Article Text

Abstract
Worldwide, more than 3 million children are infected with HIV and, without treatment, mortality among these children is extremely high. Both acute and chronic malnutrition are major problems for HIV-positive children living in resource-limited settings. Malnutrition on a background of HIV represents a separate clinical entity, with unique medical and social aetiological factors. Children with HIV have a higher daily calorie requirement than HIV-negative peers and also a higher requirement for micronutrients; furthermore, coinfection and chronic diarrhoea due to HIV enteropathy play a major role in HIV-associated malnutrition. Contributory factors include late presentation to medical services, unavailability of antiretroviral therapy, other issues surrounding healthcare provision and food insecurity in HIV-positive households. Treatment protocols for malnutrition have been greatly improved, yet there remains a discrepancy in mortality between HIV-positive and HIV-negative children. In this review, the aetiology, prevention and treatment of malnutrition in HIV-positive children are examined, with particular focus on resource-limited settings where this problem is most prevalent.
- HIV
- Nutrition
- Tropical Paediatrics
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Background
Infection with HIV is one of the greatest challenges to global health faced by the medical profession. There are 3.4 million HIV-positive children under 15 years of age and 340 000–450 000 new infections in the paediatric population each year.1 HIV infection is particularly aggressive in children—without access to treatment, more than half of HIV-infected infants die before the age of 2 years, with a median survival of only 23 months.2
Malnutrition affects over one-quarter of under 5s in the developing world and is thought to contribute to one-third of deaths in this age group—estimated at 1–2 million deaths per year.3 The majority of low-income countries (with the highest rates of malnutrition) have insufficient death certification, so this figure might be an underestimate.4 HIV infection and malnutrition often coexist, and the two conditions overlap and interact. Prevalence of concurrent HIV infection in children presenting with severe acute malnutrition (SAM) is variable, with figures of up to 71.8% reported.28 Meta-analysis of 17 large studies in sub-Saharan Africa suggested that 29.2% of children presenting with SAM were HIV-positive, although given the higher prevalence of HIV in this region, this might not be globally representative.5 Importantly, mortality from SAM is more than three times higher in HIV-positive children than their HIV-negative peers.5
SAM is defined by the WHO as a weight-for-height z-score of less than –3, or a mid-upper arm circumference of less than 11.5 cm in children aged 6 months to 5 years.6 SAM can present as non-oedematous (marasmus) or oedematous disease (kwashiorkor or marasmic-kwashiorkor), with marasmus being more common in HIV-positive children.6 ,7 In addition, HIV-positive children with SAM are at higher risk of infectious comorbidities (such as tuberculosis, respiratory tract infections, gastroenteritis and candidiasis) and other complications (such as persistent diarrhoea and poor oral intake).
This article sets out to discuss the aetiology of increased risk of malnutrition in HIV-positive children from both a medical and social viewpoint. It also aims to discuss management guidelines for this complex condition and preventive measures.
Aetiology of disease: medical
HIV-positive children have greater nutritional needs
When compared with HIV-negative counterparts, HIV-infected children (including asymptomatic children) have additional nutritional requirements to ensure normal growth and development and require high-energy, high-protein, nutrient-dense diets.8 Calorie intake needs to be increased, with children requiring up to 150% of the recommended daily allowance of calories, and micronutrient requirement is up to five times that of an HIV-negative child (table 1).8 It is recommended that—compared with HIV-negative children—asymptomatic HIV-positive children have a 10% increased calorie intake, which is best given through additional household foods, as part of a balanced, varied diet. HIV-positive children with chronic lung disease, chronic TB or chronic diarrhoea require approximately 20–30% increased calorie intake, which might be provided through increased household foods or through nutritional supplementation. Children with severe complications of HIV infection, such as SAM or stunted growth, require 50–100% increased energy intake each day, until weight is recovered. These increased nutritional demands reflect the increased nutrient cost of immune system support and prevention of muscle wasting. In resource-limited settings (RLS) where food availability is limited, it is clear that the increased nutritional requirements are unlikely to be met.
