Article Text

Abstract
Objective To test the psychometric soundness of the Safety Attitudes Questionnaire (SAQ) in Turkish hospitals, examine differences in perceptions of safety and provide baseline data.
Methods The SAQ (inpatient version) was translated with the back-translation technique into Turkish. Ten out of 50 teaching hospitals belonging to the Ministry of Health in Turkey were selected randomly. The Turkish version of the SAQ was administered to a sample of 2000 care givers at 10 hospitals. The factor structure of the responses was tested by confirmatory factor analysis. Cronbach alphas were calculated, and the mean and percentage positive safety attitude scores were assessed.
Results The response rate was 67.5%. Cronbach alphas of six factors (teamwork climate, safety climate, job satisfaction, stress recognition, perceptions of management, and working conditions) ranged from 0.66 to 0.77. Goodness-of-fit indices from the confirmatory factor analysis showed a reasonable model fit. There was a substantial variability among hospitals in terms of items and factors. Baseline data for the Turkish hospitals are presented.
Conclusion The Turkish translation of the SAQ showed satisfactory internal psychometric properties. Attitudes relevant to safety culture vary widely by hospital and indicate a need for improvement. Survey findings provide a baseline for future benchmarking.
- Patient safety
- safety
- culture
- safety attitudes questionnaire
- hospitals
- safety culture
- reliability
- assessment
- organisation
Statistics from Altmetric.com
- Patient safety
- safety
- culture
- safety attitudes questionnaire
- hospitals
- safety culture
- reliability
- assessment
- organisation
Patient safety is an important component of healthcare quality.1 Findings from several studies in various countries suggest that between 2.9% and 16.6% of patients admitted to hospitals experience one or more adverse events. Up to 50% of the adverse events are judged to be preventable.2–9
It is widely believed that healthcare organisations have to build a patient safety culture to reduce adverse events and improve patient safety.1 10–16 Safety culture is a part of organisational culture and may be defined as the attitudes, beliefs, perceptions, and values that employees share in relation to safety.17 It is usually measured by workforce questionnaire surveys.18 19 One of the most widely used questionnaire for measuring patient safety culture is the Safety Attitudes Questionnaire (SAQ), developed by the University of Texas.
The SAQ has been adapted for use in intensive care units, operating rooms, general inpatient settings (medical ward, surgical ward, etc), ambulatory clinics, pharmacies, emergency departments, and labour and delivery units.20 It is also available in the forms of safety climate survey and teamwork and safety climate.21 The psychometric properties of the several versions of the SAQ have been assessed in several countries. The 30-item SAQ demonstrated good psychometric properties on data from the USA, the UK and New Zealand.22 A 22-item version of the safety climate questionnaire was found to be a usable research instrument in the UK.23 The generic version of the SAQ showed satisfactory internal psychometric properties in Norway.24 The SAQ has been administered in many countries, and international benchmarking data are also available.22 However, to what extent these findings would generalise to Turkish hospitals is not known.
In Turkey, some hospitals (mostly private) attempt to improve patient safety to be accredited by an international accreditation organisation. A performance-based supplementary payment system (PBSPS) was introduced in the Ministry of Health (MoH) hospitals in 2004.25 The current PBSPS gives great importance to safety and encourages patient safety efforts.26 Furthermore, a recent notification requires both public and private health institutions to implement patient and employee safety practices.27 To raise patient safety awareness and build a safety culture, patient safety congresses have been convened, and in-service training has been given, too. Yet, there is little empirical evidence regarding safety culture in Turkey.
Thus, we conducted a survey with three principal objectives: (1) to test the psychometric soundness of the SAQ in Turkish hospitals, (2) to examine differences in perceptions of safety, and (3) to provide baseline data in order to identify opportunities for improvement and to assess future improvement efforts.
