
ABSTRACT
BACKGROUND
Bioethicists and professional associations give specific recommendations for discussing cardiopulmonary resuscitation (CPR).
OBJECTIVE
To determine whether attending hospitalist physicians’ discussions meet these recommendations.
DESIGN
Cross-sectional observational study on the medical services at two hospitals within a university system between August 2008 and March 2009.
PARTICIPANTS
Attending hospitalist physicians and patients who were able to communicate verbally about their medical care.
MAIN MEASURES
We identified code status discussions in audio-recorded admission encounters via physician survey and review of encounter transcripts. A quantitative content analysis was performed to determine whether discussions included elements recommended by bioethicists and professional associations. Two coders independently coded all discussions; Cohen’s kappa was 0.64–1 for all reported elements.
KEY RESULTS
Audio-recordings of 80 patients’ admission encounters with 27 physicians were obtained. Eleven physicians discussed code status in 19 encounters. Discussions were more frequent in seriously ill patients (OR 4, 95% CI 1.2–14.6), yet 66% of seriously ill patients had no discussion. The median length of the code status discussions was 1 min (range 0.2–8.2). Prognosis was discussed with code status in only one of the encounters. Discussions of patients’ preferences focused on the use of life-sustaining interventions as opposed to larger life goals. Descriptions of CPR as an intervention used medical jargon, and the indication for CPR was framed in general, as opposed to patient-specific scenarios. No physician quantitatively estimated the outcome of or provided a recommendation about the use of CPR.
CONCLUSIONS
Code status was not discussed with many seriously ill patients. Discussions were brief, and did not include elements that bioethicists and professional associations recommend to promote patient autonomy. Local and national guidelines, research, and clinical practice changes are needed to clarify and systematize with whom and how CPR is discussed at hospital admission.
Similar content being viewed by others

INTRODUCTION
Cardiopulmonary resuscitation (CPR) was developed to sustain cardiac and respiratory function in patients who suffered cardiac arrest as a result of reversible conditions. In patients with terminal illness, CPR may prolong, but cannot reverse, the dying process.1 An ethical and legal consensus developed that CPR may be withheld upon request of patients or surrogates.2–4 Recommendations promulgated in the 1980s and supported by professional organizations to date1,5 state that to respect patient autonomy, physicians should discuss CPR with patients at risk for requiring it and cover several specific elements.1,2,5,6 To set the stage for the discussion, physicians should discuss and ensure that patients understand their prognosis; the discussion should also elicit values and goals for care. The physician should explain and confirm that the patient understands the nature of CPR, their likelihood of requiring it, and its risks, benefits, and possible outcomes. Finally, the physician should make a recommendation about CPR that is consistent with the patient’s prognosis and goals for care.
Studies conducted over 15 years ago suggested that these recommendations were not routinely followed. Physicians were frequently unaware of hospitalized patients’ preferences for CPR,7 and medical residents’ discussions of code status rarely included preferences, risk, benefits, outcomes, or a physician recommendation.8 Today, notwithstanding the wide dissemination of educational initiatives,9,10 growth of the hospitalist movement,11–13 and introduction of palliative care services,14,15 many hospitalized patients at risk for requiring CPR still do not have code status discussions documented in their medical records.16–18 Moreover, residents continue to report challenges with incorporating the recommended elements into discussions of code status.10
This study (1) describes a consecutive series of patients with whom attending hospitalist physicians discussed code status at hospital admission and (2) evaluates whether these discussions met the above recommendations.1,2,5,6
METHODS
Design
We conducted a cross-sectional observational study of communication between attending hospitalist physicians and their patients in admission encounters.19 To describe code status discussions in these audio-recorded encounters, we performed a quantitative content analysis.20–22
Setting and Participants
The study setting was the general medical services at two hospitals within a university system where attendings care for patients with trainees (Hospital A) and without trainees (Hospital B). Hospitalists attending on the medical service were eligible and recruited before their rotation. Eligible patients were: (1) admitted under a participating hospitalist, (2) able to communicate verbally about their medical care, and (3) preferred to communicate in English without a translator. We excluded patients who were unable to provide informed consent or communicate verbally (severe hearing impairment, speech disorder, tracheotomy). Patients were identified on all weekdays between August 2008 and March 2009, and approached in the emergency room or their hospital room for screening and enrollment. To avoid interfering with patient care, we allowed physicians, at their discretion, to decline audio-recording on certain days or with certain patients. The Institutional Review Board at the University of California, San Francisco, approved the study, and physician and patient participants gave written informed consent.
