Article Text

Abstract
Practice-based learning via clinical placement is a core part of a physiotherapy degree with the Chartered Society of Physiotherapy requiring completion of 1000 placement hours over a preregistration degree programme. In April 2020, as a result of the COVID-19 pandemic and subsequent lockdown Connect Health had to cancel 10 student placements as we transitioned to virtual consultations for all clinics. This cancellation of student placements was replicated across the nation with many Higher Education Institutes reporting a backlog of student placements. Without the requisite placement hours students are unable to progress into the next academic year or are unable to graduate. This then reduces the flow of new-graduate physiotherapists into the workforce at a time when there is a plan to grow the physiotherapy workforce to meet primary care demand. In response to this problem a novel placement model to facilitate virtual student placements (‘virtual placements’) was developed, tested and then rolled out across Connect Health using the Plan-Do-Study-Act quality improvement methodology. The model combines shadowing a broad range of virtual clinics with delivery of patient-facing online exercise classes via the Facebook Live platform and completion of virtual projects to support knowledge consolidation. This virtual student placement model enabled an increase in student capacity of over 400% compared with 2018–2019 with 182 students starting between May and August 2020. The model runs using widely available technology, requires no additional investment and has enabled these students to continue their studies and progress towards qualifying as physiotherapists.
- allied health occupations
- PDSA
- quality improvement
- telemedicine
- health professions education
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Connect Health (‘Connect’) is the largest, independent provider of integrated community Musculoskeletal (MSK) and Physiotherapy services in the UK, serving over 350 000 National Health Service (NHS) patients per year across 26 Clinical Commissioning Groups and over 100 businesses. Connect consists of over 400 clinicians on a national basis and is diverse in terms of range of professional roles. Connect Health serves a broad patient population and have specialist services to accommodate this which includes Persistent Pain, Rheumatology, Orthopaedics, Podiatry and MSK Physiotherapy.
Connect actively supports Higher Education Institutes (HEI’s) as a placement provider, accommodating an average of 100 physiotherapy undergraduate student practice placements nationally per year. Ten undergraduate students, from two HEI’s, were due to commence their MSK practice placement within Connect in April 2020. However, traditional physiotherapy student placement models are heavily reliant on face-to-face care delivery and clinical mentorship. Therefore, with the novel COVID-19 pandemic resulting in ‘lockdown’ in the UK,1 the traditional model of student placements became redundant. This generated a need to develop a new, innovative model for undergraduate student placement provision.
Background
The COVID-19 virus is transmitted primarily through respiratory droplets generated by coughing and sneezing, and through contact with contaminated surfaces.2 WHO on 11 March 2020, declared the COVID-19 outbreak a global pandemic,3 and the UK went into ‘lockdown’ on the 23 March 2020.4 National lockdown and social distancing regulations consequentially resulted in placement providers having to cancel student placements due to a shift to virtual working, redeployment of staff and the increased of students contracting COVID-19 on practice-based placements5
Practice-based learning is a global mechanism for HEI’s to provide students with experiential learning to bridge the gap between their academic present and their professional future, providing practical opportunity to apply their taught knowledge into skill acquisition. There are over 75 HEI’s in the UK who provide physiotherapy preregistration programmes.6 The provision of clinical practice placements for students are fundamental to physiotherapy education and the Chartered Society of Physiotherapy (CSP) stipulates that each student must complete a minimum of 1000 hours of practice-based learning.7 In response to the challenges faced by HEI’s to accommodate the 1000 hours of practice-based learning during COVID-19, the CSP issued guidance8 that compliments that of the Health and Care Professions Council (HCPC),9 to focus the need for flexible contingency plans to ensure students meet the physiotherapy standards of proficiency on graduation.10
Health Education England (HEE) and the HCPC have also implemented a model whereby students can opt into a paid placement as a support worker in order to support the NHS and continue their studies.5 However, these placements often take longer to set up as students need to be added to the organisational infrastructure for example, pay roll. Further, they are also not accessible to those students with underlying health conditions who are at greater risk from COVID-19-related complications or international students that may have moved abroad to be with family during the pandemic.
