Article Text

Abstract
Objective: To enhance overall accuracy of medication lists by providing performance feedback and training to the healthcare team and increasing patient participation in the medication reconciliation process.
Methods: This prospective study involved patients seen in four academic, ambulatory primary care internal medicine clinics. Before the interventions, baseline data were analysed, assessing completeness, correctness and accuracy of medication documentation in the electronic medical record. Interventions to provide performance feedback and training to the healthcare team, increase patient awareness and participation in the medication reconciliation process were implemented. Immediately after each intervention, a data collection was undertaken to assess the effectiveness of the intervention on the accuracy of individual medications and medication lists.
Results: Completeness of medication lists improved from 20.4% to 50.4% (p<0.001). The incomplete documentation of medication lists was mostly because of lack of frequency (15.4%) and route (8.9%) for individual medications within a medication list. Correctness of medication lists improved from 23.1% to 37.7% (p = 0.087). The incorrectness in a medication list was mostly because of incorrect medications dose. Patient participation in the medication reconciliation process increased from 13.9% to 33% (p<0.001). The medication list accuracy improved from 11.5% to 29% (p = 0.014).
Conclusion: In this setting, it was helpful to engage the active participation of all members of the healthcare team and most importantly the patient to improve the accuracy of medication lists.
Statistics from Altmetric.com
Increasing numbers of complex patients with significant exacerbation of their conditions are being managed in the outpatient setting.1 Hospitalisations are being reserved for severe acutely ill or higher risk ill patients. However, most of the medication adverse drug event studies have been done in the hospital setting.23456 Very few studies have been done in the outpatient setting.7891011 Most of the studies done in the outpatient setting were observational studies showing that electronic medical records (EMRs) were no better or worse than paper records in term of accuracy of medication lists.
To reduce adverse drug events, it is necessary to maintain an accurate medication list in the medical record. In July 2004, the joint commission announced 2005 National Patient Safety Goal 8 to “accurately and completely reconcile medications across the continuum of care”. The joint commission has analysed sentinel events that have resulted from medication errors and determined the majority were because of communication errors that could have been avoided through medication reconciliation. The majority of the medication errors occur at transitions of care between providers. A part of the medication reconciliation process requires collecting a complete list of current medications for each patient. A medication list was defined as “complete” if all four components (name, dose, route and frequency) were documented for each individual medication in the medication list. A medication list was defined as “correct” if there was no discrepancy in the name, dose and frequency between the current medication list documented in the EMR and the medications the patient was actually taking at home. Consequently, a medication list was defined as “accurate” when it is both complete and correct simultaneously. Previous studies1011 have demonstrated improvements in medication list accuracy by educating the healthcare team on what constitutes a complete medication list. Varkey et al11 have stated that engaging the healthcare members and patient is crucial in the medication reconciliation process. We hypothesise that medication list accuracy would improve by including the patient in the process.
To test our hypothesis, we have designed interventions to increase the healthcare team’s and the patient’s participation in the medication reconciliation process by increasing awareness about medication reconciliation and educating about the importance of accurate medication lists. In addition, we have extended our initial prospective study conducted at one of the primary care internal medicine (PCIM) clinic outpatient practices to four PCIM outpatient clinics.
Methods
This prospective study was conducted from February 2006 to May 2007 in the Division of Primary Care Internal Medicine at Mayo Clinic Rochester. The PCIM practice consisted of four outpatient clinics staffed by 32 consultant physicians, six fellows and 95 residents who together provide primary care for more than 34 000 patients. This study was approved by the Mayo Clinic Institutional Review Board.
Medication list
During the study period, Mayo Clinic Rochester has an EMR with a Mayo-developed clinical notes application called documents browser. All visits are recorded in the documents browser. The medication list is contained within each note and is entered into a free text field with no interface to decision support or prescription order entry.
Patient population
Any patient with a physician appointment in the PCIM clinic was eligible for the study, even if they were taking no medications. However, patients who previously had refused to give consent for the use of their records for research or who were unable to communicate by telephone were excluded from the study.