Data Collection and Measures
At enrollment, physicians completed a written survey including demographics, and patients completed a written survey including demographics and a brief measure of self-evaluated health: “How would you describe your current health?” (relatively healthy/seriously but not terminally ill/seriously and terminally ill).23 The attending-patient admission encounter was audio-recorded. After the encounter, the physician completed a written survey indicating whether code status was discussed and verifying the patient’s code status. To identify seriously ill patients, we asked physicians whether: (1) the patient had a terminal illness, and (2) “Would you be surprised if this patient died or was admitted to an ICU within the next year?”24 We also asked physicians to estimate the likelihood that the patient would require CPR during the hospitalization.
Analysis
We identified code status discussions by review of transcribed audio-recordings and from physician post-encounter surveys; these agreed in all cases except for one, in which a discussion was reported on the physician survey that could not be identified in the transcript. To describe associations between patient and physician factors and whether code status was discussed, we used generalized estimating equation logistic regression models with robust standard errors and adjustment for clustering within physician.25 Due to the small sample size and event rate, we limited each model to one predictor in addition to a fixed effect for hospital.26 All statistical analyses were performed with Stata 11 (StataCorp LP, College Station, TX).
To reliably identify presence or absence of elements within the code status discussions, we developed a standardized, explicit coding scheme using an iterative process.20–22 Analysis focused on the transcript portion that included the code status discussion; however, each entire encounter was reviewed to identify related topics, such as discussion of prognosis. First, we identified elements of the code status discussion based on past work and expert and professional recommendations (e.g., discussion of prognosis, goals, and values, elements of informed consent, and physician recommendation).1,2,5,6,8,27–30 Next, we read all transcripts to identify additional elements (e.g., how the topic of CPR was introduced, decision-making process, and outcome). Salient codes were established by consensus among all authors. A draft codebook was tested on a subset of three discussions and modified for clarity. The final codebook was applied independently to all discussions by two coders. Cohen’s kappa for agreement was 0.64–1 for all reported elements, indicating substantial to almost perfect agreement.31,32 Agreement was highest for elements whose presence or absence could most objectively be established (e.g., whether prognosis was discussed, whether the physician gave a recommendation) and lower for elements that required more interpretation (e.g., whether risks, benefits, and outcomes of CPR were discussed). Disagreements in coding were resolved by consensus between the two primary coders; a third coder was available to adjudicate if consensus could not be reached.
RESULTS
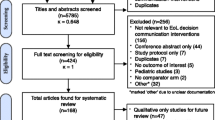
Of 35 eligible physicians, 32 consented, and 27 cared for at least 1 patient who consented (Table 1). We identified 441 patients, screened 210, found 171 to be eligible, and audio-recorded 80 encounters. We did not audio-record 91 eligible encounters because: (1) the patient did not consent (n = 64), (2) the physician declined participation for that day or patient (n = 24), or (3) the encounter occurred after-hours (n = 3). Patient characteristics did not differ by whether the encounter was audio-recorded. Physicians reported that 23 patients had a terminal illness, and that they would not be surprised by the death or ICU admission of 35 within the following year.
Eleven physicians discussed code status in 19 encounters. Most discussions occurred with patients whom the physician felt had a low likelihood of requiring CPR during the hospitalization (Table 2). Physicians were more likely to discuss code status at Hospital B (attendings only) than Hospital A (attendings and trainees), OR 27 (95% CI 5–134). Controlling for hospital, physicians more frequently discussed code status with older patients and patients whose ICU admission or death within the following year would not surprise them, OR 1.04 per year of age (95% CI 1.01–1.07) and OR 4 (95% CI 1.2–14.6). However, 23 (66%) of the patients whose ICU admission or death within the following year would not surprise the physician did not have a discussion.