The CSP and HCPC have both encouraged HEI’s and placement providers to be creative and innovative in their ability to provide workplace learning for students.8 9 This encouragement highlights the potential significant impact and future workforce risk associated with lack of placement opportunities. With the recent introduction of the 5-year general practice contract framework to assist delivery of the commitments within the NHS Long Term Plan, this framework provided funding for 20 000 new primary healthcare professionals such as Physiotherapists and First Contact Practitioners through the Additional Roles Reimbursement Scheme.11 Without a new graduate workforce to backfill these posts, there will be significant shortfall within both primary care and physiotherapy service provision. This pressure to train sufficient allied health professionals has been recognised by HEE who have extended their Clinical Placement Expansion Programme to selected allied health professions, including physiotherapy.12
The social distancing regulations introduced as part of the COVID-19 response13 prevents direct patient contact to reduce the risk of COVID-19 transmission. The use of digital technology in response to these regulations in order to maintain service delivery has seen an increase in virtual consultations.14 Virtual consultations delivered via telephone or video have demonstrated a number of advantages to service delivery including a reduced need for patients to travel to their appointments, ability to provide care to those who are shielding or self-isolating, and supports clinicians to conduct clinical work from home. Connect transitioned to offering all appointments as virtual consultations in4March 2020 and then considered the potential to innovate through virtual placements following the need to postpone the 10 undergraduate students who were to commence in April 2020. A search of the published literature returned no results for virtual placements in healthcare indicating that this is a previously unexplored area.
With the national demand for student practice placements increasing, it soon became clear that a virtual student placement model could be expanded throughout Connect to support HEI’s in placement provision. The aim of this project was, therefore, to develop a novel model for virtual undergraduate clinical placements for physiotherapy students that would allow fulfilment of the postponed 10 placements and be scalable to be delivered nationally throughout Connect and across multiple HEI’s.
Measurement
The primary evaluative outcome measure for the virtual student placement project was the number of student placements that commenced from April 2020, which was when the original 10 student placements were due to start pre-COVID-19 social distancing regulations. This data will be compared with traditional face-to-face student placement numbers in 2018–2019.
Given the recognition of a national challenge to placement provision across HEIs, and the potential that a virtual placement has to be scalable, a second outcome measure of the number of HEI’s we were able to provide placements to was selected.
The 2018–2019 data were extracted from Connect placement records while the 2020 data from virtual placements was readily available to the team. These data were gathered for all Connect services which had provided placements for students since 2018. When Connect was running a traditional, face-to-face student placement model we had 45 students from four HEI’s in April–August 2018 and 35 students across five HEI’s in April–August 2019.
Design
Initially using a modification of experience-based codesign,15 it was clear from discussions between the placement team at Connect and existing partner HEI’s, that there was a pressing demand for student placements and an appetite for innovation and collaborative working to meet this demand. The virtual student placement project was started in May 2020 following discussions and input from the HEIs as to what requirements a new placement model would need to fulfil.
Following the move to virtual consultations, we continued to complete clinical supervision for clinical staff using Microsoft Teams (Microsoft Corporation, Washington, USA) within Connect and so hypothesised that we could introduce students shadowing virtual clinics as it had proved viable to have qualified clinicians shadowing each other. This software has been made freely available to NHS services.16 As part of the COVID-19 response Connect has also launched live, online exercise classes using Facebook (Facebook, California, USA) as a medium, to replace the usual class and gym-based rehabilitation that were publicly available. This presented a novel opportunity for students to plan, lead and deliver an exercise class as part of a clinical placement.
As a result of the shift to virtual clinical delivery due to COVID-19 and a desire to fulfil our commitment to taking students on placement an initial model for virtual placements was developed as outlined in figure 1.