Patient sample selection
Data were collected from three periods: pre-intervention and two immediate post-interventions. Patient selection consisted of randomly selecting and reviewing the clinical notes of 10 to 20 patients daily from the pool of all patients seen each day in our clinic, by using a table of random numbers. Pre-intervention patient selection consisted of reviewing randomly selected electronic clinical notes of 108 patients evaluated in our PCIM clinic during February–April 2006. Immediately after the first intervention (licensed practical nurse (LPN) intervention), randomly selected clinical notes of 102 patients were reviewed in September 2006. To determine the impact of patient participation on the accuracy of medication lists a second intervention (patient awareness intervention) was designed and implemented. Randomly selected clinical notes of 115 patients were reviewed in May 2007 after the second intervention.
Completeness of the medication list from the EMR
An individual medication was defined as “complete” if the name, dose, frequency and route of administration were documented. A medication list was defined as “complete” if all four components were documented for each individual medication in the medication list. The completeness of the medication lists was assessed by abstracting the information from the EMR.
Correctness of the medication list from interviewing patients
A medication list was defined as “correct” if there was no discrepancy in the name, dose and frequency between the current medication list documented in the EMR and the medications the patient was actually taking at home. To assess the correctness of the medication list of each patient, each selected patient was contacted at home by telephone and asked to read from their medication containers the name, dose and frequency of each medication he or she was currently taking. This information was compared with that documented in the patient’s EMR.
Accuracy of the medication list
A medication list was defined as “accurate” when it was both complete and correct simultaneously. Therefore, all the medications in the list from the EMR had the four components (name, dose, route and frequency). In addition, no discrepancy was found among the medication listed in the current medication list documented in the EMR and the medications the patient was taking at home.
Intervention
This study had three different measurement periods. The first measurement, or pre-intervention measurement, determined how often documented medication lists were complete and the major types of incompleteness. This was followed by an intervention to provide performance feedback and training for the LPNs, which was implemented in August 2006. The impact of the intervention on the accuracy of medication lists was assessed in September 2006 (LPN intervention). Finally, to evaluate the impact of patient participation in the medication reconciliation process, a third measurement was undertaken in May 2007 (patient awareness intervention).
Pre-intervention phase
The major types of incompleteness for medication lists were identified after the pre-intervention data collection. Analysis was performed and the findings communicated to a multidisciplinary team consisting of physicians, nurses, administration and allied health. The medication reconciliation initially consisted of sending an appointment confirmation letter asking the patients to bring to their visit their medication containers or an update medication list, having an LPN review the medications with the patient and enter an updated medication list into the EMR as a preliminary note and having the physician reconcile the medication list with the patient during the visit. However, the appointment confirmation letter was only sent to patients who had their visits scheduled 7 days in advance. PCIM has an advance access model, so many appointments are scheduled on the same day or next day that the patient calls for an appointment.
LPN intervention
The LPN intervention was implemented in August 2006 and the second data collection was done in September 2006. The intervention consisted of training LPNs on what constituted a complete and correct medication list and providing an individualised feedback to each LPN on their pre-intervention performance in terms of number and types of inaccuracies identified on the medication lists that they had entered into the EMR during the pre-intervention data collection period. The overall impact of this first intervention in the accuracy of the medication list was measured in September 2006.
Patient awareness intervention
In early May 2007, PCIM receptionists started calling the patients a day before their visit to the office, reminding them to bring their medication containers or an updated list of their medications. In addition, the paragraph asking the patient to bring their medication containers or an updated list was highlighted in the appointment confirmation letter. In the last 2 weeks of May, a brochure explaining the importance of knowing their medications was made available to the patient in the waiting room of the PCIM clinic. In addition, the LPNs were instructed to educate the patients about the importance of bringing their medications to their visits and to give each patient a copy of the brochure. Finally, at the end of the visit, the physicians were instructed to reconcile the medication list and provide a paper copy of the medication list available in the EMR to each patient. A third data collection was done during last 2 weeks of May 2007 to determine the impact of patient participation on the process of medication reconciliation.
Statistical analysis
Univariate comparisons between study phases were made using two-sample t tests for continuous variables and χ2 tests for categorical measures. In this study, the statistical analysis took into account that most patients have multiple medications by using generalised estimating equations within a logistic regression model. The minimum sample size to obtain a significant improvement in medication list accuracy from the pre-intervention level of 20% to 45% with 80% power was found to be 65 patients in each phase, with an α level of 0.05 and a two-tailed alternative. The statistical software package SAS (SAS Institute, Cary, North Carolina) was used for data analysis. Analysis was performed on three sets of medications: (a) all medications, (b) prescription medications only and (c) prescribed scheduled medications only. Prescription medication is defined as any medication that needed a prescription by a physician/nurse practitioner/physician assistant for the purchasing of the medication within the USA (ie, all medications excluding the over-the-counter medications). Prescribed scheduled medications are defined as medications that had to be taken at regular intervals of time.
