
Abstract
BACKGROUND
Current diabetes management guidelines offer blueprints for providers, yet type 2 diabetes control is often poor in disadvantaged populations. The group visit is a new treatment modality originating in managed care for efficient service delivery to patients with chronic health problems. Group visits offer promise for delivering care to diabetic patients, as visits are lengthier and can be more frequent, more organized, and more educational.
OBJECTIVE
To evaluate the effect of group visits on clinical outcomes, concordance with 10 American Diabetes Association (ADA) guidelines [American Diabetes Association, Diabetes Care, 28:S4–36, 2004] and 3 United States Preventive Services Task Force (USPSTF) cancer screens [U.S. Preventive Services Task Force, http://www.ahrq.gov/clinic/uspstf/resource.htm, 2003].
RESEARCH DESIGN AND METHODS
A 12-month randomized controlled trial of 186 diabetic patients comparing care in group visits with care in the traditional patient–physician dyad. Clinical outcomes (HbA1c, blood pressure [BP], lipid profiles) were assessed at 6 and 12 months and quality of care measures (adherence to 10 ADA guidelines and 3 USPSTF cancer screens) at 12 months.
RESULTS
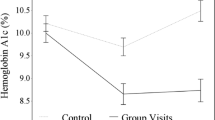
At both measurement points, HbA1c, BP, and lipid levels did not differ significantly for patients attending group visits versus those in usual care. At 12 months, however, patients receiving care in group visits exhibited greater concordance with ADA process-of-care indicators (p < .0001) and higher screening rates for cancers of the breast (80 vs. 68%, p = .006) and cervix (80 vs 68%, p = .019).
CONCLUSIONS
Group visits can improve the quality of care for diabetic patients, but modifications to the content and style of group visits may be necessary to achieve improved clinical outcomes.

Similar content being viewed by others


References
Centers for Disease Control and Prevention. National diabetes fact sheet, United States, 2003. Atlanta, GA, U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2003.
American Diabetes Association. Economic costs of diabetes in the U.S. in 2002. Diabetes Care. 2003;26:917–32.
Hofer TP, Zemencuk JK, Haywar RA. When there is too much to do: how practicing physicians prioritize among recommended interventions. J Gen Intern Med. 2004;19:646–53.
Beck A, Scott J, Williams C, et al. Cooperative health care clinics: a group approach to individual care. JAGS. 1997;45:543–9.
Clancy DE, Cope DW, Magruder KM, Huang P, Wolfman T. Evaluating concordance to American diabetes association standards of care for type 2 diabetes through group visits in an uninsured or inadequately insured patient population. Diabetes Care. 2003;26:2032–6.
Trento M, Passera P, Borga E, et al. A 5-year randomized controlled study of learning, problem solving, and quality of life modifications in people with type 2 diabetes managed in group care. Diabetes Care. 2004;27:670–5.
Sadur CN, Moline N, Costa M, et al. Diabetes management in a health maintenance organization. Diabetes Care. 1991;12:2011–7.
Wagner EH, Grothaus LC, Sandhu N, et al. Chronic care clinics for diabetes in primary care: a system-wide randomized trial. Diabetes Care. 2001;24(4):695–700.
Chobanian AV, Bakris GL, Black HR, et al. and the National High Blood Pressure Education Program Coordinating Committee. Seventh report of the joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. 2003;42:1206–52.
American Diabetes Association. Standards of medical care for patients with diabetes mellitus (position statement). Diabetes Care. 2004;28:S4–36.
Mayberry RM, Davis T, Alema-Mensah E, Samadi AR, Finley R, Jones A. Determinants of glycemic status monitoring in Black and White Medicaid beneficiaries with diabetes mellitus. J Health Care Poor Underserved. 2005;16(4 Suppl A):31–49.
U.S. preventive services task force. Preventive Services Resource Links. Agency for healthcare research and quality, Rockville, MD. September 2003.Available from http://www.ahrq.gov/clinic/uspstf/resource.htm. Accessed 15 June, 2005.
Davis TC, Long SW, Jackson RH. Rapid estimate of adult health literacy in medicine: a shortened screening instrument. Fam Med. 1993;25:391–395.
May DS, Kiefev CI, Funkhouser E, Fouad MN. Compliance with mammography guidelines: physician recommendation and patient adherence. Prev Med. 1999;28(4):386–94.
Acknowledgement of Financial and/or Other Support
This project was supported by grant number 5 P01 HS10871 from the Agency for Healthcare Research and Quality, a grant from The Robert Wood Johnson Foundation, Princeton, New Jersey, and 1R21NS043569 from National Institutes of Health/NINDS.
Conflict of Interest
Dr. Magruder, and Mr. Yeager reported receiving a $7,500 grant from Pfizer.
Drs. Clancy, Magruder and Mr. Yeager received a $107,445 grant from Eli Lilly in 2005–2006. Dr. Magruder was the principal investigator.
The other authors reported no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Clancy, D.E., Huang, P., Okonofua, E. et al. Group Visits: Promoting Adherence to Diabetes Guidelines. J GEN INTERN MED 22, 620–624 (2007). https://doi.org/10.1007/s11606-007-0150-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-007-0150-3