Daily calorie requirements of HIV-positive children
Diarrhoea and other infections
Acute, recurrent and chronic diarrhoea, and subsequent malabsorption, are common in HIV-positive children. Common infective organisms include bacteria (eg, salmonella, shigella, campylobacter), viruses (eg, rotavirus, adenovirus, CMV), parasites (eg, entamoeba, giardia, cryptosporidia) and fungi (eg, candida, histoplasma). Recurrent and chronic diarrhoea are, understandably, risk factors for the development of SAM and growth impairment.
Furthermore, malnutrition predisposes to gastrointestinal tract infection through gut mucosal barrier dysfunction, establishing a vicious infection-malnutrition cycle. Other infections—particularly pneumonia, which is also very common in HIV-positive children—have been found to contribute to the increased risk of malnutrition in children in several lower-income countries.9
Coinfection with HIV and Mycobacterium tuberculosis (TB) is an extremely common problem: TB is the largest single cause of death in HIV-positive individuals and, in areas of high prevalence, it is the most common coinfection in HIV-positive children.10–12 HIV and TB pathogens interact, resulting in an accelerated clinical course and premature death. TB infection results in secondary wasting: indeed, weight loss is the presenting feature in almost 50% of cases of TB and persistent anorexia is a feature in approximately one-quarter.13 Weight loss associated with TB is particularly marked in RLS. For example, in Malawi, TB patients had significantly lower body fat mass (35% lower) and 19% less lean body mass than matched controls, the extent of wasting being related to severity of TB infection.14 Furthermore, malnutrition is a risk factor for the acquisition of primary TB infection, as well as progression to active disease.
HIV enteropathy
HIV enteropathy is a unique disease entity caused by direct HIV-mediated and indirect cytokine-mediated damage to the gastrointestinal mucosa in the absence of pathogens. It can affect individuals at all stages of HIV infection and is characterised by chronic diarrhoea, gastrointestinal inflammation, increased intestinal permeability and malabsorption. HIV enteropathy causes typical histological changes, including lymphocytic infiltration of the epithelium, villous atrophy/blunting and crypt hyperplasia.15 Chronic diarrhoea and malabsorption caused by HIV enteropathy lead to malnutrition, which increases the risk of infective gastroenteritis; the interacting effects of infection and HIV enteropathy drive a vicious cycle that propagates malnutrition.16
Late presentation to medical services
In RLS, presentation to hospital for SAM—and other conditions—is often very late, with consequent poorer outcomes of medical intervention.17 In HIV-positive children, it has been observed that many SAM-related deaths occur within 1 week of admission, indicating the advanced stage of disease.18 The reasons underlying late presentation are complex and involve social, economic and cultural barriers, but it is likely that late presentation contributes significantly to the excess mortality seen in HIV-infected children with SAM.
Aetiology of disease: social
Wasting and malnutrition in HIV-positive children does not simply reflect interactions of biological processes, but includes a series of failures within the health system, the home and community.8
Food insecurity in HIV-positive households
Food security is defined as regular physical, social and economic access to sufficient quantities of safe and nutritious food, which meets the dietary requirements for a healthy life. When these conditions are not met, food insecurity is said to exist. A combination of reduced earnings due to frailty, reduced savings and assets, the high cost of antiretroviral treatment (ART) and high adult mortality causes food insecurity in HIV households. Food insecurity increases the risk of malnutrition in children in the household. However, employment and income among HIV-positive people increases after prolonged ART treatment, thus improving food security and nutritional status of all household members.19 ,20 A study of 30 000 HIV-positive people showed that treatment with ART resulted in recovery of employment to 90% of baseline compared with 37% before treatment was initiated.19
Children born to HIV-positive mothers not receiving ART have 2.5 times higher risk of dying before their second birthday than children of HIV-negative women, malnutrition being one contributing factor.21 In the developing world, women are the main caregivers and food purchasers/preparers in the family and, therefore, maternal illness from HIV contributes to malnutrition in children. Timely initiation of ART in HIV mothers has, however, been shown to reduce under five mortality rates to levels similar to those of children of HIV-negative women.22 A large study in rural South Africa demonstrated that the under 2s mortality rate fell significantly following the initiation of maternal ART—this being the most important contributing factor to the decline in paediatric mortality.23 It is clear, therefore, through the effects of food security and maternal HIV that all children in HIV-positive households are at greater risk of malnutrition than children in households where neither parent has HIV/AIDS.