Results
Patient characteristics
The clinical characteristics of the patients participating in the completeness portion of the study are listed in table 1. No significant difference was noted among the pre- and post-intervention measurements.
Pre- and post-intervention clinical characteristics of patients and physicians for the completeness portion of the study
The mean number of medications taken by patients ranged from 7.3 to 7.7, of which approximately 39% were over-the-counter and 11.7% were taken on an “as-needed” basis for symptoms.
Completeness
A statistically significant increase in the number of complete individual medications and the number of complete medication lists between the pre-intervention phase and the LPN intervention or patient intervention of the study were observed (p<0.03) (table 2). Associated with the interventions, there were improvements in the documentation of medication dose, route and frequency as shown in fig 1.
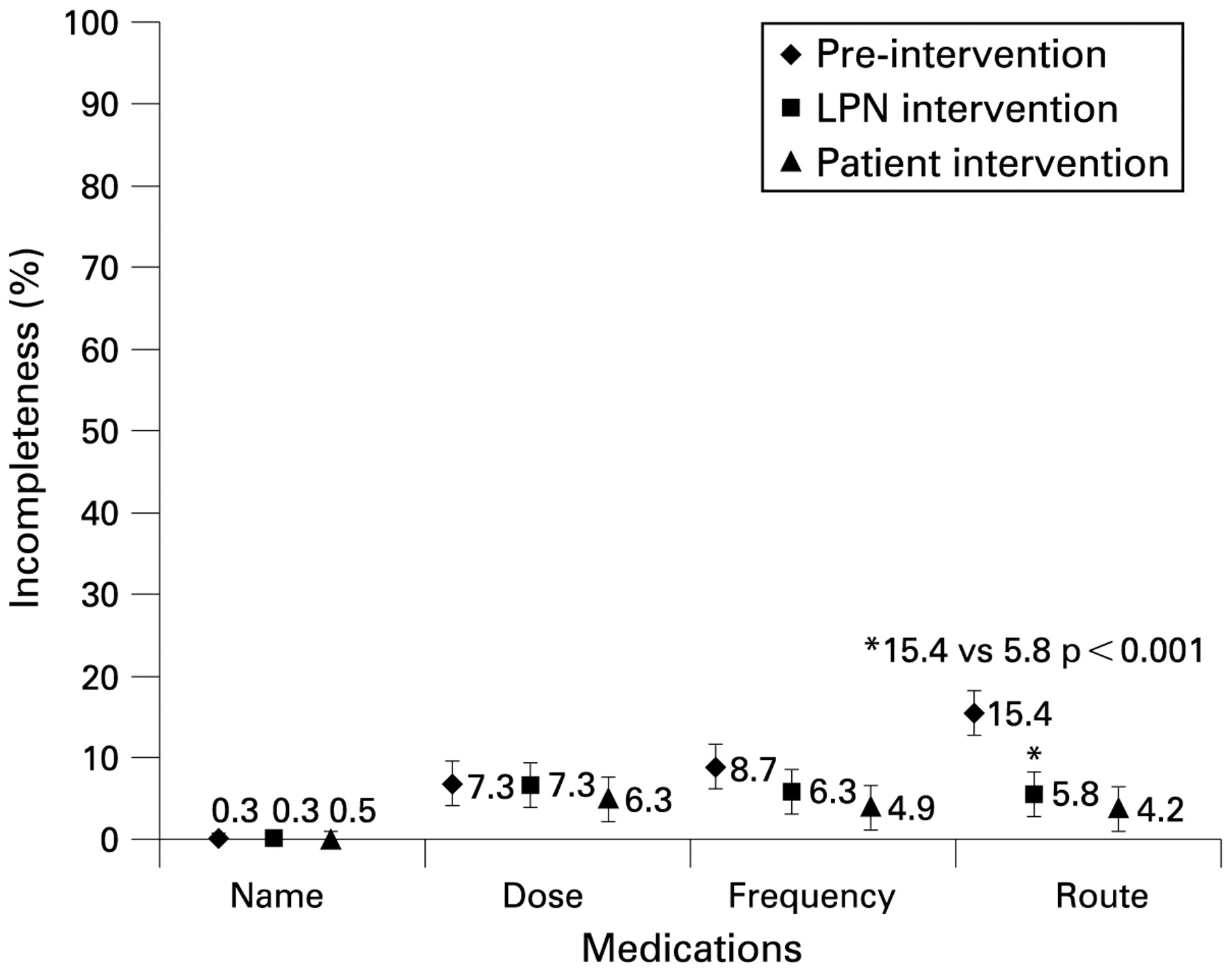
Reasons of incompleteness of individual medications at pre-intervention, LPN education and patient awareness interventions (per cent and 95% CIs).
