Article Text

Abstract
Objectives To safely expand and adapt the normal workings of a large critical care unit in response to the COVID-19 pandemic.
Methods In April 2020, UK health systems were challenged to expand critical care capacity rapidly during the first wave of the COVID-19 pandemic so that they could accommodate patients with respiratory and multiple organ failure. Here, we describe the preparation and adaptive responses of a large critical care unit to the oncoming burden of disease. Our changes were similar to the revolution in manufacturing brought about by ‘Long Shops’ of 1853 when Richard Garrett and Sons of Leiston started mass manufacture of traction engines. This innovation broke the whole process into smaller parts and increased productivity. When applied to COVID-19 preparations, an assembly line approach had the advantage that our ICU became easily scalable to manage an influx of additional staff as well as the increase in admissions. Healthcare professionals could be replaced in case of absence and training focused on a smaller number of tasks.
Results Compared with the equivalent period in 2019, the ICU provided 30.9% more patient days (2599 to 3402), 1845 of which were ventilated days (compared with 694 in 2019, 165.8% increase) while time from first referral to ICU admission reduced from 193.8±123.8 min (±SD) to 110.7±76.75 min (±SD). Throughout, ICU maintained adequate capacity and also accepted patients from neighbouring hospitals. This was done by managing an additional 205 doctors (70% increase), 168 nurses who had previously worked in ICU and another 261 nurses deployed from other parts of the hospital (82% increase).
Our large tertiary hospital ensured a dedicated non-COVID ICU was staffed and equipped to take regional emergency referrals so that those patients requiring specialist surgery and treatment were treated throughout the COVID-19 pandemic.
Conclusions We report how the challenge of managing a huge influx of patients and redeployed staff was met by deconstructing ICU care into its constituent parts. Although reported from the largest colocated ICU in the UK, we believe that this offers solutions to ICUs of all sizes and may provide a generalisable model for critical care pandemic surge planning.
- critical care
- crisis management
- hospital medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The UK confirmed its first cases of COVID-19 on the 31 January 2020. Experience from Italy provided an early warning for the UK to prepare for a substantial surge in critically ill patients if the health service were not to be overwhelmed. Reports from China and Italy suggested that 9%–26% of COVID-19 patients admitted to hospital required treatment in the intensive care units (ICU)1–3 with a median length of stay of 9 days.3 4 Modelling these data indicated that we would need to expand our capacity from 67 to more than 450 beds. Action was taken in accordance with national guidance5 to reduce and then discontinue all elective surgery from 17 March. The subsequent exponential increase in the number of patients requiring organ support in the UK has been well reported.6
We were aware of a number of recommendations for management of a surge in critical care demand7–9 but could find no information on how to operationalise the plan within such a large ICU. We therefore established a multidisciplinary working group and adopted an ‘Assembly Line’ approach focused on standardisation, simplification, upskilling and teamworking.
Organisation of critical care services before the pandemic
The Queen Elizabeth Hospital Birmingham (QEHB) was one of the largest single site hospitals in the NHS with 1200 beds and one of four acute hospitals in the University Hospitals Birmingham NHS Trust (UHB). In normal times, it was a major trauma and emergency centre serving the Midlands, as well as providing a national referral service for liver, renal, lung and cardiac transplants, a regional service for neurosciences and burns, and accommodating the Royal Centre for Defence Medicine. The ICU supporting these services had 100 bed spaces (24 as single isolation rooms) in four contiguous zones on one floor, normally funded to provide 67 level three equivalent beds. These were managed flexibly between level 1+, 2, 3 and 4 so that on average, 80 beds were used to treat patients at any one time. There were 43 specialist intensivists and 520 whole time equivalent nursing staff (of which 376 were permanent staff) providing care according to national standards (Guidelines for the Provision of Intensive Care Services, V.2).10 Each day, the ICU was staffed by 8 consultants (specialists), 7 registrars (senior residents) and 12 trainees (interns) who worked a mixture of 12 hours (long days) and 9 hours (short days) shifts. Consultants covering the ICU at night normally operated an on-call system from home. Nurse:patient ratios were 2:1 for level 4, 1:1 for level 3 care, 1:2 for level 2. Nurses worked 12.5 hour shifts. Physiotherapy provided care at a ratio of 1:7 Monday to Friday with a prioritised service at weekends.
In 2019, the ICU cared for 4217 patients and provided over 29 153 patient days of intensive care of which 67% was for elective and 33% for emergency admissions.
Methods
Our challenge was to expand critical care beds by up to 500% while maintaining patient and staff safety, delivering quality care and contending with a potential reduction in the core workforce from sickness/shielding, carer responsibilities and isolation following COVID-19 exposure. By breaking down each element of an ICU admission into its component parts, we planned to be resilient to these challenges. Staffing resources were increased in the ICU by releasing personnel from their duties elsewhere in the hospital and from regional non-emergency hospitals. Although many of the seconded staff were allocated from theatres that had been mothballed during the first wave surge, staff volunteered from all parts of the hospital (e.g. consultant hepatologists, audiology technicians, out-patient nurses). The ‘Assembly Line’ approach allowed us to allocate a sudden surge of staff to teams that best used their skills and allowed packaged training to be targeted.