Methods
Survey instrument
We used the 59-item Safety Attitudes Questionnaire (Inpatient Version)20 where the care-giving areas are not specified in the items such as ‘Medical errors are handled appropriately in this ICU’ but kept neutral such as ‘Medical errors are handled appropriately in this clinical area’. We chose the SAQ based on its brevity, stable and robust factor structure, and wide administration. It is also the only questionnaire which shows links to patient outcomes.19 The SAQ elicits a snapshot of the safety culture through surveys of frontline worker perceptions.22
The SAQ measures six factors (dimensions): teamwork climate, safety climate, job satisfaction, perceptions of management, stress recognition and working conditions.22 Results from these factors are reported in this article. The items belonging to each factor are listed in table 1. The SAQ uses a five-point Likert-type scale with response choices of disagree strongly (1), disagree slightly (2), neutral (3), agree slightly (4) and agree strongly (5).
Safety Attitudes Questionnaire item descriptives
The original SAQ was translated into Turkish by the first author (SK). Then, this Turkish version was translated back into English by an independent translator who had never seen the original version before. The original SAQ and back-translation were compared by one of the developers of the American SAQ. Since he concluded that all items in them have the same meaning, the Turkish translation was accepted as valid. A pilot study was performed on 30 physicians and 30 nurses from three hospitals. Minor adaptations were made to the questionnaire wording before it was used in the survey. For example, ‘physicians’ was changed to ‘doctors’.
Sample
We decided to administer the SAQ in hospital wards, since we thought that safety culture in wards may be different from the culture in other work areas in the hospital, and strategies for improving safety culture should be tailored accordingly. In fact, a recent study28 found safety climate to be lowest among personnel working in emergency departments followed by wards and highest among personnel in other clinical and nonclinical areas.
At the time of the study, there were 50 teaching hospitals belonging to the MoH in Turkey. We selected 10 out of 50 hospitals randomly. Then, we asked the 10 sampled hospitals how many physicians and nurses had been working currently in their ‘general inpatient wards’ (medical wards, surgical wards, etc). We excluded emergency departments, operating rooms, intensive care units and other units such as radiology, pharmacy and physical therapy. We did not include part-time physicians (only 18% of physicians were practising part time, and they might have different perceptions and attitudes) but included midwives (most of whom work like a nurse).
We learnt that 2877 physicians and 1959 nurses met these criteria. We chose 1190 physicians and 810 nurses using a stratified random sampling technique with probability proportional to size allocation. Between 1 and 28 February 2007, quality department personnel of the hospitals distributed the questionnaire to the sampled care givers. The completed questionnaires were placed in sealed envelopes and sent to the first author at the university for analysis.
Analysis of the data
Each factor (scale) score was computed by taking the mean of its component survey items (two negatively worded items were reverse-scored so that their valence matched the positively worded items). We also present percentage agreement to facilitate understanding of the items and scales. The percentages of all respondents within a hospital reporting ‘agree slightly’ or ‘agree strongly’ for each of the items within a given scale were charted as the percentage positive.22
To test the psychometric soundness of this patient safety survey, we investigated the underlying factorial structure of the SAQ using CFA. We used a number of fit indices—comparative fit index (CFI), Tucker–Lewis index (TLI), root mean square error of approximation (RMSEA), standardised root mean square residuals (SRMR)—in addition to the model χ2 statistic, using the recommended cut-off values of greater than 0.90 for the CFI and TLI, less than 0.08 for the RMSEA, and less than 0.10 for the SRMR.29 The p value should exceed 0.05,30 although large samples may produce low p values even in good models.31
Internal reliability of the factors was measured using Cronbach α. If different items are supposed to measure the same concept, the internal reliability should be greater than or equal to 0.6.32
The construct validity was also studied by calculating Pearson correlation coefficients between the scale scores. The construct validity of each factor is reflected in scale scores that are moderately related.33 All statistical analyses were performed using SPSS version 11.0 (SPSS, Chicago, Illinois) and AMOS version 4.0 (SmallWaters, Chicago, Illinois).
Results
Response rates and demographics
There were 1349 respondents out of 2000 questionnaires administered in 10 hospitals (734 physicians, and 615 nurses), for an overall response rate of 67.5%. Nurses had a higher response rate (75.9%) than physicians (61.7%). The average respondent was 33 years old with 5 years of experience at the current department and 7 years of experience at the current hospital. Almost all nurses (98.2%) and one-third of physicians (32.8%) were female (table 2).