Complete medication lists pre- and post-intervention measurements
Individual medications and medication lists for all medications were found incomplete more often than that for prescribed medications. The completeness of medication lists improved even further when analysis was restricted to prescribed scheduled medications (fig 2).

Improvement in completeness of medication lists of all medications, prescription medications and prescribed scheduled medications (per cent and 95% CIs).
Correctness
Not all patients included in the completeness portion of the study agreed to participate in the correctness portion of the study (fig 3). Fifty-six per cent of the eligible patients agreed to participate in the correctness pre-intervention phase (61 out of 108 patients contacted), while 51% of eligible patients agreed to participate in the LPN intervention phase (52 out of 102 patients contacted) and 60% of eligible patients agreed to participate in the patient intervention phase (69 out of 115 patients contacted).

Distribution of participants and non-participants in completeness and correctness portions. I, intervention; II, post-intervention.
When comparing correctness pre- and post-interventions measurements, differences between the clinical characteristics of patients whose medication lists were assessed for correctness were not significant. However, several clinical differences were noted between participants and non-participants in the correctness portion of the study. The participants were older than the non-participants (60.8 vs 57.3; p = 0.08), female (67.0% vs 57.3%; p = 0.07), but similar on being seen by staff doctor (74.7% vs 72.7%; p = 0.59) and number of medications (7.5 vs 7.4; p = 0.93).
The major reason(s) for incorrect medication lists was that the current EMR medication list had the incorrect dose and frequency. Another common source of error was that the EMR medication list was commonly found to contain medications no longer being taken by the patient. In addition, when contacted at home, patients reported taking medications that were not listed in the EMR medication list (medications added to the list). Comparison of data collected pre- and post-LPN interventions showed no statistically significant improvement in the correctness of medication lists (table 3). On the other hand, following the patient intervention, a statistically significant improvement in the individual medication dose, medications deleted from list and medications added to list were observed.
Correctness of medication lists and reasons of incorrectness for pre- and post-intervention for all medications
Accuracy
The accuracy of the medication lists improved significantly from the pre-intervention measurement to post LPN and patient interventions (ie, from 11.5% to 29% with p = 0.014). Medication lists containing only prescribed scheduled medications were the most accurate lists (fig 4). The improvement in the accuracy of the medication list was only observed when patients started to bring their medication containers or an updated medication lists to their medical visits (fig 4).

Accuracy of medication lists of all medications, prescription medications, and prescription and scheduled medications (per cent and 95% CIs).
