Article Text

Abstract
Problem: Sliding scale insulin (SSI) is frequently used for inpatient management of hyperglycemia and is associated with a large number of medication errors and adverse events including hypoglycemia and hyperglycemia.
Design: Observational before and after study evaluating the impact of implementation of a standardized SSI protocol and preprinted physician order form.
Setting: University Hospital in Pittsburgh, PA, USA.
Strategy for change: Guidelines for the use of SSI were created by an interdisciplinary committee and implemented in non-intensive care units. In addition, a preprinted physician order sheet was developed which included the guidelines and an option for ordering one of three standardized insulin sliding scales or a patient specific scale.
Effect of change: One year after implementation the physician order form was used for 91% of orders and, overall, 86% of SSI orders followed the guidelines. The number of prescribing errors found on chart review was reduced from 10.3 per 100 SSI patient-days at baseline to 1.2 at 1 year (p = 0.03). The number of hyperglycemia episodes 1 year after implementation decreased from 55.9 to 16.3 per 100 SSI patient-days.
Lessons learnt: The protocol was readily accepted by hospital staff and was associated with decreased prescribing errors and decreased frequency of hyperglycemia.
- SSI, sliding scale insulin
- SSR, sliding scale regular insulin
- insulin
- medication errors
- hyperglycemia
- practice guidelines
- SSI, sliding scale insulin
- SSR, sliding scale regular insulin
- insulin
- medication errors
- hyperglycemia
- practice guidelines
Statistics from Altmetric.com
- SSI, sliding scale insulin
- SSR, sliding scale regular insulin
- insulin
- medication errors
- hyperglycemia
- practice guidelines
- SSI, sliding scale insulin
- SSR, sliding scale regular insulin
- insulin
- medication errors
- hyperglycemia
- practice guidelines
Sliding scale insulin (SSI) is commonly used to manage hospitalized patients with and without diabetes mellitus.1–3 Monotherapy with SSI often leads to erratic fluctuations of glucose control because it tries to retrospectively “treat” hyperglycemia rather than prospectively “prevent” it.1,4,5,6,7,8,9,10 In the hospital setting, use of supplemental short acting insulin in addition to scheduled basal and preprandial insulin for patients with type 1 diabetes is recommended.11,12 In addition, initial use of supplemental insulin as monotherapy for patients with type 2 diabetes with unknown insulin needs who are not eating is also suggested.11 Supplemental insulin can be thought of as the appropriate use of SSI.
OUTLINE OF PROBLEM
Before implementation of a standardized SSI protocol at our institution, SSI orders were physician-specific and varied in the minimum blood glucose level requiring an insulin dose as well as in the number of insulin units to be administered for a given blood glucose level. Individual physicians rarely used different scales for different patients and many did not start insulin until a patient’s blood glucose level exceeded 11.1 mmol/l (200 mg/dl). The variability in SSI orders contributed to a high frequency of medication errors and adverse drug events.