Planned pathway for ICU admission and management
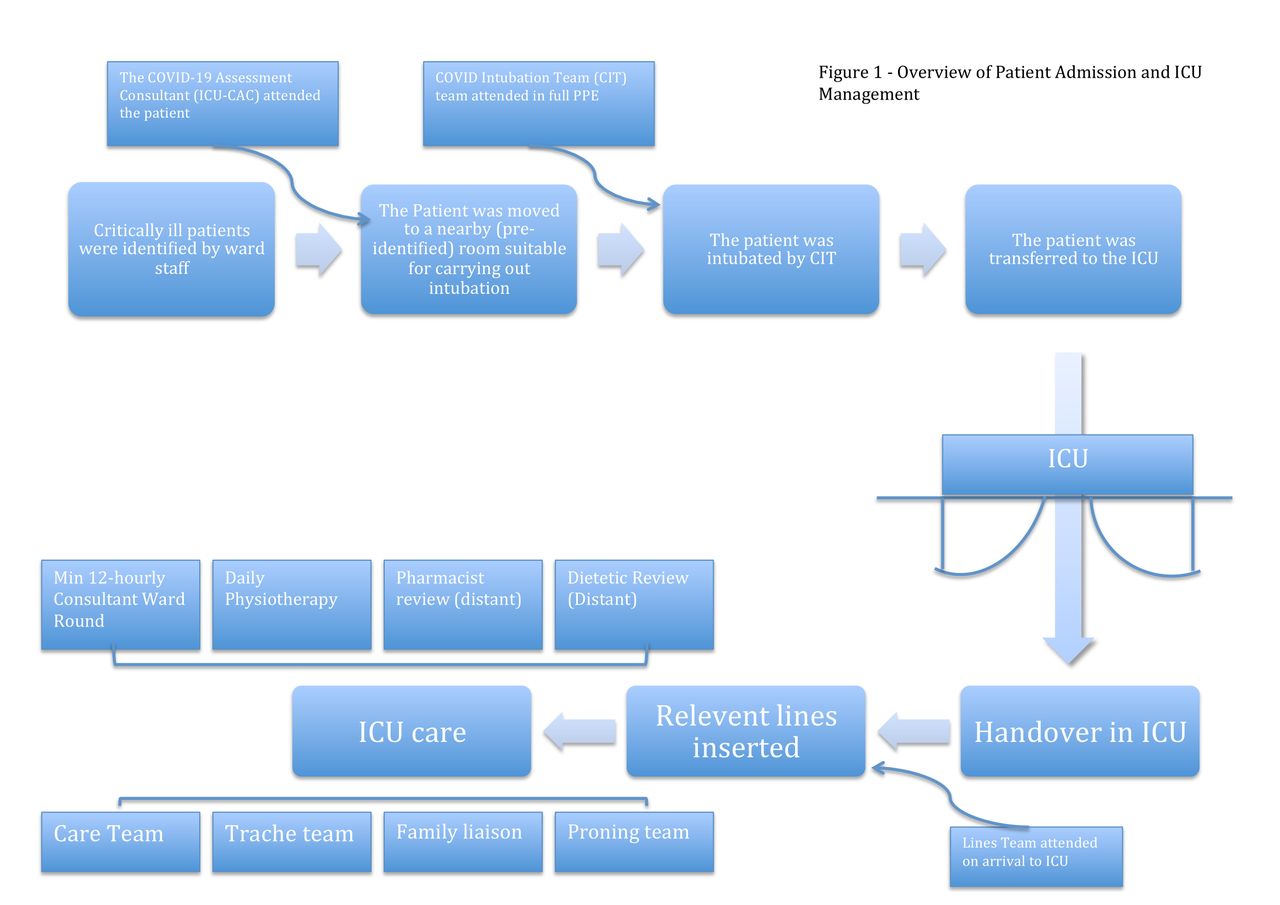
The patient journey through ICU was streamlined as follows (figure 1):
Critically ill patients were identified by ward staff.
The COVID-19 Assessment Consultant attended the patient on the ward or in the emergency department (ED) and decided on the need and appropriateness for ICU admission.
In cases where the advantage of ICU admission was deemed marginal, the patient was discussed with another ICU consultant or our Institution’s Ethics Board.
The patients were supported by Bag/Valve/Mask for the short transfer to a nearby intubation room.
As intubation is a high risk, aerosol generating procedure (AGP), we preidentified a number of areas that were used for intubation with suitable airflow, space around the bed and privacy from general view. Rooms were identified on each ward and ED.
In the absence of evidence to the contrary at the time, the senior ICU staff agreed to suspend normal management of patients and did not use non-invasive ventilatory support during the first COVID-19 wave. This was for three reasons: (1) non-invasive ventilatory support is an AGP and transporting patients to the ICU would risk contamination of the corridors (2) Non-Invasive Ventilation (NIV) uses higher oxygen flows and were concerned about the additional stress to our infrastructure and oxygen supply (3) the nursing intensity of an NIV patient is paradoxically higher and would have additionally stressed the inexperienced staff.