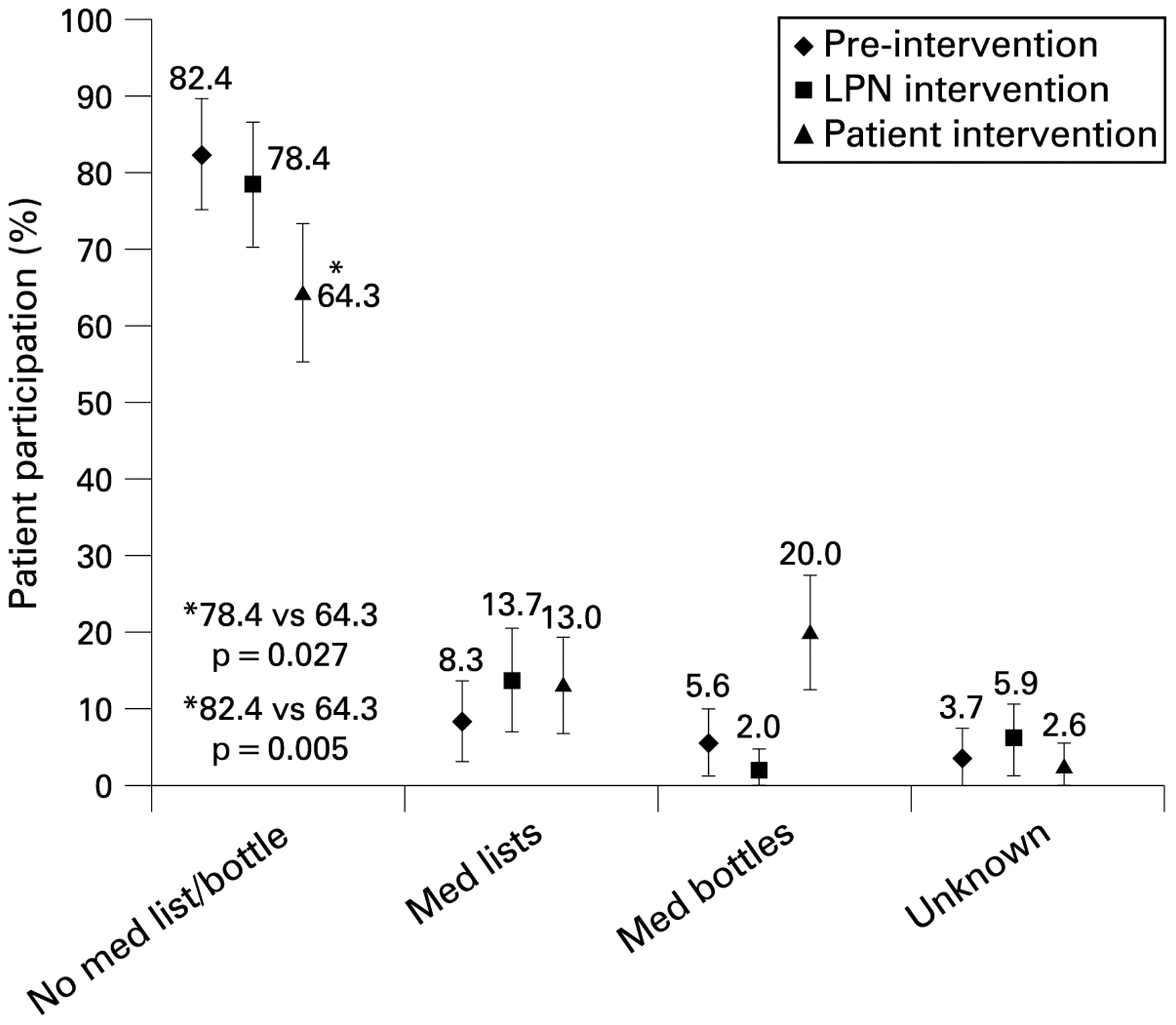
An increase from 13.9% to 33% (p<0.001) was observed in the percentage of patients who brought their medication containers and/or an updated list to their visit when they were called and reminded a day before their appointment (fig 5). In addition, the increase of patient awareness of the medication reconciliation process led to an increase in the percentage of medication list correctness from 23.1% to 37.7% (p = 0.087), as shown in table 3. This result supported our hypothesis that increasing patient active participation is an important component in improving the correctness of EMR medication lists.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of patients participating in the medication reconciliation process (per cent and 95% CIs).
Discussion
LPN training and performance feedback and increased patient participation were effective interventions that improved the completeness of medication lists and individual medications in an outpatient PCIM practice. The medication list completeness in the pre-intervention phase of this study was found to be in good agreement with the medication list completeness reported on our previous study10 (ie, 20.4% and 18.5%, respectively). This study showed the superiority of individualised feedback and training of LPNs intervention when comparing with general training of LPNs offered on our previous study,10 that is, a statistically significant increase in medication list completeness from 18.5% to 45.1% was observed (p<0.001).10 To further improve the completeness of the medication list, one must consistently provide training and individualised performance feedback to all the members of the healthcare team involved in the medication reconciliation process.