Code status discussions lasted a median of 1 min (range 0.2–8.2), corresponding to a median of 4% (range 1%–22%) of the encounter. Table 3 summarizes main findings of the discussion content analysis; a detailed account, including exemplar quotations, follows. Physician and patient identification labels correspond to their order of appearance in the manuscript, not study enrollment.
Introduction of the Topic of Code Status
In 18 discussions, the physician introduced the topic of code status; in the remaining discussion, the patient volunteered that he had a Do Not Resuscitate (DNR) order after the physician inquired about his health care power of attorney. Physicians usually discussed code status toward the end of the encounter, along with surrogate decision-makers (n = 11), and advance directives (n = 5). In 14 discussions, physicians told patients that they discussed code status with all patients:
PHYSICIAN: And we ask everyone these questions when they come into the hospital, just so I know, in case of an emergency. In case of the worst possible scenario, if you should stop breathing or your heart should stop, have you thought, before, about what you would want doctors to do?
Hospital B: Physician A, Patient 1, a 47-year-old woman with end-stage renal disease admitted for observation after dialysis catheter placement
Discussion of Prognosis and Patient Values, Goals, and Preferences
Only one encounter addressed both code status and prognosis. Here, the patient raised prognosis because he found it difficult to decide about code status without knowing his overall prognosis.
PATIENT: [My oncology physicians] really haven’t provided much information on prognosis…I think that’s a discussion that I need a little more information. It’s still a little abstract. I mean, my general thing [is] to say, “No, I don’t want heroic measures.”…But that seems like a fairly drastic response, unless it’s just…I mean, you know, I just don’t feel like I know what the words mean enough to know what I’m saying.
Hospital B: Physician B, Patient 2, a 60-year-old man with metastatic cancer admitted with failure to thrive
Discussions of preferences for end-of-life care focused on the use of life-sustaining interventions, as opposed to larger life goals. Patients mentioned quality of life, but neither defined it nor characterized acceptable functional status. Physicians accepted these vague references without prompting patients to elaborate.
PATIENT: My basic position has been that I do not want my life extended…[there is a] serious question as to whether I would be able to return to a relatively normal or natural life. I don’t want any artificial means taken to extend my life, if it’s not going to extend the quality of my life.
PHYSICIAN: I see. I ask because some people absolutely don’t want anything done. And other people say, “Do everything.” And there’s a lot of gray in between. So I want to make sure we respect your wishes. But I think I have a sense of where you’re coming from.
Hospital B: Physician C, Patient 3, a 78-year-old man with squamous cell skin cancer admitted with dehydration and failure to thrive due to oral pain after radiation therapy
CPR as an Intervention: Elements of Informed Consent
Physicians framed indication for CPR in general terms, such as “emergency” or “if something unexpected should happen,” along with phrases such as, “if your heart were to stop” or “you couldn’t breath on your own.” The words “death” or “die” appeared in only two discussions. No physicians described specific scenarios in which the patient would be likely to require CPR. Estimations of the likelihood that the patient would require CPR, present in nine discussions, in all cases took the form of reassurance that the physician did not think that the patient would need it.
PHYSICIAN: And then the other question, again I ask everybody and I don’t think this is gonna be an issue, but, in the event of an emergency, if your heart were to stop working or you were to stop breathing would you want us to do CPR for you?
Hospital B: Physician D, Patient 4, a 50-year-old man with abdominal pain and diarrhea, admitted for workup of possible malignancy
When describing CPR as an intervention, undefined jargon, such as “resuscitation,” “CPR,” and “compressions,” was used. In three discussions, physicians stated that the default protocol would be to perform CPR. In five discussions, a distinction was made between short- and long-term use of life-sustaining therapy. However, physicians did not always clarify that the outcome of CPR for any individual patient is unpredictable.