Redeployed consultant (attending) anaesthetists along with Operating Department Assistants formed the COVID-19 Intubation Team (CIT) who were mobilised in full personal protective equipment (PPE) from their base in theatres, to intubate and ventilate the patient.
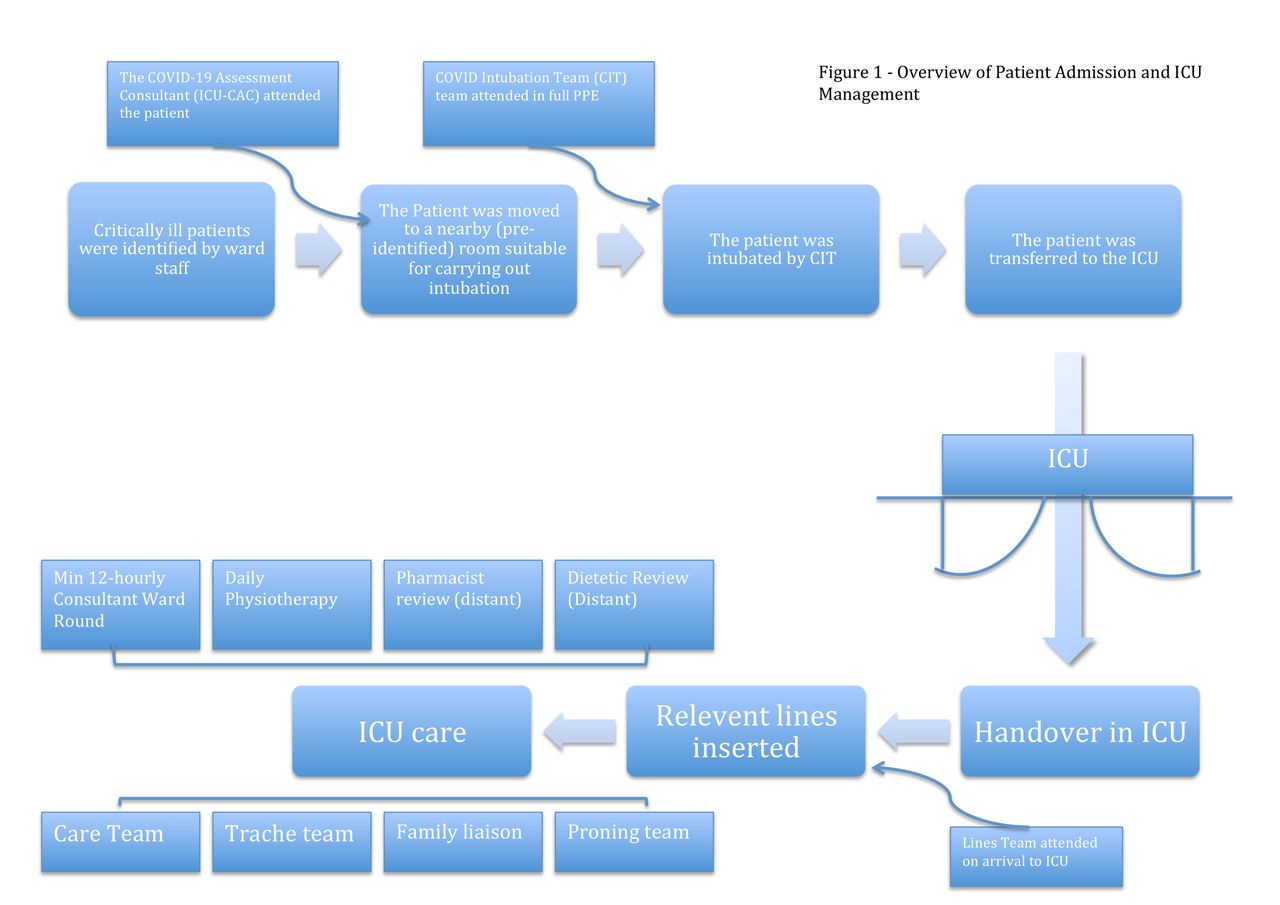
Overview of patient admission and ICU management. CIT, COVID-19 Intubation Team; ICU, intensive care unit.
Protocolised management in ICU
Safe delivery to the ICU was achieved and met by a senior member of the ICU medical team who took handover from the CIT leader
The Lines Team had already been alerted and was waiting for the admission in ICU before the patient arrived. On arrival of the patient, vascular access as decided by the admitting doctor (arterial cannulae, central venous pressure and renal replacement cannulae if required) was placed.
If proning or deproning were required, the proning team was contacted.
A team of fourth year medical students were recruited to act as the Family Liaison Service to contact relatives daily and impart the information. Additional information was provided by the clinical staff when required or when withdrawal of supportive care was being considered.
The clinical staff completed an update on the patient’s condition twice daily from a standard operating procedure template designed by the COVID-19 task force.
If the patient needed a tracheostomy, the Trachy Team were contacted and a time arranged for the procedure to be performed. Percutaneous tracheostomy was preferred as it reduced aerosol production. If the Trachy Team were to consider that a surgical tracheostomy was needed then theatre time was booked in a dedicated COVID-19 theatre.