Barriers to accessing healthcare
A major contribution to the excess mortality due to malnutrition in HIV-positive children is the inaccessibility of timely and appropriate medical services. The barriers to access of medical care are plentiful and vary on regional, country and district levels.
There is a paucity of hospitals and healthcare facilities in poorer countries, meaning that distances that individuals must travel to access healthcare can be great. Distance and transport are reported as the major barriers to accessing maternal and paediatric health services in many developing countries.24 ,25 In addition to the cost of transport, a major financial barrier to treatment for both HIV and malnutrition is the cost of medical treatment in countries where public healthcare is not available; this can ostracise the poorest in the community.
Although there are relatively few good studies into the effects of stigma on HIV-positive individuals, it is accepted that stigma is ubiquitous to people living with HIV/AIDS (PLWHA) and this offers a constant barrier to treatment. Efforts to reduce prejudice and discrimination in health workers involved in HIV management, as a mode to reduce stigma, have been met with unremarkable results.26
Suspicions and fear surrounding ‘Western’ medicine and health interventions have been reported in Zambia and represent another barrier to healthcare provision to HIV-positive children.27 Fear of Western science and medicine has also been observed in clinical trials from across the developing world and is indicative of a far greater and complex problem that impacts on management of malnutrition in HIV-positive children.28 The roots of this have been mooted from many different anthropological, political and sociological approaches, discussion of which is beyond the scope of this article.
Prevention and treatment of malnutrition in HIV-positive children
Best practice in infant feeding
A safe and effective infant feeding regimen that minimises the risk of HIV transmission needs to be implemented in all children born to HIV-positive mothers. Where infection has already occurred, best practice feeding regimens reduce the risk of HIV-associated malnutrition. It is estimated that up to 40% of cases of vertical transmission in sub-Saharan Africa have occurred via breast feeding.29 The feeding of a child born to an HIV-positive mother must be analysed on an individual and contextual basis, following published guidelines (table 2). Overall, exclusive breast feeding for the first 6 months is recommended for HIV-positive mothers unless replacement feeding is acceptable, feasible, affordable, sustainable and safe (AFASS, figure 1).30 Treatment with ART minimises the risk of vertical transmission.