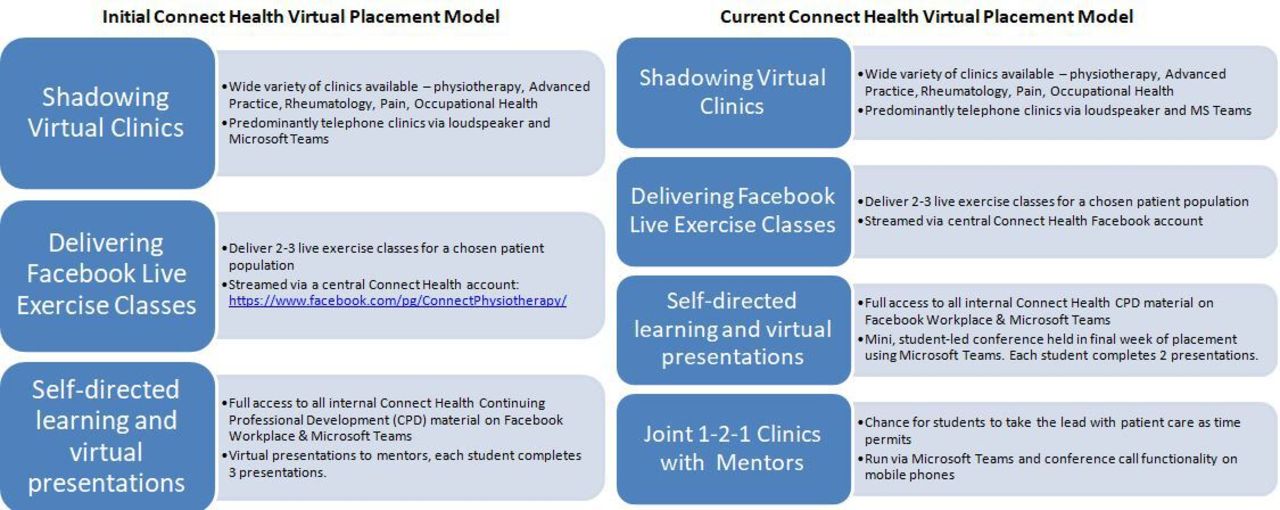
The initial virtual placement model is shown on the left, this model was implemented with the first cohort of students in may 2020. The current connect health virtual student placement model is shown on the right and demonstrates the development following PDSA cycles. PDSA, Plan-Do-Study-Act.
This initial model combined exposure to patient care via shadowing virtual clinics, opportunity to deliver public-facing exercise classes via Facebook Live and knowledge development via self-directed learning and preparation and delivery of virtual presentations. To ensure that the initial model designed would provide sufficient exposure to patients and learning opportunities to contribute toward the required placement hours required by the CSP, two separate HEIs contributed to development of the model.
To gauge initial capacity for placement provision, we gathered expressions of interest from our clinical staff in acting as a clinical mentor for a student on virtual placement, as we anticipated that the number of mentors would be the primary limiting factor to number of virtual placements that we could accommodate. From these responses we were able to provide 24 placements across two partner HEI’s starting on 18 May 2020. We planned to continue gathering support of clinicians across Connect with the aim of offering more placements throughout the summer months in order to be able to expand our offering to HEIs across England.
With the initial model finalised, the virtual placements team allocated a lead clinician to coordinate the placements and with a remit to develop the initial model as required, to be able to implement a sustainable, scalable virtual placement offering, using quality improvement (QI) methodology. The virtual placements team agreed to meet weekly via Microsoft Teams to review progress and plan the next stage of the project as well as staying in regular email contact.
Strategy
Various methodologies exist to support a QI process. The virtual placements project was a novel, untested idea and in keeping with the aims of the project, we utilised The Model for Improvement17 which is well suited to use when introducing new systems. The Model for Improvement incorporates Plan-Do-Study-Act (PDSA) cycles within a broader framework and allows experimentation, to test changes and observe the outcome prior to implementing the learning into the next cycle.