Prior to the procedure the ICU medical team contacted the family to discuss the decision and answered any questions.
Patients received daily respiratory physiotherapy which commenced within 24 hours of admission. Rehabilitation was started as early as possible in the patient’s recovery in ICU and continued on the wards.
On discharge from the ICU, the patient was moved to COVID-19 wards where they were cared for by a team familiar with their needs. COVID-19 patients are a complex group with delirium, severe deconditioning, poor mobility and breathlessness,13 therefore, in order to keep the Assembly Line moving safely and to try to prevent readmission, an ICU consultant followed the discharged patients and a formal consultant to consultant handover was undertaken.
Implemented changes
ICU consultants proposed themselves for roles in the reorganisation according to their training, experience and strengths. The structure revolved around teamwork so that responsibility for an area did not fall on an individual, cover could be maintained in the event of absence and consensus could be made. Important decisions (such as the decision not to use non-invasive ventilatory support and to intubate patients directly) were discussed and consensus obtained throughout the whole consultant body with face-to-face meetings, WhatsApp and email discussions.
Infrastructure
Within each ICU, normal bed-spaces contained two pendants that each carried oxygen (4 kPa Pressure; 2 outlets) air (400 kPa supply; 2 outlets), suction (up to −80 kPa; 2 outlets), Anaesthetic Gas Scavenging System and 8 electrical sockets (240 V). The decision was made to place two beds in each bed-space so that staff were concentrated in one area. One trained ICU nurse supervised up to six non-ICU nursing staff. Concentrating patients in the same ICU footprint avoided diluting skills and knowledge rather than moving into theatres and other non-ICU venues.
Command
A dedicated task force of four ICU consultants trained in major incidents and mass causalities formed a line of command modelled on the gold/silver/bronze structure for coping with major incidents and mass casualties for all acute sites of our institution. Gold managed the interactions between all service operators nationally and regionally; silver managed the status of ICU within the whole of UHB; bronze managed local site-based resources at QEHB. Operational updates and risks were escalated from bronze to silver daily. Meetings were held at the start and end of each shift to communicate changes in standard operating procedures, distribution of staff across the clinical areas and manage any points of pressure within the service. Daily shift safety huddles were undertaken with other ICU staff to update them on policy changes, stages of preparation, hospital status and future planning.
Workforce
A total of 205 additional medical staff were sourced, primarily from the anaesthesia (47 of all grades) and also 158 from medical and surgical specialities whose elective work had been curtailed, to work directly in the ICU. Another 111 anaesthetist of all grades supported the ICU though visiting teams outlined in figure 1. In order to support ICU naïve medical staff, a training programme was created and undertaken by the nursing professional development and the combined deployed consultant team which was a mixture of intensivists and anaesthetists. A programme of online video lectures and resources were developed by the consultant body providing learning on topics such as COVID-19 management, sedation and the basics of ventilator settings. Each individual had an induction to the unit and the opportunity to get hands on experience of some of the equipment they were unfamiliar with prior to their first ICU shift. As roles were simplified, those staff allocated to ‘end-of-bed’ care were taught about monitoring, recording data and raising concerns about physiological derangement. Staff trained to administer drugs were trained in checking and delivering infusions. The visiting teams outlined in figure 1 were each trained in their roles. For example, the proning teams were trained in turning patients who were fully monitored and in relief of pressure points. The ICU had ventilation protocols already in place for usual non-COVID care; these were supported by our electronic systems so that if new staff recorded ventilated tidal volumes that were outside the protocol, the protocol could instruct them in what actions they should take.

Organisation of medical staff within ICU. ICU, intensive care unit.
A new staffing structure (figure 2) was put in place to mix the expertise of ICU doctors and non-ICU doctors. The day-to-day jobs, such a central line insertion, trips to the CT scanner, admitting patients, ordering radiographic investigations and blood tests and making referrals, were divided according to the skill-mix of the medical staff.
COVID-19 units were led by a sector commander, who was an experienced ICU consultant with overall responsibility for their designated COVID-19 area comprising up to 40 patients. Each COVID-19 unit was then split so that teams guided therapy for between 15 and 20 patients each, with an area lead overseeing each Area. The area leads were anaesthetists who did not necessarily have recent ICU experience but are able to manage acute physiological changes and the airway. Each area also has a junior area lead, an ICU registrar, who fielded problems from more junior staff and escalated to the area lead or sector commander as appropriate.
Each COVID-19 area was further divided into Pods of 4–6 patients; Pod doctors provided care for these patients. Pod doctors were from a variety of background ranging from ICU or anaesthetic junior trainees through to medical or surgical consultants. Pod doctors performed the initial daily morning and evening reviews to identify any ongoing issues or potential procedures which were escalated and validated to the area lead and sector commander. Each patient was reviewed by an ICU consultant at least every 12 hours and usually more frequently, maintaining usual standards of senior oversight. Protocolisation of care reduced the burden of scrutiny for consultants responsible for the patients.
All ICU rotas were harmonised and organised such that staff are always working with the same team and provided a mix of ICU/anaesthetic staff and non-ICU doctors. This allowed teams to recognise the differing skills of their members and to allocate tasks appropriately. It also allowed limited training (eg, central venous catheterisation) to continue. Shifts were changed to full 12.5 hours resident shifts.