PHYSICIAN:…if an emergency were to happen…and your heart would [stop] or your breathing became so difficult that you needed to be attached to machines, would you want the nurses and doctors to attempt heroic measures to try to restart your heart and attach you to a breathing machine?
PATIENT: Technically not…because okay, if it’s a temporary thing that, you know, if you restart the heart and it’s okay again but if it means the end really and you’re just prolonging it, then no.
PHYSICIAN: Okay. So if the doctors think that we might be able to get you back easily, then we should try?
PATIENT: Yeah.
PHYSICIAN: Okay. Okay. That makes sense.
Hospital B: Physician E, Patient 5, an 85-year-old woman admitted with a pelvic fracture after a fall
Risks, benefits, and possible outcomes of CPR were mentioned in six discussions. Physicians described possibilities of recovering and requiring life support.
PHYSICIAN: Sometimes we do a few things to see if we can get your heart started again and kind of revive you and sometimes that means you end up in the intensive care unit on machines for a few days, but some people do get better from that.
Hospital A: Physician F, Patient 6, a 72-year-old woman with central nervous system lymphoma admitted for inpatient chemotherapy
In no case did the physician provide a likelihood of survival after CPR. Patients used terms such as “vegetable” or “invalid” to describe possible outcomes of CPR, but physicians did not explore their meaning.
PATIENT: Well, if I was gonna be an invalid for the rest of my life, I would not want any part of being resuscitated.
PHYSICIAN: But if it is something that, for surgery, for example, if you needed to have the breathing machine, to have a small surgery…you might consider it for that circumstance.
Hospital A: Physician G, Patient 7, an 88-year-old woman admitted with pancreatitis
Physician Recommendation, Decision-Making, and Outcome of the Discussion
In no discussion did the physician make a recommendation about the use of CPR. We categorized patients’ initial stated preferences about code status as: full code (n = 7), DNR (n = 6), unsure (n = 3), and unclear (n = 3). In all seven cases in which the patient initially expressed a preference for full code, the physician did not pursue the topic further.
PHYSICIAN:…if for some reason you got so sick that your heart stopped beating or your lungs got so sick that they couldn’t breathe on their own, would you want us to attempt to bring you back to life with electricity shocks and other things?
PATIENT: Yes.
PHYSICIAN: Yes. Okay. Okay. I think that’s all my questions.
Hospital B: Physician H, Patient 8, a 67-year-old woman with cholangiocarcinoma admitted with fever and abdominal pain
In four of the six instances in which the patient initially expressed a preference for DNR, the physician explored preferences for short- versus long-term use of life-sustaining therapy. This exploration changed the patient’s preference from DNR to full code in three of four cases.
PHYSICIAN: In case of the worst possible scenario, if you should stop breathing or your heart should stop, have you thought, before, about what you would want doctors to do?
PATIENT: Yeah. I don’t want them to go to a lotta trouble. And I need a priest.
PHYSICIAN: You need a priest. So you don’t want to be resuscitated?
PATIENT: Yeah…well, not if I’m gonna be like frozen if they resuscitate me, you know what I mean?
PHYSICIAN: OK, but in the moment, we often don’t know that. So, do you want us to give it like the best try we can–
PATIENT: Oh yeah.
PHYSICIAN: OK. So we will do all the resuscitation and then we can think later, if things don’t get better down the line. But in the immediate sense, if you should stop breathing or if your heart should stop, you would want us to try to…
PATIENT: Sure.
Hospital B: Physician A, Patient 1, a 47-year-old woman with end-stage renal disease admitted for observation after dialysis catheter placement
In all three cases in which we designated the patient’s initial preference as “unsure,” the physician explored further. In the three cases with an initial “unclear” patient preference, the physician did not pursue the topic further.
We categorized the final outcome of the discussions as full code (n = 11), DNR (n = 3), deferred (n = 1), and unclear (n = 4). In the four discussions for which the outcome was unclear, the coders could not determine what the physician planned to order for the patient’s code status; in all of these cases the physician reported the code status as full code on the post-encounter survey. Otherwise, there were no discrepancies between the coded discussion outcome and the physician’s post-encounter survey response.