We completed three PDSA cycles between May and June 2020 which can be divided into Initiation, Implementation and Improvement. These cycles are fully detailed in table 1.
This table demonstrates the three PDSA cycles undertaken for the virtual student placements project
Results
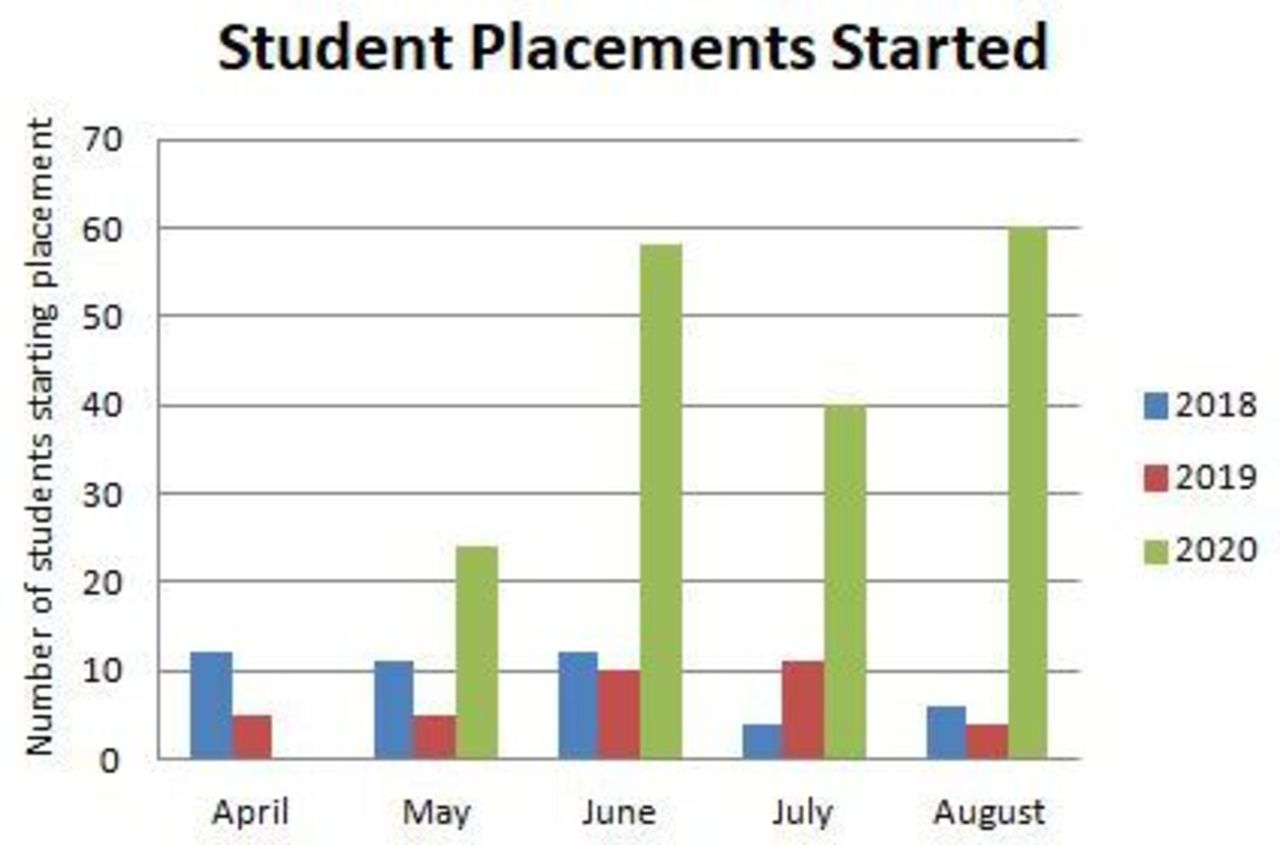
The primary outcome measure was the number of students starting on placement within Connect (figure 2) in April–August 2020. From April to August 2020, 182 virtual student placements were provided. The traditional face-to-face model over the same time period of April–August in 2018 was able to accommodate 45 placements, and in 2019, 35 placements. The virtual placement provided a placement capacity increase of 404% (2018) and 520% (2019), respectively.