Nursing staff also had a hierarchical structure in order to cope with an influx of 429 nurses, 168 of whom had previously worked on ICU but another 261 were ICU naïve. 1:1 nursing was provided to all patients who were sedated and ventilated but the bedside nurse was not always an ICU-trained nurse. An ICU-trained nurse oversaw up to six beds (depending on the skill mix of the bedside nurse and geography of the ICU) with a senior nurse (band 7) overseeing up to 35 patients.
The groups of nursing staff that were reallocated to support critical care services came from diverse clinical backgrounds: Research and Development, Acute Medical Unit, Theatres/Recovery, Biomedical Sciences, Preoperative Assessment, Coronary Care, Cardiology, Trainee ACCP, Clinical Nurse Specialist, Emergency Nurse Practitioners, Ward Nurses, Night Practitioners, Professional Development Nurses, Orthodontic Nurses and Day Case. The ICU also used their core skills to provide care but they were also given basic core training that enabled the safe management of invasive monitoring, basic ventilation principles and equipment training.
Theatre nursing staff were redeployed and allocated to visiting teams (such as the Care Team, Lines Team, Proning Team and Tracheostomy Team) who provided the Assembly Line care. They brought their understanding of sterile and surgical techniques while in PPE.
The physiotherapy team was supported by staff redeployed from other clinical areas to provide cover from 8:00 to 20:00 hours, 7 days per week. This was provided at a ratio of 1:12 with at least four senior physiotherapists on shift each day. The physiotherapy team provided respiratory physiotherapy, including supporting the ongoing management of lung protective ventilation and rehabilitation where possible.
Policies and procedures
A small COVID-19 critical care multidisciplinary tactical group with prior experience in high consequence infectious diseases led the rapid production of flexible policies and procedures. These included the donning and doffing of PPE, simulation, resuscitation, intubation, self-isolation and shift patterns. Policies were drawn up to consider safety of staff and to be able to stay within the confines of supply. Standard operating procedure templates allowed those staff members not familiar with ICU to perform tasks safely and to standards outlined by the ICU staff. Wards rounds were administered with the assistance of a template. Research active clinicians reviewed the latest, rapidly changing national and international evolution of evidence to feed back to the team in critical care and any alterations to the policies/Standard Operating Procedures filtered down through various communication methods.
Communication
Communication with families was mainly undertaken by the Patient Liaison Team (see below).
Communication with colleagues both on and off ICU proved challenging with traditional use of bleeps and mobile phones problematic while wearing PPE. A new communication system was procured allowing hands-free Wi-Fi communication. The system was designed so staff could speak directly to another carrier of the device either by name or role. To communicate with visiting teams (Intubation, Lines, Proning, Tracheostomy), a single route of referral via one communication centre (one unused operating theatre) was established. A ‘red phone’ equipped with a louder ring was used in each ICU area as a back-up direct line of contact from ICU commander to the unit and vice versa.
Bedside key resource folders with laminated cleanable pages were created and information posters were displayed in the units. We used traditional email to distribute daily updates to the multidisciplinary team which also provided a portal for feedback. Social media (none of which carried patient information) was used with multiple WhatsApp groups (for immediate short-term decisions), Twitter (to engage with the wider community about current practise and boost morale) and Facebook (also to boost morale).
Service delivery
Care pathways were disaggregated into task sequences; discrete processes of care requiring specific skills sets. Care processes which could be delivered by non-intensive care staff redeployed to intensive care were identified. The teams were autonomous and able to deliver care as they saw fit. Processes were refined within each team without external influence. This allowed them flexibility about skill mix and staffing according to availability. These discrete teams were separate resources with no cross-over of staff to reduce the risk of externally acquired COVID-19 from spreading between teams. Cross-cover for sickness, self-isolation and caring for household members was managed within teams reducing stress on higher managers. Examples are given below:
Intubation team
A team of senior anaesthetists and operating department assistants was formed to perform all endotracheal intubations in full PPE outside ICU in ward and ED patients with respiratory failure from COVID-19 infection. This allowed safe stabilisation of the patients and staff protection.
Proning team
Intensive proning simulation training was delegated to our anaesthetic and critical care physician-assistants (ACCP) who cascaded their training to neurosurgical consultants and other deployed theatre staff. The team consisted an airway trained practitioner (ACCP or anaesthetist) and four theatre non-scrub staff who moved between ICUs in full PPE.
Lines team
Senior anaesthetists experienced in central venous catheter insertion were allocated to spend their shift inserting lines of all types for new admissions and changing lines as directed by the ICU team. They were accompanied with a scrub team and carried limited equipment with them to reduce cross-contamination.
Care team
Theatre teams were formed to assist with washing and routine care to relieve pressure on the ICU nursing staff.