DISCUSSION
We identified and analyzed the content of code status discussions in audio-recordings of admission encounters between 80 patients and 27 attending hospitalists at 2 hospitals within a university system. As to patients with whom physicians discussed code status, our findings mirror past studies: rates of discussions varied between hospitals,16,33 and physicians were more likely to discuss CPR with older and more seriously ill patients,16 yet many patients with serious illness and a higher likelihood of requiring CPR did not have discussions.16–18 The content of the discussions closely resembles resident physicians’ communication about code status.8,10 Discussions were brief and did not include elements recommended by bioethicists and professional associations, particularly: (1) discussion of prognosis and goals for care, and (2) a physician recommendation.1,2,5,6 These findings suggest that physician experience does not affect the content of CPR discussions. Further, despite 15 years of hospital-based initiatives aimed at improving communication about serious illness,9–15 little has changed in how code status is discussed.
Variability in rates of discussions across providers, hospitals, and institutions may reflect lack of clarity in guidelines. The practice of discussing or attempting to discuss code status with all patients at hospital admission, as rates in one of our hospitals suggest, has been reported by residents at academic centers.34 This may be a response to the Patient Self-Determination Act, which requires hospitals to ask patients about and offer to help complete advance directives.35 Ethical and professional association guidelines, however, specifically state that CPR should only be discussed with patients who are at risk for requiring it.1,2 Code status and advanced directives are related, but not synonymous. Advance directives state preferences for care to be provided in the event of terminal, irreversible illness where the patient is unable to communicate their wishes; DNR orders are physician orders that dictate care only during the current hospitalization.1,6,36 Given patient admission volumes, requiring code status discussions with all admitted patients may, in part, cause physicians to have short discussions that do not include the recommended elements.
Short discussions that fail to include the recommended elements engender significant problems. Patients do not understand CPR as an intervention and the decision they are being asked to make,10,17,37 and seriously ill patients overestimate their prognosis,38 as well as survival after CPR.17 Patients who understand their prognosis and the rate of survival after CPR are less likely to desire life-sustaining therapies in general, and CPR specifically.6,38,39 Discussions that do not include the recommended elements yield, at best, a decision for full code, the default without a discussion. At worst, brief discussions may reinforce misinformation about the effectiveness of CPR,40 which may negatively impact future discussions.
The lower rate of discussions at Hospital A may reflect the fact that, at this hospital, residents evaluated, and may have discussed code status with, patients prior to the audio-recorded attending-patient encounter. Should attendings repeat code status discussions if residents have already performed them? While repetition may increase the burden to patients and decrease resident autonomy, the attending is both ethically and legally responsible for writing the DNR order. Prior studies raise concern that resident CPR discussions are ineffective at promoting patient autonomy.8,10 Thus, we believe that an independent attending-patient discussion of code status is particularly warranted for patients who request DNR status and/or who the attending feels are likely to require CPR or have a poor outcome from it. Involving trainees in these discussions is an opportunity for modeling best-practice discussions.
How can we improve the quality of code status discussions? Past studies have cited deficiencies in medical training as a barrier to communication about end-of-life issues.33,41–44 Gaps are apparent at conceptual and skill levels. Accurately assessing and communicating prognosis appear particularly challenging for physicians.45 This creates a bias toward seriously ill patients receiving CPR, as they are less like to refuse it if they do not understand their prognosis.6,38,39 Residents report not getting feedback on code status discussions,42 and feel uncomfortable with such aspects as making a recommendation about CPR and handling patients’ emotional responses.10 Similarities observed between the content of attendings’ and residents’ communication indicate that trainees learn by modeling and are not exposed to code discussions that meet recommendations. In the outpatient setting, research described best practices for advance care planning by observing discussions of experts in bioethics and communication.30 This approach should be adapted to the inpatient setting, to describe how to accomplish recommendations for discussing code status. Communication-training programs should then be designed using proven methods to teach these skills.46–48
Further research should focus on patient perceptions of the utility and relevance of ethical and professional association recommendations. It is unclear whether patients would have a clearer understanding of CPR after discussions that incorporate expert recommendations. This should be empirically evaluated, along with outcomes as to the decisions patients ultimately make and whether care is then better aligned with their goals and values. Systems-level interventions to support best-practice CPR discussions are needed. The admission encounter is a particularly challenging interaction for hospitalists, who are meeting patients for the first time, often after patients have interacted with a number of other providers. Hospitalists must immediately build rapport with the patient and discuss the medical plan along with patient concerns. These tasks require a significant amount of time, and adding a code status discussion that includes goals, values, prognosis, and a recommendation may be particularly challenging. Further, discussions of prognosis and life-sustaining therapies should be informed by input from outpatient primary care and specialist providers such as oncologists; however, reaching them in advance of the admission encounter is often not possible.
