare safety culture research seems to be in its infancy.
Still, reviewed studies reported a variety of interventions to improve safety culture in healthcare. Generally, improvements were accomplished by implementing multifaceted interventions, targeting more than one dimension of safety culture at a time. A systematic review on the effectiveness of these interventions is acutely needed. In the future, research on improving safety culture should be conducted longitudinally to ensure sufficient time to observe and measure change (eg, at least 3–5 years).24 25
Although the utmost effort was put in place to provide a comprehensive review of currently available evidence about safety culture in healthcare, this review has several limitations. The majority of studies included were from the acute care hospitals, some were from rehabilitation settings and long-term care, and none were from community or home care settings. In addition, this review did not assess the methodological quality of studies. Nevertheless, the review provides a starting-point to come to a common understanding and use of definitions and measures of safety culture.
Conclusion
A first step for healthcare organisations to improve safety culture is to clearly define and conceptualise the concept. Since culture is a context-specific, local phenomenon, it may be best to focus on the unit-level rather than the entire organisation.26–28 In this manner, improving each unit's safety culture will contribute to improving the whole organisation's safety culture. The next step would be an assessment of the current safety culture via one of several methods proposed. The resulting weaknesses should be addressed using targeted interventions. An ongoing process of measuring, improving and evaluating safety culture should then be undertaken. The emerging model of improvement includes a continuous process of identifying strengths and weaknesses, implementing interventions and evaluation (figure 2).

{kind=link}
{kind=link}
Emerging model of improving safety culture in healthcare based on key concepts from reviewed literature.
Moving forward, a common set of concepts will enable researchers to better share information and strategies to improve safety culture in healthcare, building momentum in this rapidly expanding field. Advancing the measurement of safety culture to include both quantitative and qualitative methods should be further explored, and longitudinal research in culture change is required.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
Web Only Data
Files in this Data Supplement:
Footnotes
Funding Canadian Institutes of Health Research; Ontario Neurotrauma Foundation.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.