{kind=link}
{kind=link}
The bar chart demonstrated the number of student placements provided between April–August for three successive years (2018–2019). The blue and red bars highlight placements provided using a face-to-face model, the green bar represents the virtual placement developed within this QI project. QI, quality improvement.
The secondary outcome measure was the number of HEIs we were able to provide placements to. In the period between April–August 2020, placements were provided to students from 8 HEIs using the virtual model. The traditional face-to-face model over the same time period of April–August in 2018 was able to accommodate students from 4 HEI’s, and in 2019, 5 HEIs.
Lessons and limitations
The initial project aim was to develop a model that allowed for the completion of the 10 postponed student placements in a virtual manner. This then evolved into the development of a sustainable nationwide, virtual student placement model. Throughout this process several key lessons emerged.
A robust virtual infrastructure is vital to running effective placements. With no face-to-face contact between any stakeholders there is a challenge to effective communication between placement coordinators, clinicians, students and HEI’s. All students were given a dedicated Connect user account to provide access to this virtual infrastructure. We used the Microsoft 365 (Microsoft, Washington, USA) platform to run the logistics of the placement with a shared placement calendar enabling students to see all the learning opportunities available. Facebook Workplace is used by Connect for internal communications and a student community group was created within the wider Connect community group to provide a space for student discussion and engagement as well as repository for resources.
To support Connect clinicians in mentoring virtual students we arranged Microsoft Teams meetings with the HEI tutors to provide a forum for question and discussion. These were all recorded and circulated to all mentors afterwards.
When introducing a new model of practice, role modelling is vital. We had two of our Consultant Physiotherapists involved with the first cohort and this commitment from the senior clinical team signalled the importance of this project. We engaged heavily with the early adopters to support them in virtual mentoring of students and encouraged them to share their success stories and lessons learnt across the clinical workforce. This helped drive the momentum of the project and ensure clinicians were engaged with mentoring and offering clinics for students to shadow virtually. This leadership ensured we had the clinical capacity to support the students on virtual placement.
The iterative nature of QI and the Model for Improvement allowed for experimentation in order to innovate and demonstrate continuous improvement. We made several changes to how the calendar was structured and organised in the first week in order to ensure the administrative workload on the virtual placement team was both manageable and sustainable. We cut one of the virtual projects in week 3 of the first cohort to better support student workload and timetable pressures. We introduced the peer mentor model at the start of week 3 when the second student cohort had started which was not something we had considered in our initial planning. Considering these improvements within the PDSA cycles helped provide structure and consistency throughout the improvement process.
Some unique strengths of this virtual placement model became apparent during implementation. Students were able to shadow a broad range of clinics including physiotherapy, advanced practice, rheumatology, consultant physiotherapist led, specialist pain and occupational health. Students reported that they enjoyed the opportunity to engage with so many different clinical settings and learn from a wide range of clinicians within one placement, which is not usually readily available. The students from the preceding cohort would provide peer-mentorship, alongside the clinical mentor. This peer mentor model provides a novel opportunity for early development of leadership and mentoring skills as well as supporting the continuation of the peer learning associated with traditional placements.
The virtual nature of the placement also enabled those students with pre-existing health conditions or living abroad to complete a clinical placement and thus continue with their studies. Ensuring that students had control over their timetable enabled them to fit the placement to their needs with several students doing flexible hours to accommodate childcare arrangements. Without a virtual placement they would have been unable to complete a practice-based placement and would have had to delay progress through their course thus adding to the future workforce pipeline problem.
While we achieved our aim of creating a virtual student placement model it is not without limitations. The primary limitation, as with all virtual working, is the reliance on technology. For some students and clinicians there is a familiarity issue with virtual platforms. This was addressed in PDSA cycle 2 through appropriate support and development of easy to follow guides to help students and clinicians navigate the new virtual landscape. The key solutions implemented to overcome this problem were:
Production of walk-through videos to assist clinicians and students in setting up and navigating the central clinic calendar in order to populate shadowing clinics.