Our study has several limitations. First, we only captured communication in the initial attending-patient encounter and did not review patients’ medical records for documentation of prior code status discussions. The discussions we audio-recorded may have been brief because the attending was verifying a decision that was made during a past hospitalization, with an outpatient physician, or with a resident, although no attending referred to such a discussion. It is also possible that attendings had more prolonged discussions in a subsequent encounter. Discussions for seriously ill patients may have been deferred to specialists such as oncologists or palliative care physicians. Second, we did not record a number of encounters because we were unable to screen all patients before the attending encounter or because physicians declined participation on certain days or with certain patients. Physicians who were newer to the medical service or who were experiencing a busy clinical day were most likely to decline audio-recording; yet it is unlikely that physicians in these situations were more likely to discuss code status or to have longer, more involved discussions. Further, we were able to collect at least one audio-recording from all participating physicians who cared for a consenting patient. Third, our results are based on discussions of physicians within one system. Though the consistency of our findings with other studies supports their validity,8,10,22 code status discussions should be studied at other academic and non-academic institutions with larger numbers of physicians.
Our results suggest numerous avenues of intervention to improve the content and delivery of code discussions. There is a need to clarify guidelines, at both national and institutional levels. As a first step, we recommend that efforts target patients who are at high risk for requiring CPR or having an outcome that is worse than average.49,50 Limiting discussions to these patients as opposed to trying to discuss code status with all admitted patients may encourage longer discussions in which prognosis and overall goals of care can be explored.
REFERENCES
Guidelines for the appropriate use of do-not-resuscitate orders. Council on Ethical and Judicial Affairs, American Medical Association. JAMA. 1991;265(14):1868-1871.
The President’s Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioural Research: Deciding to Forego Life Sustaining Treatment 1983.
Meisel A, Cerminara K. Right to Die: the Law of End-of-Life Decisionmaking. 3rd ed. New York: Aspen Publishers; 2009.
Reich, Warrent T. (Ed) Encyclopedia of Bioethics. 3rd ed. New York: Macmillan Reference USA; 2004.
American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Part 2: Ethical Issues. Circulation. 2005;112:IV-6–IV-11.
Kass-Bartelmes BL, Hughes R. Advance Care Planning: Preferences for Care at the End of Life. Agency for Healthcare Research and Quality Research in Action. 2003(12).
The SUPPORT Principal Investigators. A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatments (SUPPORT). JAMA. 1995;274(20):1591-98.
Tulsky JA, Chesney MA, Lo B. How do medical residents discuss resuscitation with patients? J Gen Intern Med. 1995;10(8):436–42.
National Consensus Conference on Medical Education for Care Near the End of Life. Executive summary. J Palliat Med. 2000;3:88-92.
Deep KS, Griffith CH, Wilson JF. Communication and decision making about life-sustaining treatment: examining the experiences of resident physicians and seriously-ill hospitalized patients. J Gen Intern Med. 2008;23(11):1877–82.
Auerbach AD, Pantilat SZ. End-of-life care in a voluntary hospitalist model: effects on communication, processes of care, and patient symptoms. Am J Med. 2004;116(10):669–75.
Wachter RM, Goldman L. The emerging role of "hospitalists" in the American health care system. N Engl J Med. 1996;335(7):514–7.