Percutaneous tracheostomy team
Ear, Nose and Throat and maxillofacial surgeons were seconded to the ICU and were accompanied by dedicated, experienced anaesthetist. The ICU protocolised the process for insertion of a percutaneous tracheostomy which was agreed by the surgeons during surge preparations. The surgeons received training on the tracheostomy insertion equipment used in the ICU. To reduce the need for cross-contamination and cleaning, a percutaneous insertion technique was used that did not use bronchoscopy. There was multidisciplinary agreement about the physiological parameters to guide selection for tracheostomy although the decision regarding the requirement for tracheostomy was made by an ICU consultant.
Patient liaison team
Medical Students in the fourth year (from five) of their university course were seconded to the ICU. They were protected from exposure to COVID-19 in the ICU by remaining outside and instead received daily updates about patients from a template completed by the nursing staff caring for the patient. Wherever possible, the same medical student rang the family at the same time of day to try to reduce anxiety in the family over delayed or unexpected calls
Renal replacement therapy team
Although the number of renal replacement therapy (RRT) was lower than the same period 12 months ago, the surge meant that more patients required RRT simultaneously. A protocol was developed to enable the sharing of machines while providing adequate clearance and fluid balance control. The protocol underwent real-time modification when it became clear that many of the patients exhibited a hypercoagulative state. Most patients where managed with 4 hours of high volume haemodiafiltration (6L ultrafiltration exchange per hour), and net negative fluid balance of 100 mL per hour during treatment. Machines were then cleaned before being used with the next patient. Most machines treated three patients during any 24 hours period. Our ICU moved to Fresenius 8005 machines with a sterile water plant with individual reverse osmosis units for each and so we had no problems with supply of RRT fluids.
Ventilation team
The physiotherapy team were tasked with supporting compliance with lung protective ventilation. This included measuring patients on admission, with height and ideal lung protective tidal volumes displayed on white boards in the patients bedspace. The physiotherapy team also completed morning and evening ward rounds where ventilator settings were reviewed and changed according to a protocol.
Research team
The importance of research in understanding COVID-19 disease was recognised by maintenance of a skeleton research staff. The research nurse team was cut to 12% of its normal personnel and 80% of reallocated staff were directed towards the ICU with the rest shielding due to existing co-morbidities. Our hospital fell into line with the national requirement for participating Urgent Public Health Research Studies (https://www.nihr.ac.uk/covid-studies/) approved by the chief medical officer and recruited to 19 of those studies.
Training and education
All formal educational assessment requirements were always suspended but informal bedside teaching continued day or night provided by senior team members to those more junior. This was met with enthusiasm, particularly from the ICU naïve members and excellent feedback given regarding teaching and support. The Critical Care Clinical Nursing Education workforce had their normal rotas adapted to facilitate 24/7 support for all redeployed nursing workforce.
Psychosocial support
It was recognised that the service reconfiguration and overwhelming nature of the COVID-19 surge brought with it a burden of physiological and emotional challenges. Personnel were working in unfamiliar environments with the constant stress of being exposed to a harmful infective agent.
Critical care nursing had already appointed a restorative practice lead nurse before the pandemic but as the workforce expanded, an additional full-time senior nurse was seconded to support delivering clinics, meeting staff, telephone and social networking forums. This allowed staff access to emotional and psychological support during the day and night. Where necessary, the Restorative practice nurses could refer staff to trust councillors and psychologists.
In addition to the social media channels mentioned above, a named wellness champion sent regular emails to all colleagues and made themselves available for conversations that were difficult to have with other colleagues or family. Well-being rest rooms were identified which provided access to a bed, hot drinks and refreshments for time out of the PPE and away from the ICU. Hot meals were delivered day and night to the COVID-19 staff rest rooms and staff were offered meal vouchers for use in the hospital canteen.
These initiatives were welcomed and staff report that they felt they had clear pathways they could use if needed and a well signposted first contact to use for a variety of needs. Close working with occupational health professionals helped to supplement and support guidance given regarding shielding or sickness. Analysis of staff feedback is underway and will be reviewed in regards to ongoing improvements that can be made to out support structure.
Results
During the 4 weeks of April 2020, a total of 154 patients were admitted to the dedicated COVID-19 ICUs. Thirteen patients were negative for COVID-19 based on nasal swabs and non-directed broncho-alveloar lavage samples. Overall mortality for the cohort was 27% (n=42). Median length of ICU stay was 19 days (range 1–50 days) and the median time to death was 9.5 days (range 1–40 days).
A sample of our time from decision to admit from the ward or ED to safe transfer to ICU was 110.7±76.75 min (±SD, N=19) compared with 193.8±123.8 min (±SD, n=15) (p=0.022). In many cases, it was unclear when the decision to admit to ICU was made and many of our patients were admitted from other hospitals and so were not included in the calculations.
We provided 3402 patient days care on ICU during April 2020, compared with 2599 for the same month in 2019 (30.9% increase) but absolute patient numbers (COVID-19 and non-COVID) decreased to 274 from 428 (35.9 decrease), a reflection of the length of stay of the average patient with COVID-19 disease. A total of 126 patients were cared for simultaneously compared with a peak of 86 patients in the previous year (46.5% increase). The number of ventilated days increased in the same period to 1845 from 694 (165.8% increase). In the equivalent period in 2019, 58 tracheostomies were inserted; this compares with 114 tracheostomies during the COVID-19 crisis in April 2020. Table 1 summarises these differences in activity. Between the 8 April and 8 May, there were 180 recorded patient interactions for the Line team with 16 Arterial lines, 98 vascaths, 89 Central Venous and 12 Peripherally Inserted Central Catheter insertions, a total of 215 lines in all. In total 60% of patients admitted with symptoms of COVID-19 pneumonia were ventilated in the prone position with many requiring five episodes of proning. At the peak, the proning teams carried out 52 proning/deproning procedures in a 12-hour shift.
