Article Text

Statistics from Altmetric.com
Introduction
Intensive care unit (ICU) antimicrobial stewardship (AMS) interventions generally do not include nurses although their role is increasingly recognised.1–4 Previous literature described inclusion of nurses and nurse-led AMS interventions outside of ICU daily bedside rounds.5 6 After using a structured quality improvement (QI) evaluation of the daily bedside rounding model of the ICU clinical team we hypothesised the addition of ‘infection’ as an entity in the ICU nurses’ structured daily report would improve interprofessional discussion of infection management.
Methods
Setting
Thirty-bed, tertiary-care, medical-surgical ICU at an academic centre with an established AMS programme.7
Design
We used the QI improvement methodology of Plan, Do, Study, Act cycle to frame this project.
Phase 1: Plan: We identified process gaps in infection management occurring during ICU interprofessional rounds.
Workflow analysis identified that the nursing daily report provided unstructured information about infection status. Infection management discussions were limited to ICU pharmacists and physicians.
Focus groups found that nurses frequently did not know the indication for prescribed antimicrobials but perceived this knowledge to be important in providing safe and effective care.
Therefore, we proposed the introduction of ‘infection’ as a separate entity in the daily nurse report to provide structure for essential information dissemination and allow routine nursing inclusion in team discussions of infection management. Using the theoretical domains framework of behaviour change, we developed an intervention focused on nurses’ capability, motivation and opportunity to participate in discussion of infection management.8 9 Our phased approach used education, persuasion, training and enablement to facilitate behaviour change.
Phase 2: Do: We engaged ICU stakeholders, including nursing leaders, to design, implement and support inclusion of ‘infection’ in the nurse report.
During meetings with ICU physicians and pharmacists, we highlighted how prior AMS rounds had equipped them with a skill set to incorporate the framework for infection management (table 1) into their daily practice. They now needed to facilitate nurse participation.
Pre-intervention and post-intervention changes in inclusion of infection management decision-making framework components during daily bedside ICU rounds
Forums with ICU nurses provided the rationale for inclusion of ‘infection’ and addressed concerns regarding nursing role in management of infection. Similar forums with ICU pharmacists addressed concerns about redundancy of roles during bedside rounds.
We achieved consensus among all stakeholders regarding process and launch date.
At the launch, the AMS nurse provided ICU nurses with group or individual education. Stickers in the bedside nursing clinical summary tool (Kardex) served as visual reminders. The AMS nurse supported nurses by attending daily rounds and giving real-time feedback on their reporting.
Phase 3: Study: Post-implementation training and feedback to improve intervention acceptance and sustainability was performed.
Based on nursing feedback, we modified the training approach for new nurses, to include role-playing and scripts. Audit and feedback during rounds continued and additional visual cues were added to the ICU daily clinical flow sheet.
The primary outcome was frequency of discussion of each of the eight components of the infection management framework (table 1).
A convenience sample of pre-implementation and post-implementation interprofessional team bedside round discussions was audited (Monday to Friday) by a non-AMS team member (MSS) using an electronic tool (SimpleSurvey, OutSideSoft Solutions, Quebec, Canada). The ICU team was aware of the auditor but not the audit details.
Data were analysed using descriptive statistics.