Wachter RM, Goldman L. The hospitalist movement 5 years later. Jama. 2002;287(4):487–94.
Higginson IJ, Finlay I, Goodwin DM, et al. Do hospital-based palliative teams improve care for patients or families at the end of life? J Pain Symptom Manage. 2002;23(2):96–106.
Morrison RS, Penrod JD, Cassel JB, et al. Cost savings associated with US hospital palliative care consultation programs. Arch Intern Med. 2008;168(16):1783–90.
Auerbach AD, Katz R, Pantilat SZ, et al. Factors associated with discussion of care plans and code status at the time of hospital admission: results from the Multicenter Hospitalist Study. J Hosp Med. 2008;3(6):437–45.
Heyland DK, Frank C, Groll D, et al. Understanding cardiopulmonary resuscitation decision making: perspectives of seriously ill hospitalized patients and family members. Chest. 2006;130(2):419–28.
Mirza A, Kad R, Ellison NM. Cardiopulmonary resuscitation is not addressed in the admitting medical records for the majority of patients who undergo CPR in the hospital. Am J Hosp Palliat Care. 2005;22(1):20–5.
Anderson WG, Winters K, Arnold RM, Puntillo KA, White DB, Auerbach AD. Studying physician-patient communication in the acute care setting: The Hospitalist Rapport Study. Pat Educ Counsel. in press.
Corbin J, Strauss A. Basics of Qualitative Research: Grounded Theory, Procedures and Techniques. Thousand Oaks, CA: Sage; 1990.
Crabtree BF, Miller W. Doing Qualitative Research. Newbury Park, Calif: Sage Publications; 1992.
Tulsky JA, Fischer GS, Rose MR, Arnold RM. Opening the black box: how do physicians communicate about advance directives? Ann Intern Med. 1998;129(6):441–9.
Prigerson HG. Socialization to dying: social determinants of death acknowledgement and treatment among terminally ill geriatric patients. J Health Soc Behav. 1992;33(4):378–95.
Koropchak CM, Pollak KI, Arnold RM, et al. Studying communication in oncologist-patient encounters: the SCOPE Trial. Palliat Med. 2006;20(8):813–9.
Zeger SL, Liang KY. Longitudinal data analysis for discrete and continuous outcomes. Biometrics. 1986;42(1):121–30.
Vittinghoff E, McCulloch CE. Relaxing the rule of ten events per variable in logistic and Cox regression. Am J Epidemiol. 2007;165(6):710–8.
von Gunten CF. Discussing do-not-resuscitate status. J Clin Oncol. 2003;21(9 Suppl):20s–5.
Balaban RB. A physician’s guide to talking about end-of-life care. J Gen Intern Med. 2000;15(3):195–200.
Pentz RD, Lenzi R, Holmes F, Khan MM, Verschraegen C. Discussion of the do-not-resuscitate order: a pilot study of perceptions of patients with refractory cancer. Support Care Cancer. 2002;10(8):573–8.
Roter DL, Larson S, Fischer GS, Arnold RM, Tulsky JA. Experts practice what they preach: A descriptive study of best and normative practices in end-of-life discussions. Arch Intern Med. 2000;160(22):3477–85.
Cohen J. A coefficient of agreement for nominal scales. Educ Psychol Meas. 1960;20:37–46.
Landis R, Koch G. An application of hierarchical kappa-type statistics in the assessment of majority agreement among multiple observers. Biometrics. 1977;33:363–74.
Loertscher L, Reed DA, Bannon MP, Mueller PS. Cardiopulmonary resuscitation and do-not-resuscitate orders: a guide for clinicians. Am J Med. 2010;123(1):4–9.
Smith AK, Ries AP, Zhang B, Tulsky JA, Prigerson HG, Block SD. Resident approaches to advance care planning on the day of hospital admission. Arch Intern Med. 2006;166(15):1597–602.
Patient Self Determination Act—1990: Federal Register; 2002.
Aging with Dignity: Five Wishes. http://www.agingwithdignity.org/five-wishes.php. Accessed March 2010.