Response rates and characteristics of respondents by care giver type
Safety climate scale psychometrics
The Cronbach alphas of six factors ranged from 0.66 to 0.77 (table 3). The alpha value for the 30-item SAQ was 0.89.
Mean factor scores and intercorrelations of the six dimensions
The factor structure of the responses was tested by CFA. Our factor structure model is presented in figure 1. Goodness-of-fit-indices for the model are shown in table 4. Pearson correlation coefficients between the scale scores can be seen in table 3.

Factor structure model.
Goodness-of-fit indices for factor structure model
Baseline climate
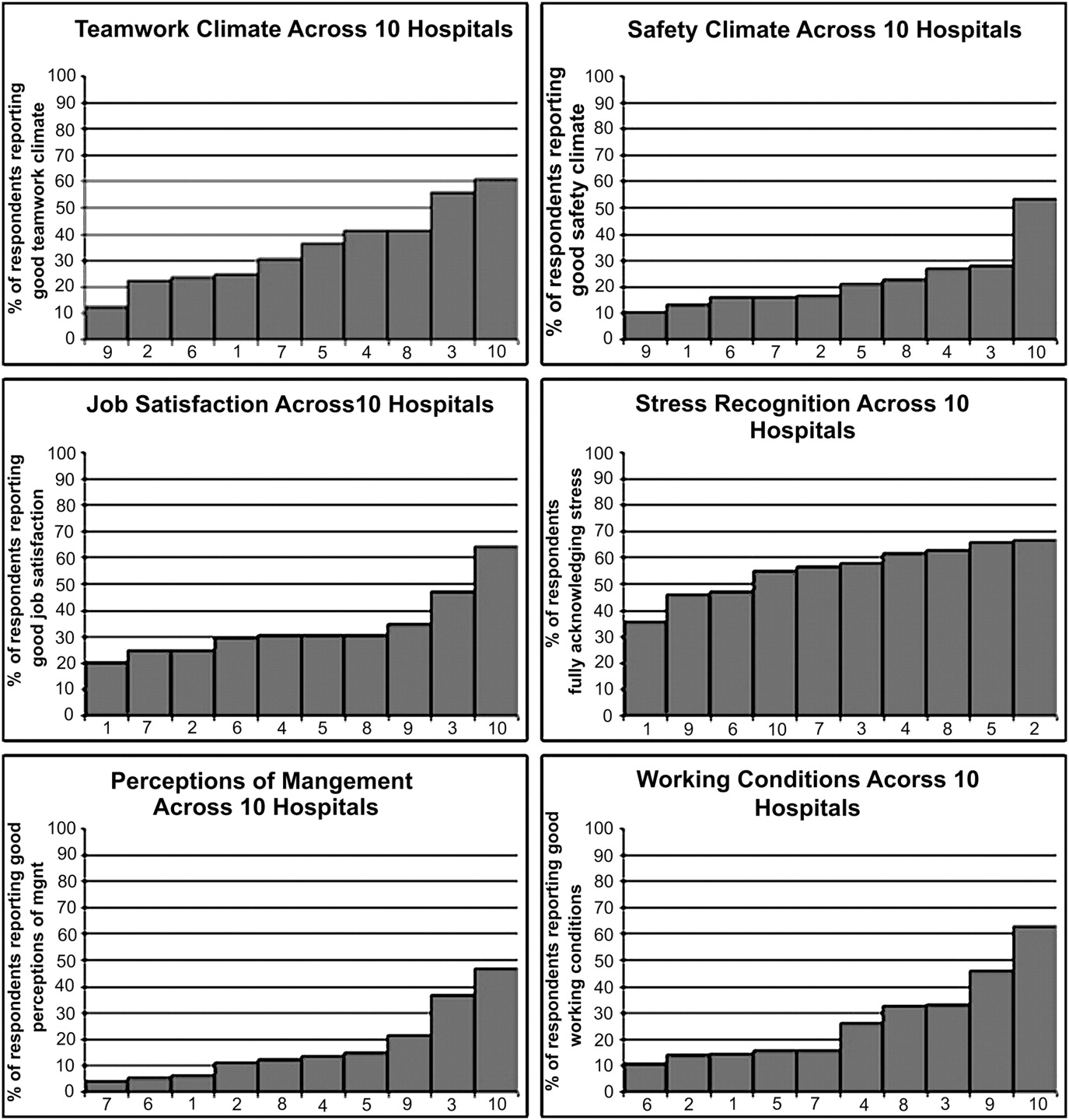
The means for SAQ factors are shown in table 3. SAQ item descriptives are presented in table 1. The six SAQ factor distributions in figure 2 demonstrate the variability in percentage positive SAQ scores across the 10 hospitals.