Best practice infant feeding regimens for children born to HIV-positive mothers, based on WHO guidelines52–53
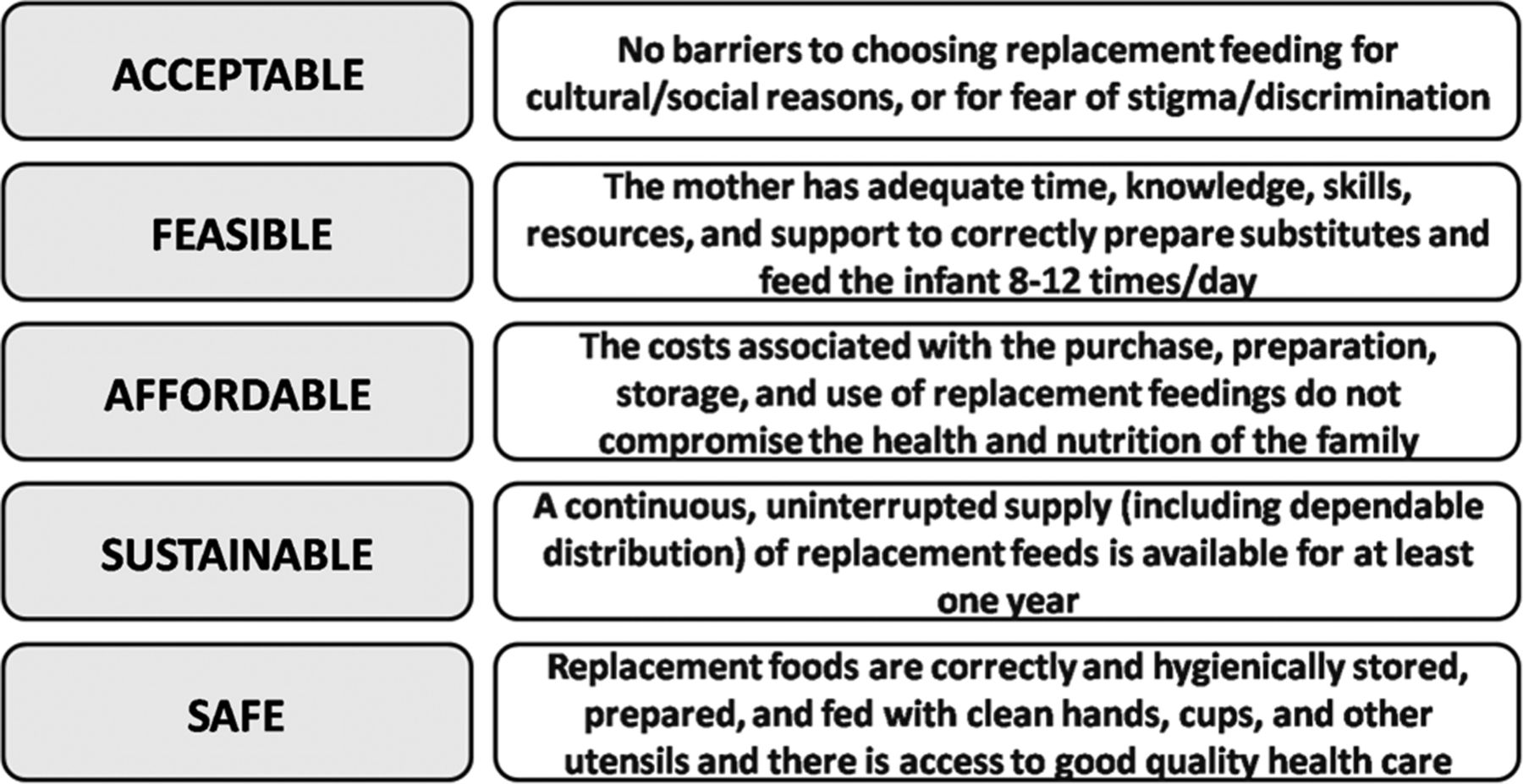
Infants under the age of 6 months born to HIV-positive mothers should be exclusively breast fed unless breast milk substitutes fulfil the acceptable, feasible, affordable, sustainable and safe criteria, as defined by the Joint United Nations Programme on HIV/AIDS.36
It is imperative that mixed feeding (ie, part breast; part formula or semisolid foods) is avoided in the first 6 months of life; this is particularly crucial when ART is unavailable or unacceptable to the mother. In children under 6 months, a mixed feeding regimen of breastmilk and formula milk resulted in an approximately twofold increased risk of vertical transmission of HIV, while mixed feeding with solids increased the risk to 11-fold.31–34 Vertical transmission of HIV occurs when virus present in the milk infects children through the intestinal mucosa. It has been suggested that the use of formula milk and/or solid foods interferes with the integrity of the infant intestinal mucosa, thereby increasing the risk of vertical transmission.31 ,35 On the other hand, cessation of breast feeding before 6 months has been implicated in increased infant mortality, especially from diarrhoea.36 In high HIV endemic areas, there is emerging evidence that feeding practices differ significantly from these recommendations. In South Africa, for example, less than 8% of infants under 6 months old are exclusively breast fed.37
Education regarding prevention of HIV transmission and optimal infant feeding regimens are crucial for the prevention of malnutrition. Infant feeding and nutrition has been identified as a major concern for women living in RLS, which suggests that women would be receptive to such education programmes.38 It is particularly helpful if the female educator is a positive role model, whose own children are thriving despite also living in poor conditions, as this has a significant and lasting effect on the rates of recovery from malnutrition in both rural and urban settings in developing countries around the world, including South Africa, Bangladesh and Haiti.39 ,40
Treatment of SAM
When preventative strategies fail, either community-based or hospital-based therapies need to be implemented to prevent mortality from SAM. The community-based approach involves provision of treatment for those without medical complications with ready-to-use therapeutic foods (RUTFs) or other nutrient-dense foods at home. Hospital or special facility-based approaches are required for severely malnourished HIV-positive children with medical complications, including children with reduced appetite or coexisting infections.