Deep KS, Griffith CH, Wilson JF. Changes in internal medicine residents’ attitudes about resuscitation after cardiac arrest over a decade. J Crit Care. 2009;24(1):141–4.
Weeks JC, Cook EF, O’Day SJ, et al. Relationship between cancer patients’ predictions of prognosis and their treatment preferences. JAMA. 1998;279(21):1709–14.
Murphy DJ, Burrows D, Santilli S, et al. The influence of the probability of survival on patients’ preferences regarding cardiopulmonary resuscitation. N Engl J Med. 1994;330(8):545–9.
Diem SJ, Lantos JD, Tulsky JA. Cardiopulmonary resuscitation on television. Miracles and misinformation. N Engl J Med. 1996;334(24):1578–82.
Plauth WH 3rd, Pantilat SZ, Wachter RM, Fenton CL. Hospitalists’ perceptions of their residency training needs: results of a national survey. Am J Med. 2001;111(3):247–54.
Tulsky JA, Chesney MA, Lo B. See one, do one, teach one? House staff experience discussing do-not-resuscitate orders. Arch Intern Med. 1996;156(12):1285–9.
Lorenz K, Lynn J, Shekelle PG, et al. End-of-Life Care and Outcomes 2004.
Curtis JR, Patrick DL, Caldwell ES, Collier AC. Why don’t patients and physicians talk about end-of-life care? Barriers to communication for patients with acquired immunodeficiency syndrome and their primary care clinicians. Arch Intern Med. 2000;160(11):1690–6.
Christakis NA. Death Foretold: Prophesy and Prognosis in Medical Care. Chicago: University of Chicago Press; 2000.
Back AL, Arnold RM, Baile WF, et al. Efficacy of communication skills training for giving bad news and discussing transitions to palliative care. Arch Intern Med. 2007;167(5):453–60.
Kurtz S, Silverman J, Draper J. Teaching and Learning Communication Skills in Medicine. 2nd ed. Oxford: Radcliffe Medical Press; 2005.
Davis DA, Thomson MA, Oxman AD, Haynes RB. Changing physician performance. A systematic review of the effect of continuing medical education strategies. Jama. 1995;274(9):700–5.
Ebell MH, Becker LA, Barry HC, Hagen M. Survival after in-hospital cardiopulmonary resuscitation. A meta-analysis. J Gen Intern Med. 1998;13(12):805–16.
Ehlenbach WJ, Barnato AE, Curtis JR, et al. Epidemiologic study of in-hospital cardiopulmonary resuscitation in the elderly. N Engl J Med. 2009;361(1):22–31.
Acknowledgements
We would like to thank the patients and physicians who generously donated their time to participate; Eric Vittinghoff, PhD, MPH, UCSF Department of Epidemiology and Biostatistics, for guidance in selection and execution of statistical analyses; and Amy J. Markowitz, JD, Consulting Editor/Scientific Writing Specialist, UCSF Clinical and Translational Research Career Development Program for editing the manuscript. Dr. Anderson was funded by the National Palliative Care Research Center and the University of California San Francisco Clinical and Translational Science Institute Career Development Program, which is supported by NIH grant number 5 KL2 RR024130-04. These findings were presented on March 6, 2010 at the 2010 Association for Clinical Research Training and the Society for Clinical and Translational Science Society Joint Annual Meeting.
Conflicts of Interest
None disclosed.
Disclosures
Dr. Anderson was funded by the National Palliative Care Research Center and the University of California San Francisco Clinical and Translational Science Institute Career Development Program, which is supported by NIH grant number 5 KL2 RR024130-04. These findings were presented on March 6, 2010 at the 2010 Association for Clinical Research Training and the Society for Clinical and Translational Science Society Joint Annual Meeting.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Anderson, W.G., Chase, R., Pantilat, S.Z. et al. Code Status Discussions Between Attending Hospitalist Physicians and Medical Patients at Hospital Admission. J GEN INTERN MED 26, 359–366 (2011). https://doi.org/10.1007/s11606-010-1568-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-010-1568-6