STRATEGY FOR CHANGE
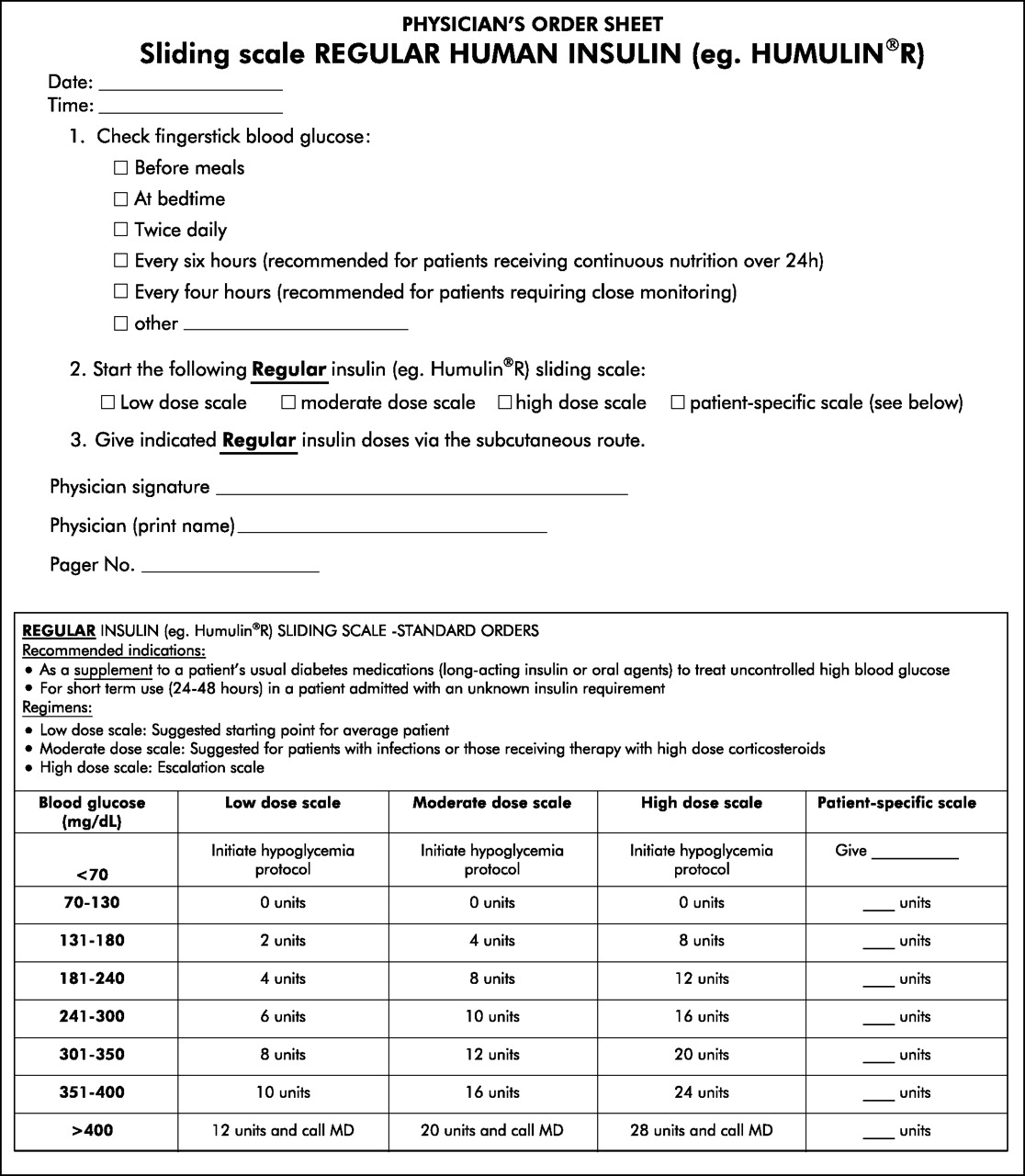
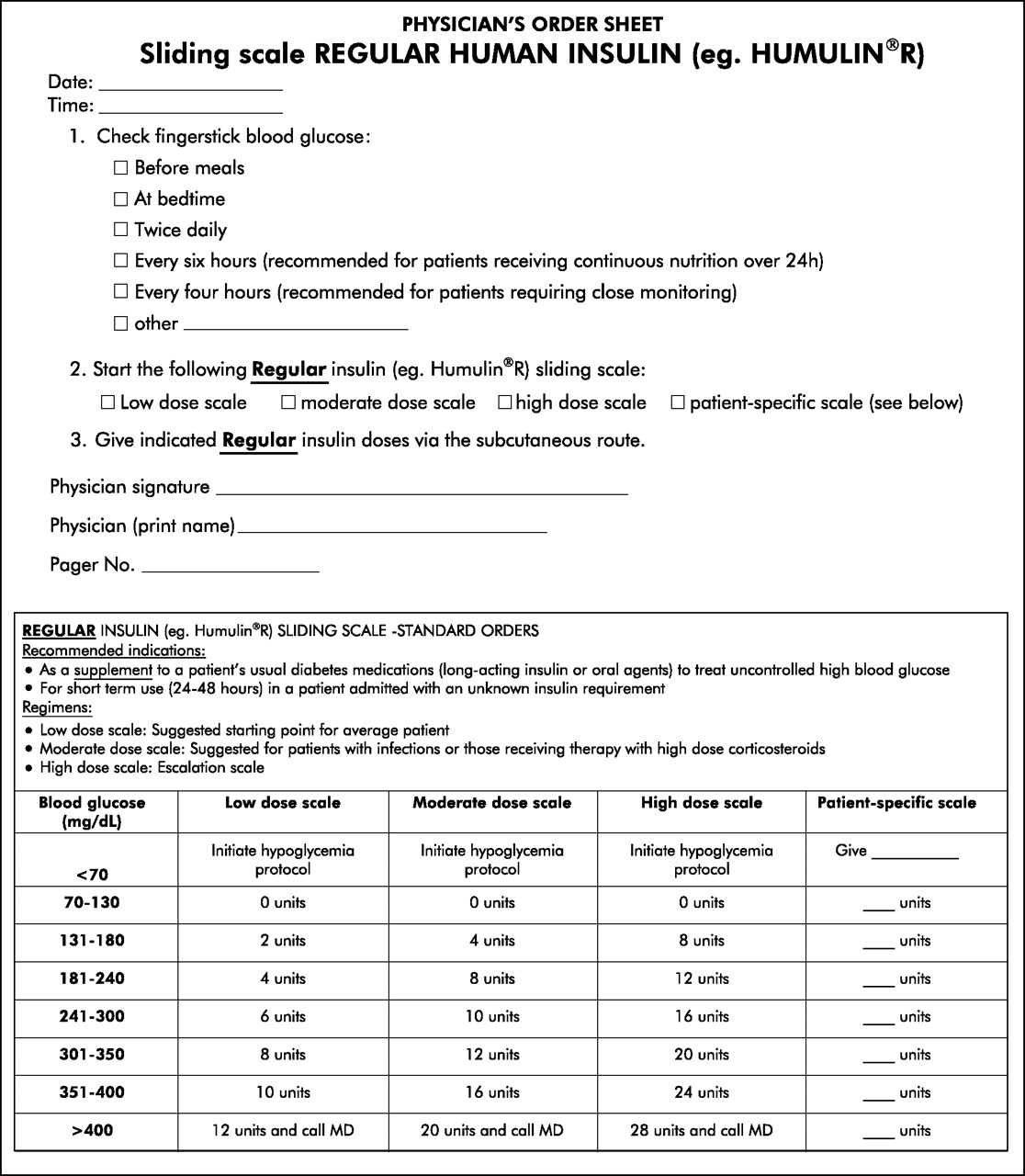
The goal of this quality improvement project was to develop, implement, and assess a standardized supplemental SSI protocol in non-intensive care units in order to reduce medication errors and prevent adverse drug events related to SSI. The interdisciplinary Diabetes Patient Safety Committee (DPSC) at our tertiary care center developed a sliding scale regular insulin (SSR) protocol for SSI which included the following guidelines: (1) SSI is indicated only as a supplement to patients’ usual glucose lowering medications or for short term use (24–48 hours) in patients admitted with unknown insulin requirements; (2) prescribers can choose one of three standardized regular insulin sliding scales (mild, moderate, high); and (3) these regimens start insulin coverage when the blood glucose level is >7.2 mmol/l (130 mg/dl). To help facilitate adherence to these guidelines, a preprinted SSR order form containing the guidelines as well as the standardized scales was developed (fig 1).
{kind=link}
Sliding scale regular insulin (SSR) order form.
The Medical Executive and Pharmacy and Therapeutics committees approved implementation of the SSR protocol on all non-intensive care units. Approval was obtained from the Patient Safety Committee to assess the impact of implementation as a quality improvement project.
Charts of patients prescribed SSI were reviewed at three time points (before implementation and 2 months and 1 year after implementation). Collected data included the presence or absence of the new SSR order form, prescribing errors, concurrent orders for basal insulin or oral glucose lowering agent, and all collected blood glucose data. Prescribing errors included use of “U” for unit or omitted insulin type.
The incidence of prescribing errors, hypoglycemia (blood glucose <3.9 mmol/l (<70 mg/dl)), and hyperglycemia (blood glucose 16.7 mmol/l (⩾300 mg/dl)) is reported as rate per 100 SSI patient-days. Incidence densities were compared using hypothesis testing.