Dedicated ‘how-to’ guide and walk-through videos for successful delivery of Facebook Live classes.
Ensuring all students had access to, and understood how to contact, the Connect IT team should they experience any technology issues.
A more difficult challenge to overcome is the accessibility issues some people may experience with technology, for example a clinician with a hearing impairment. Furthermore, while our virtual placement model offers a learning rich environment it is not possible for students to take the lead as much within consultations. Due to information governance risks associated with students working remotely we were unable to give access to clinical records systems for them to input clinical notes. To mitigate this, students were encouraged to write their own notes during consultations and share these with their mentors for discussion afterward allowing them to develop this skill.
The virtual clinic environment also means that there is no opportunity to for students to practice their ‘hands-on’ objective assessment skills, which is usually seen as a key component of clinical placements. We decided that, rather than trying to artificially include teaching on this, we would better serve students by focusing on the skills needed to run a successful virtual clinic as well as the opportunity to develop skills not previously included on clinical placements such as the delivery of virtual rehab classes.
This is a challenge that many qualified clinicians faced during COVID-19 as well as the students on clinical placement. To this end, the senior clinical leadership within Connect produced a series of webinars to help clinicians’ up-skill in virtual consultations and these were made available to all students as well. These skills are likely to form part of the future of healthcare delivery and this model provides a unique learning opportunity for exposure to such skills early in the student’s careers.
Examples of these webinars can be found at these URLs:
‘Remote Rehabilitation’ with Matthew Wyatt: https://www.youtube.com/watch?v=8O__lTQfILU&feature=youtu.be (online supplemental file 1).
Supplementary video
‘Video Consultations’ with Andrew Cuff: https://www.youtube.com/watch?v=DnI2fkFrIZg&feature=youtu.be (online supplemental file 2).
Supplementary video
Further, students were encouraged to write up case studies and plan hypothetical objective assessments based on the virtual assessments conducted. This helps to develop the clinical reasoning which underpins a good objective examination and is arguably the most important skill to start developing on placements with the mechanics of objective assessment developed later. It seems likely that aspects of virtual clinics will be carried forward into service models after the COVID-19 pandemic and thus the opportunity to develop these skills now equips students to thrive in the post-COVID-19 era of service delivery.
Due to the COVID-19 pandemic clinical diaries are quieter than normal due to the interruption of routine care, and this has allowed most students the opportunity to lead on some patient consultations. However, as diaries start to get busier as part of COVID-19 recovery, it is anticipated that this may become more difficult to manage and we may have to scale down our student numbers for the model to remain sustainable.
Conclusion
The virtual placements QI project was successful and useful as we were able to design, implement and improve, to arrive at a model for virtual placements that allowed us to achieve our aims. To our knowledge, this is the first report on the implementation of virtual placements in response to the COVID-19 pandemic. We believe this model, or a version of it, could be implemented in any setting running virtual clinics to facilitate the continuation of student placements during the COVID-19 pandemic and thus supporting the progress of students into the workforce.
The QI process was conducted rapidly, in response to an ever-changing environment, and should be considered with respect to its limitations. We continue to run an iterative QI approach to develop a blended student placement model combining the best of both traditional and virtual models as we transition back to face-to-face working. We are also looking to undertake a qualitative evaluation of the student and clinician experience of the virtual student placement model.
Acknowledgments
The authors would like to thank Thomas Flanagan for critical review and input as well as the clinical education teams at Kings College London and Brunel University for their review of the initial placement model and support of the programme.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @rorytwogood
Contributors MW and RT conceived and designed the initiative. All authors were involved in collection, analysis and interpretation of data. RT, EH and AC drafted the manuscript with critical review and final approval from all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Connect Health receive a standard placement tariff for each undergraduate physiotherapy student on placement within the organisation.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.