The treatment regimen for SAM of HIV-infected children should follow the WHO guidelines.41 It involves initial stabilisation of the child, followed by a rehabilitation phase. During the initial stabilisation phase, life-threatening problems are identified and treated, with the aim of reducing oedema and restoring organ function.41 ,42 Key steps include treatment of infections, caloric replacement (such as F75, discussed later) sufficient to prevent loss of further muscle and fat and correction of electrolyte imbalance. Treatment of acute infection during the stabilisation phase is of particular importance as comorbidities such as gastroenteritis, malaria, pneumonia, bacteraemia (30%) and other invasive bacterial diseases complicate a large proportion of early deaths in children admitted for SAM.42
Treatment of TB infection is a crucial step in treatment of SAM as it in itself can cause significant wasting. A further infection that warrants particular attention is oesophageal candidiasis, which affects approximately 10% of HIV-positive individuals at some point.43 Oesophageal candidiasis causes dysphagia and odynophagia, which can lead to poor oral intake and subsequent wasting, and, as such, treatment of any concurrent oral or oesophageal candida infection is an important part of treatment of SAM.
The rehabilitation phase involves gradual introduction of foods, use of high-calorie nutritional formulas (such as F75, F100) and micronutrient/vitamin supplementation. The rehabilitation phase primarily comprises 6–10 weeks of therapeutic feeding with 50–100% increased calorie intake, as well as holistic assessment of the child's health, HIV therapy and family setting (table 1, figure 2). Alternatively, for children with uncomplicated malnutrition, community or outpatient-based treatment with RUTF can be initiated. The major benefit of RUTF is that it addresses the major problem of lack of access to inpatient facilities and allows timely intervention.

{kind=link}
{kind=link}
Guidelines for treatment of severe malnutrition in HIV-positive children, based on WHO guidelines.8 ,41 Although early initiation of antiretroviral treatment is advocated in these guidelines, this remains controversial, and delaying initiation of treatment until after the acute phase might be prudent.
There has been some controversy surrounding the efficacy of malnutrition treatment regimens in HIV-positive children, with mortality remaining approximately three times higher in HIV-positive children than HIV-negative children, regardless of treatment setting.5 The excess mortality observed is likely to be due to concurrent infections and other medical complications of HIV infection. Surprisingly, meta-analysis showed that mortality rates among HIV-positive children in hospital settings compared with those receiving community-based treatment were identical.5 These data will need to be re-evaluated once there has been widespread implementation of the guidelines specific to HIV-positive children. It is hoped that these guidelines will reduce the discrepancy in mortality between HIV-positive and HIV-negative children.