{kind=link}
{kind=link}
Percentage positive scores are computed as the percentage of respondents within a hospital who answered agree slightly or agree strongly on each of items within a scale (ie, 4 or 5 on the original five-point Likert scale).
Discussion
This study provides the most complete information available to date on patient safety culture in Turkish hospitals and revealed several important findings about psychometric properties of the Turkish version of the SAQ.
Our response rate (67.5%) was similar to the response rates of (67–68%) previous SAQ administrations in other countries.22 24 34 As shown in table 1, no items produced a large number of missing responses. These findings testify to the acceptability of the SAQ in the Turkish hospitals.
Composite scale reliability for the SAQ (0.89) was as strong as the SAQ reliability (0.90) found in the international benchmark data.22 Cronbach alphas for all factors were greater than 0.60.
The construct validity of the SAQ containing 30 items, as judged by the goodness-of-fit indices from the CFA, was generally satisfactory. The p value of less than 0.001 speaks against the fit of the model to the data, but the TLI (0.969) and CFI (0.974) exceeded the recommended cut-off values of 0.90, the RMSEA (0.069) was less than the critical value of 0.08, and the SRMR (0.061) was below the suggested criteria of 0.10.
Examination of table 3 shows that six factors have moderately related. The highest correlation was between Working Conditions and Safety Climate (r=0.69), but no correlation was exceptionally high. It is interesting that the highest correlation found in the international benchmark data (between 203 clinical areas) was also found between Working Conditions and Safety Climate (0.95).22
On the basis of the above evidence, we conclude that the Turkish translation of the SAQ is a reasonably reliable and valid instrument for the measurement of patient safety culture in Turkish hospitals.
We found substantial variability among hospitals in terms of items (table 1) and factors (figure 2). All hospitals were MoH hospitals, and the same regulations are applied to all. The variation among the hospitals may result from the hospital managers demonstrating different levels of commitment to patient safety.
The item descriptives (table 1), percentage positive distributions (figure 2) and mean factor scores (table 3) serve as baseline data for the SAQ in Turkey. When we compared our item results with SAQ international benchmark data from cross-sectional surveys of 10 843 healthcare providers in three countries (USA, UK, New Zealand),22 our scores were generally lower (ie, our respondents’ scores were more negative). The lowest scores were found on the items of ‘I am encouraged by my colleagues to report any patient safety concerns I may have’ (49% vs 78% agree), ‘the culture in this clinical area makes it easy to learn from the errors of others’ (45% vs 72% agree), and ‘I receive appropriate feedback about my performance’ (27% vs 46% agree), so they will be important challenges for Turkish hospital managers. On the other hand, the items ‘fatigue impairs my performance during emergency situations’ (70% vs 40% agree) and ‘hospital management does not knowingly compromise the safety of patients’ (69% vs 41% agree) received the highest scores, compared with the international benchmark data. One of the prominent characteristics of the culture of our hospitals was a high level of stress recognition.
Providing safe care is all care givers' responsibility, but it is the leader's job to provide an environment where safe care could be given. Leaders should create structures, processes and programmes that allow a culture of safety to flourish. In order to promote patient safety, managers of the Turkish hospitals may use existing strategies, such as patient safety leadership walkrounds,35–37 safety briefings,38 39 comprehensive unit-based safety programme40–42 and teamwork training.43–45
Our findings establish a baseline for future benchmarking and identify opportunities for improvement in participating hospitals. The results reported here represent findings from the MoH teaching hospitals, but they may not be representative of other types of Turkish hospitals. Further research on the unit level, on other types of personnel, and on the relationship between safety culture and outcome variables is needed.
Acknowledgments
The authors thank E Bal for helping to collect data and PY Balçık for entering the data into the computer.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.