Summary of increase in activity for the study period
During the same period, 98 patients commenced mobilisation within critical care, defined as sitting on the edge of the bed or higher. All 84 patients discharged from critical care during the study period had commenced mobilisation and on average were able to stand or step transfer prior to ward step down.
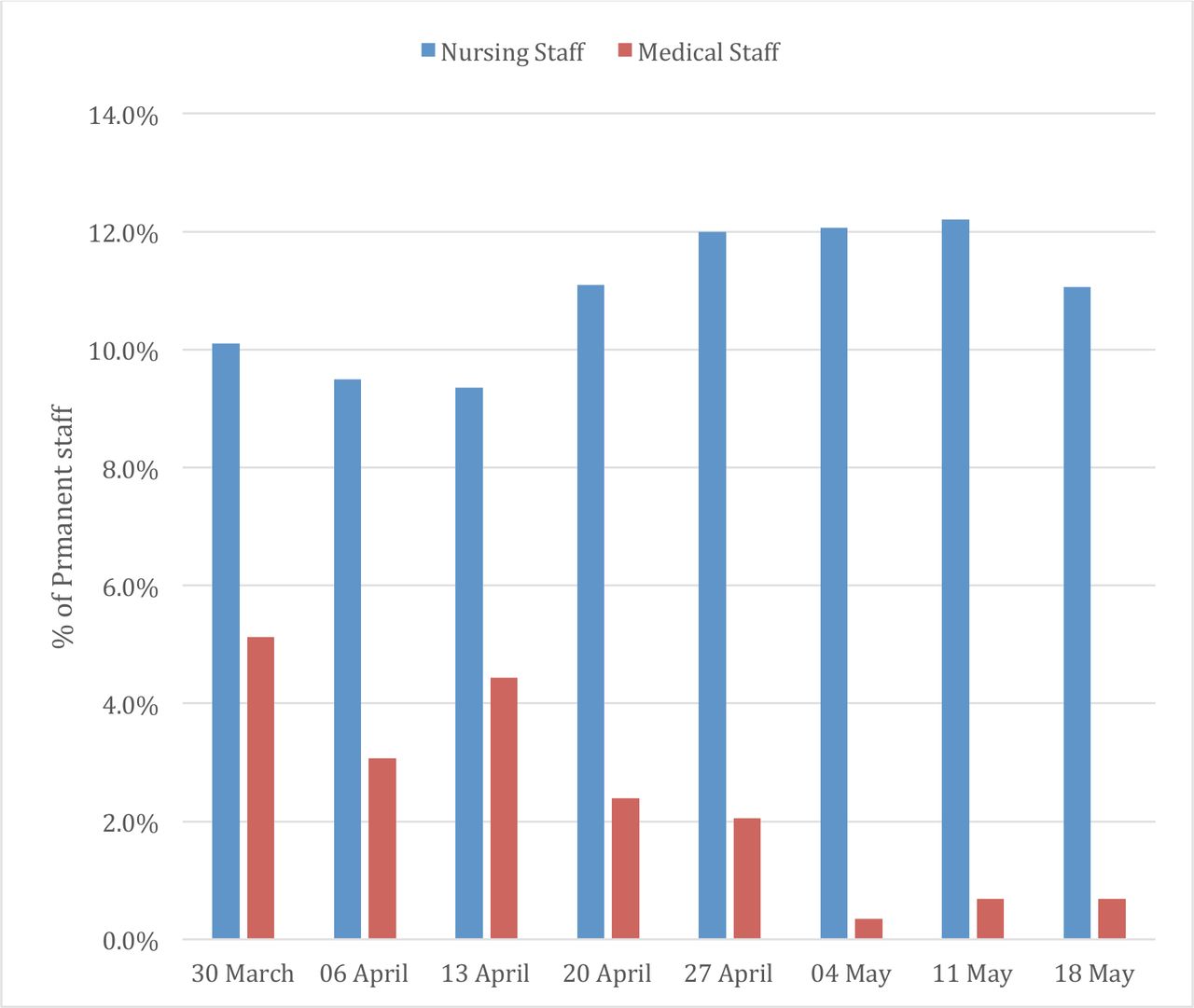
We saw relatively few staff absences. Figure 3 plots ICU staff absence because of illness (combined long term and short term). Normal nursing absenteeism was approximately 10% and this rose to 12.1% before falling again. We had a spate of medical staff who caught COVID-19 just before a period of this study and so we saw a fall in medical absenteeism back to baseline 1.3% during the surge itself, having previously been a high 5.1%.
{kind=link}
{kind=link}
{kind=link}
ICU staff sickness between 30 March 2020 and 18 April 2020. ICU, intensive care unit.