Correct timing of initiation of ART
In recent years, there has been a dramatic increase in the proportion of HIV-positive individuals on treatment: for example, in one hyperendemic region in Southern Africa, since the ART programme ‘scale-up’, there has been an increase from 0% in 2004 to 31% in 2011.44 Use of ART has led to a decrease in morbidity and mortality in HIV-positive children in RLS. Despite widespread advances in the availability of ART, there remains a disparity between the number of children who require ART and the number receiving treatment; furthermore, initiation of therapy occurs late in children with already advanced disease.5 Initiation of ART is associated with a sustained improvement in growth responses, especially in younger children, even in the absence of complete viral suppression.45–47 The direct effect of ART on growth, as well as the decreased frequency of opportunistic infections in children receiving ART, means that absence (or late initiation) of ART treatment can be considered a risk factor for development of malnutrition in HIV-positive children.
This is a controversial area as there have been several reports showing that severe malnutrition was precipitated in the months following ART initiation.48 ,49 One study reported that approximately 10% of HIV-positive children were hospitalised for severe malnutrition within 12 weeks of starting ART.48 Furthermore, an unusually large proportion of these children developed oedematous malnutrition (kwashiorkor), and it has been argued that this is because a degree of immune competence is required to develop oedema.50
It was postulated that the SAM observed might represent a form of immune reconstitution syndrome (IRIS) in children with underlying chronic malnutrition and severe immunosuppression.48 This is supported by a large study in Peru of children initiating ART, where children with IRIS were more likely to develop one or more indicator(s) of malnutrition compared with children without IRIS, this effect being more significant in children under 5 years of age.51 Another plausible explanation is that the development of malnutrition following initiation of ART represents a variant of re-feeding syndrome or an unusual antiretroviral toxicity reaction.48
Further research is required to establish the pathogenesis of this phenomenon and to determine the optimal time of ART initiation in children with underlying malnutrition in order to avoid rebound complications. Until there are clear evidence-based guidelines, it would seem prudent to treat SAM and acute medical problems with initiation of ART once the child is stabilised.
Conclusions
Malnutrition is a major threat to the health of children living in RLS and is responsible for up to 2 million deaths per year in children under 5 years of age. Malnutrition on a background of HIV infection is a complex medical condition that carries significant morbidity and mortality for affected children, with greater mortality from SAM among HIV-positive children than their HIV-negative peers. It is crucial that research continues into the pathogenesis of SAM on a background of HIV infection as this will allow the establishment of more effective care pathways for complicated SAM, thereby decreasing the disparity in mortality between HIV-positive and HIV-negative children. Furthermore, given that there is high HIV prevalence among children with SAM, HIV testing should be considered in all children from high-risk areas who present with SAM.
Prevention of mother-to-child transmission of HIV remains one of the most important interventions to improve global child health. In particular, an increase in exclusive breastfeeding rates would lead to decreased vertical transmission. Education and support for mothers of HIV-positive children is crucial, especially with regards to infant breastfeeding practices. Support should also be given to help meet the increased daily nutritional needs of HIV-infected children in order to prevent development of SAM. Government-level interventions to improve healthcare infrastructure and assure food security are other important steps in the prevention of malnutrition in HIV-positive children.
Coinfection is another major contributor to SAM in HIV-positive children, and efforts to reduce number of infections, such as gastroenteritis (eg, through water sanitation), are important. Given the complex and detrimental interaction between HIV, TB and malnutrition, the global fight against mycobacterial infection must continue, and a decrease in TB incidence might improve nutrition among HIV-positive children. Finally, although it is clearly beneficial to start HIV-positive children on ART, the question of when this therapy should be initiated in children with SAM needs to be addressed. Further research needs to be conducted into the correct timing of therapy in order to maximise the benefits of treatment while minimising the risk of rebound malnutrition.
References
Footnotes
-
Contributors AMR and NM-A were responsible for review design and critical appraisal and editing. AMR and CSH were responsible for writing and production of figures and tables.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.