EFFECTS OF CHANGE
Before implementation of the SSR protocol, more than 20 different types of SSI orders were used. Regular insulin was used in 98% of orders and the mean starting blood glucose level was 186 mg/l. On average, 65% of patients prescribed SSI had diabetes, 21% received concurrent corticosteroid treatment, 3% received total parenteral nutrition, and 9% received enteral nutrition support.
Within 2 months of implementation the SSR order form was used for 63.2% of SSI orders. One year after implementation it was used for 91% of orders. Overall, 79% and 86% of SSI orders followed the guidelines (regardless of order form use) at 2 months and 1 year, respectively, after implementation. For those patients taking oral glucose lowering agents at home, 87% and 71% continued these medications in hospital at 2 months and 1 year, respectively.
The number of prescribing errors found on chart review was reduced from 10.3 per 100 SSI patient-days at baseline to 1.2 at 1 year (p = 0.03, table 1). The incidence of hypoglycemia was 4.4 events per 100 SSI patient-days at baseline and 4.7 events per 100 SSI patient days at 1 year (p = 0.67). The incidence of hyperglycemia declined from 55.9 events per 100 SSI patient-days at baseline to 36.4 events per 100 SSI patient-days 2 months after implementation (p = 0.07); this fell further to 16.3 per 100 SSI patients-days 1 year after implementation (p = 0.0001 compared with baseline).
Number of prescribing errors, episodes of hypoglycemia, and episodes of hyperglycemia (per 100 SSI patient-days)
LESSONS LEARNT AND NEXT STEPS
Development and implementation of an SSR protocol was readily accepted and associated with decreased prescribing errors and decreased frequency of hyperglycemia. High acceptance of the protocol was probably due to the decrease in the amount of time required by prescribers to complete the order form (check a box) compared with writing out complete SSI orders. In addition, there was no associated increase in hypoglycemia as usage of the SSR protocol increased, despite the fact that insulin coverage started at a lower blood glucose level (7.2 mmol/l (130 mg/dl)) than previously used.
The incidence of hyperglycemia was decreased following implementation of the SSR protocol. It should be noted, however, that the incidence of 16.3 episodes of hyperglycemia per 100 SSI patient-days found 1 year after implementation is still high. Although the protocol specified that it should be used concurrently with the patient’s diabetes regimen, the appropriate escalation of these medications was not assessed. The most likely reason for hyperglycemia in hospitalized patients with diabetes is poor management of scheduled insulin or glucose lowering agents.
All patients who had basal insulin documented as a home medication were continued on basal insulin. In 29% of patients, home oral glucose lowering agents were held during hospitalization and scheduled insulin was not initiated. Although the reasons for holding home medications were not collected, some appropriate reasons may exist including holding metformin following surgery or contrast media, holding long acting sulfonylureas in the presence of acute renal failure, or holding thiazolidinediones during acute exacerbations of congestive heart failure. The DPSC is currently working on inpatient diabetes guidelines that will ensure that the duration of holding oral glucose lowering agents is minimized (that is, limited to instances when they are contraindicated) and, if they must be held, then basal/bolus insulin therapy is initiated in the setting of persistent hyperglycemia.
Prescribing SSI ensures that blood glucose levels are assessed several times a day to help identify the need for initiation or change in scheduled insulin or oral glucose lowering agents during the stressful time of hospitalization. The SSR protocol can serve as the correction insulin component as hospitals move toward recommended basal/bolus insulin prescribing.
Footnotes
-
Competing interests: M T Korytkowski has received the following from pharmaceutical companies that make insulin in the past five years: (1) consulting fees from Eli Lilly, (2) consulting fees and honoraria for speaking from Novo Nordisk, (3) honoraria for speaking engagements from Aventis, and (4) grant support from Aventis. There are no other competing interests to declare.
-
Parts of this study were presented as posters at the 38th American Society of Health-System Pharmacists Midyear Clinical Meeting, New Orleans, LA in December 2003 and the American Diabetes Association 64th Annual Scientific Sessions, Orlando, FL in June 2004.