Discussion
The Long Shops were the first recorded example in the UK of assembly line manufacture. Dating back to the height of the industrial revolution, they broke down the manufacture of agricultural machinery, steam engines and trolleybuses into small manageable parts. Apprentices could be taught to become skilled at just a few tasks on the line and did not need to be proficient in the whole process. This allowed more complex machines to be made as well as shortened the time needed for workers to become proficient. We believe that we have used a similar production line model for the care of ICU patients to manage the surge in redeployed staff and COVID-19 during the first wave of a global pandemic.
Although previous work alerted us to the pressures that we expected to cope with during the first wave surge,7–9 we could find no information on how to implement preparations in a large ICU. We believe that breaking ICU care into its component parts and taking an Assembly Line approach to its delivery allowed a flexibility to cope with a surge in patient numbers while also enabling a wide-ranging teaching programme, ensuring that teams were protected from burnout, reducing cross-contamination between teams from infected patients and accommodating staff absences. In addition to unprecedented patient numbers in a short period of time, we also dealt with a surge in additional staff who needed training and a role suited to their skills, all while maintaining patient safety and a high standard of care. We increased our efficiency so that there was always an ICU bed immediately available and the time to admission of a patient to ICU was reduced even in the face of what would otherwise have been overwhelming numbers.
In terms of mortality rates, the Assembly Line approach provided a quality of care which was at least comparable to other hospitals in the UK. One criticism may be that the Assembly Line does not allow for bespoke adaptation, however, as our surge capacity was for a single disease, the need for adaptation of our protocols was minimal.
When Garrett and Sons14 introduced the Assembly Line, it was dedicated to only manufacturing one product. Similarly, our changes facilitated the treatment of one disease, COVID-19, but was not necessarily suitable for the management of the full spectrum of critical illness.
It is unclear whether an Assembly Line provides better care. Concerns were voiced that by deconstructing ICU care into discrete tasks staff would become deskilled in various procedures and may face challenges to the care process without the holistic approach normally adopted. It was felt that, as these measures were put in place to deal with a short term surge of characteristically similar cases, the workforce would quickly be able to reacquaint themselves with those skills and procedures once the need for a long shop approach had passed. A future review from our workgroup based on the feedback from staff, both redeployed and ICU based, will formally assess to what extent these measures had on staff moral, training and acceptance of our dramatically different approach to ICU care in face of the COVID-19 crisis.
We believe that strict infection prevention control and the early introduction of donning and doffing areas protected the ICU from a large increase in staff absenteeism. We also believe that staff confidence and mental well-being was enhanced by these clearly defined areas.
Conclusions
In April 2020, our ICU was faced with a surge in critically ill patients but also a surge in staff redeployed to help cope with the expected increase in patient numbers. We were fortunate in being able to reallocate large staffing numbers from elsewhere in the hospital to the ICU and use their specific skills into discrete teams. We have described a model of care that we believe may be useful for ICUs of all sizes when faced with abrupt changes in demand.
We found that significant changes to all aspects of ICU, from staff structuring to clinical delivery, greatly improved the ICU capacity and efficiency as measured by time to admission. Important lessons have been learnt about what can be achieved in a short space of time when required. A number of the initiatives implemented are clearly only viable in the short term (lines teams, proning teams, trachy teams), other measures have a more widespread use for a unit under significant workload pressure such as family liaison teams, ventilation and RRT teams.
Measures such as staff absenteeism and feedbackfrom redeployed staff were good. Rates of COVID-19 acquired from working in the ICU were low and sickness for other reasons including stress were little different from pre-COVID. Staff feedback for teaching and how supported they felt was good and the numbers of staff willing to return to ICU for any subsequent surge are high.
We believe that the system we employed for the first surge in COVID-19 patients to our institution will serve as a good starting point for other organisations.
Acknowledgments
The authors acknowledge the ICU patients and work of all ICU, seconded and support staff of University Hospitals Birmingham NHS Trust Department of Critical Care,
Footnotes
Twitter @Whitehouse_ICU
Collaborators The QEHB COVID-19 Response Team: Abby Ford, Alejandro Barrios, Andy Johnston, Anwar Shah, Bill Tunnicliffe, Julian Bion, Brian Pouchet, David Hume, David Riddington, Deborah Turfrey, Dhruv Parekh, Gregory Packer, Harjot Singh, Ian Ewington, John Kelly, Kaye England, Laura Tasker, Mansoor Bangash, Mav Manji, Mike Knowles, Mohammed Arshad, Neil Abeysinghe, Nicholas Talbot, Nilesh Parekh, Phillip El-Dalil, Randeep Mullhi, Ravi Chauhan, Ravi Hebballi, Richard Browne, Sam Denham, Sandeep Walia, Shraddha Goyal, Steffen Kroll, Sue Sinclair, Tom Clutton-Brock, Tomasz Torlinski, William Tosh, Zahid Khan
Contributors All authors contributed to the preparation, collation of data and writing of the paper. All authors approved the final paper. CO, CP, NG, TV and TW conceived the paper. CO and TW edited the paper prior to submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data that support the findings of this study are available from the corresponding author, TW, upon reasonable request.