It was more difficult to improve the medication list correctness. The percentage of medication list correctness was found to be in good agreement between our previous study10 and this study (before patient awareness intervention) (ie, 18% and 23.1%, respectively). Furthermore, it was observed that when only training and personalised feedback was provided to the LPNs, the correctness of medication lists declined from 31.2% (pre-intervention) to 23.1% (after LPN intervention). Even though there was an absolute decline in our study in the correctness of the medication lists, it was not statistically significant (p<0.34). This finding is inconsistent with the audit and feedback finding by Varkey et al11, who found an improvement in the medication list correctness by participation of the healthcare members in the process. There are several possible reasons for the decline in the correctness of the medication list after the LPN intervention was implemented. First, a small number of patients agreed to participate in the correctness assessment that contributes to less precise point estimates for correctness. In addition, LPNs may have felt pressure to make all the medication lists complete and may have speculated on the dose based on previous medication lists when the actual medication containers were not available.
In contrast, the patient awareness intervention suggests that when the patients were invited to actively participate in the process by bringing their medication containers or an updated medication list, the correctness of the EMR medication lists improved from 23.1% to 37.7% (p = 0.087). Similarly, Varkey et al11 found that patient participation in the medication reconciliation process is crucial to enhance the accuracy of medication lists. Furthermore, our study found smaller discrepancies due to (a) failure to record medications that patients were actually taking, as compared to Bedell et al7 and Frank et al12 (our study 2.3% vs Bedell 20% and Frank 37%), and (b) inclusion of medications patients were not taking (our study 3.6% vs Bedell 29% and Frank 6%).
The majority of patients in our study did not bring a medication list or medication containers to the appointment with the physician, even when reminded. We hypothesise that to increase patient participation in the medication reconciliation process and the accuracy of medication lists, patients should be educated on the importance of knowing their medications and playing a more active role in helping their primary care providers in the management of their health problems. To achieve this goal, an education brochure was designed with the aim to help patients understand why medications have been prescribed and why they should be knowledgeable about the medications they are taking. This brochure was made available to the patients in the waiting rooms of the PCIM clinics and the LPNs were instructed to give a copy of the educational brochure to each patient during their visit to the clinic during our second intervention. We hypothesise that the impact of this intervention will be felt within a year of continuing education of our patient population. In addition, patients can be further engaged in the medication reconciliation process by including patient representatives as member of the practice improvement team to help identify changes that might affect patient’s behaviour.
Medication list accuracy improved from 11.5% to 29% (p = 0.014). To further improve the accuracy of the EMR medication lists, it is important to continue an ongoing discussion with patients about the importance of documenting all the medications they take and identifying optimal aids to help patients keep the list accurate. For example, providing patients with access to their EMR from home with the ability to edit the medication list is an area for development.
Study limitations and strengths
Our prospective study had several limitations. Because the intervention was implemented for our entire PCIM practice, we had no simultaneous control group to compare with the post-intervention group; however, the pre-intervention measurement can serve as a historical control. The results were based on four PCIM practices, which may not be generalised to other practice settings. Another potential limitation of the correctness portion was a participation rate ranging from 50% to 60% of the patients. Lastly, in this study, the gold standard for correctness evaluation was direct communication with patient and not pharmacy database.
On the other hand, this study has several strengths. It was conducted in an ambulatory setting in which patients were seen by residents and staff physicians. Few patients met the exclusion criteria of this study. Lastly, this study showed that it is possible to improve the accuracy of medication lists with a low technology solution, such as making a telephone call.
Future research could assess the impact of an electronic patient record, enhanced patient education efforts to educate patients regarding the importance of knowing their medications, clinician reminders to update the current medication list when making medication changes or additions, and quarterly performance feedback to LPNs and clinicians with comparison with peers.
Conclusion
The results of the present study showed that significant improvement in the accuracy of the entire medication list in an outpatient primary care practice can be achieved in a short time by involving and training all members of the healthcare team, providing performance feedback and increasing patient participation in the process. Further improvement in the accuracy of the medication list may be achieved by continuous education of healthcare team members, enhancing patient involvement through education, populating the medication list when prescriptions are ordered and providing patient access to their medical record.
Acknowledgments
The authors would like to acknowledge Holly K VanHouten for statistical analysis and Sara S Mason for helping with data collection and entry from February to April 2006.
REFERENCES
Footnotes
Presented as a poster at the ISQua 2007, Boston, Massachusetts, 30 September 2007.
Funding Funding for this study came from a Mayo Foundation CPI-10 grant.
Competing interests None.