Results
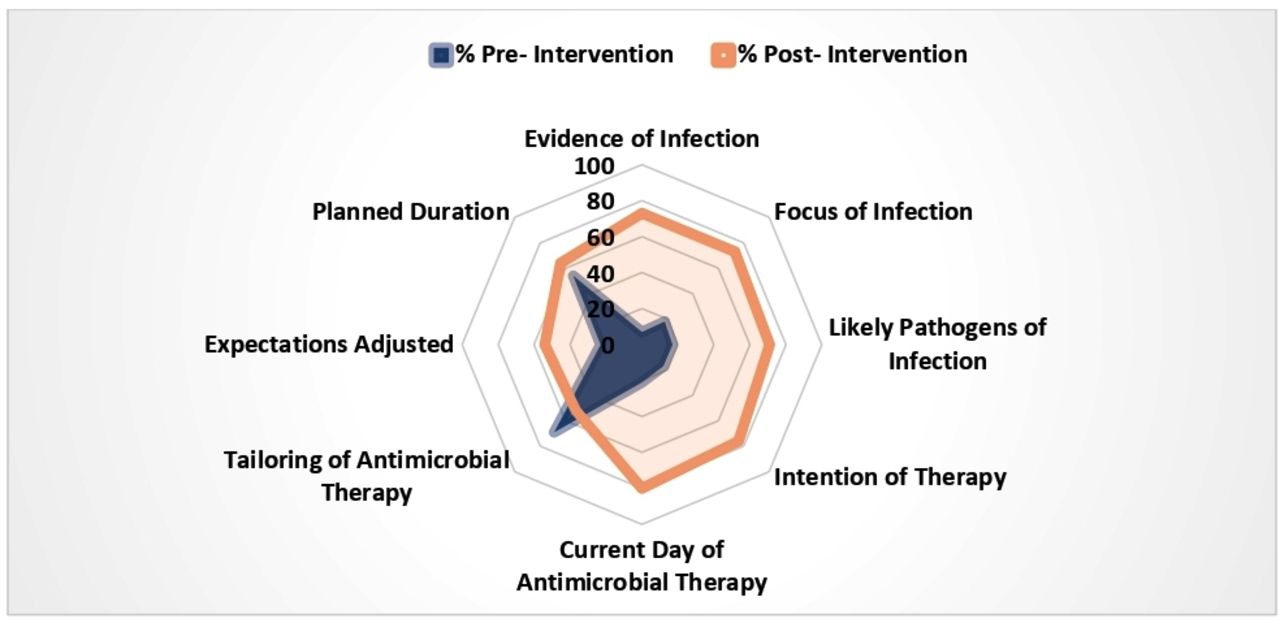
During the pre-implementation period (May 2017 to October 2017), 95 audits were completed and 217 were completed during post-implementation (October 2017 to August 2018). After implementation there was a statistically significant increase in discussion of each infection management component, except tailoring of antimicrobial therapy (figure 1, table 1).
{kind=link}
Decision-making framework component inclusion before intervention and after intervention.
Phase 4: Act: Over the subsequent 18 months, the intervention was scaled up and implemented into three additional ICUs across the institution. Ongoing feedback is provided to each ICU team weekly during AMS rounds based on appropriateness of antimicrobial prescribing.10
Discussion
A structured QI redesign of the daily bedside nursing report in the ICU to include ‘infection’ led to improved interprofessional discussion of key components of infection management.
This low-resource intervention did not disrupt workflow and increased nursing involvement. Seven of the eight components of infection management discussion increased. Decreased discussion of tailoring of therapy after intervention was unexpected; this warrants future investigation.
Few studies have described nursing engagement in AMS despite their recognised role and to our knowledge this is the first description of such an AMS intervention.1 5 6 By leveraging key aspects of behaviour change framework; motivation (need to know information for rounds), opportunity (incorporated into existing workflow), and capability (training and inclusion in discussion increases infection-related knowledge), our novel approach was successful in integrating nurses into bedside discussions of infection management.
Our AMS programme has been active in the ICUs of our institutions for greater than 10 years, therefore our intervention was largely independent of AMS guidance, and focused on the process of communication among the ICU interprofessional team. However, it was not without limitations as it was conducted in a single ICU that was already socialised to AMS. Our audit captured data related to the frequency of sharing of information and statement of planned actions, not quality of discussion. It will be important to explore relationships between quality of discussion and appropriateness of antimicrobial prescribing and patient outcomes. A larger, multicentre study with patient-specific outcomes would help understand the generalisability, feasibility and effectiveness of this approach in improving antimicrobial prescribing and infection management in ICUs.
Conclusion
Redesigning bedside nurse reporting to include infection is associated with improved infection management discussion.
Footnotes
Twitter @ASPLDD, @canuckIDpharm
Contributors LD planned the study, and contributed to the conduct of the study, data analysis and writing of the manuscript. LD is responsible for the overall content as a guarantor. MSS contributed to data collection for the study, initial data analysis and drafting of the study report and manuscript. MM contributed to planning of the study, data analysis and manuscript drafts. LJ contributed to the conduct of the study, data analysis and manuscript writing. SCJJ participated in the data analysis and manuscript revisions. SN participated in study planning, data analysis and manuscript writing. CB reviewed the study plan and provided review of manuscript drafts. AMM approved the study plan and provided review of data analysis and contributed to manuscript revisions.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval The study received approval from the research ethics board as a QI initiative.
Provenance and peer review Not commissioned; externally peer reviewed.