Article Text

Abstract
Catastrophic haemorrhage or carotid blowout a rare but devastating consequence of head and neck cancer. In most cases, this represents a terminal event, and the patient is prescribed pre-emptive analgesia and anxiolytics. There is anecdotal evidence that due to the time taken to prepare the medications that patients do not receive these drugs prior to death. We aimed to identify the drug to patient time using simulated catastrophic haemorrhage simulations. We used the current protocol for this and also proposed a new grab-bag with preprepared anxiolytic and anagelsic medications. Each scenario was repeated 16 times. The mean time for drug administration using the current policy was 124 s compared with 48 s when the grab-bag was used (p<0.01). The new protocol also reduced the variability in the drug to patient time. We aim to implement this new protocol on the head and neck ward.
- palliative care
- clinical protocols
- healthcare quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Catastrophic haemorrhage from head and neck cancer, or carotid blowout, is an uncommon but devastating complication of advanced malignancy. When an appropriate patient at risk of a carotid blowout is admitted to the Ear, Nose and Throat (ENT) ward, anticipatory sedatives and analgesia are prescribed with instructions to be administered should a haemorrhage ensue. However, current policy at National Health Service (NHS) Ayrshire and Arran is that the prescribed controlled medications cannot be stored at the patient’s bedside. There is some anecdotal evidence from nursing colleagues that due to rapid decline of the patient coupled with the time taken to prepare these medications at the controlled drug cupboard, that patients die without receiving anticipatory medications.
In this project, we primarily aim to quantify the drug to patient time once nursing staff have been made aware of a simulated catastrophic haemorrhage. We also propose changes to the current practice which we have also simulated. This aims to provide quantifiable evidence to promote a current change in practice.
Background
Catastrophic haemorrhage or carotid blowout is a severe consequence of advanced head and neck malignancy. The condition is defined as a rupture of the carotid artery and this can be caused by direct tumour invasion or as a complication of fibrosis of the tumour advnetitia secondary to the treatment of head and neck cancer. It occurs in approximately 4% of all head and neck cancer cases.1 Most patients at risk of carotid blowout have advanced disease and as such are being treated with palliative intent, with care focused on maintaining quality of life with treatment being aimed to alleviate symptoms. In these cases, such a haemorrhage represents a terminal event.2 3 Even in centres worldwide where carotid blowout is managed aggressively with endovascular repair, the mortality rate remains at 40%–60% and only approximately 23% of patients survive the event without major morbidity.1 4–8 The symptoms of carotid blowout are massive haemoptysis, haematemesis or neck hematomas with the mode of death being asphyxiation or exsanguination.
Palliative patients deemed to be at risk of carotid blowout are recommended to be prescribed anticipatory sedatives/anxiolytics.4 9 This treatment is thought to be necessary due to the dramatic and distressing nature of a catastrophic haemorrhage, and is aimed to relieve extreme anxiety and panic associated with the event. This is usually in the form of intra-muscular (IM) or intravenous (IV) dose of benzodiazepine. An anticipatory opiate dose may also be prescribed in patients where pain has been difficult to control to ease any pain.7
Measurement
In this simulated study, we chose to measure the drug to patient time following the initiation of a simulated catastrophic haemorrhage scenario. We measured both the time taken for the nursing staff to reach the patient (also referred to as the IM time) and the time taken for the drugs to be administered through a peripheral intravenous cannula (also referred to the intravenous time). This allows for the measurement and thus gives an indication as to the delay a patient would experience prior to receiving sedative medications in an acute event. This measurement also allows for direct comparison once standard protocols have been altered.
Design
Intervention
Current NHS Ayrshire and Arran policy with respect to anticipatory medication delivery is that all controlled drugs should be left unprepared within the controlled drugs cupboard. As such in an emergency situation, nursing colleagues would need to secure the keys for the controlled drug cupboard, identify the correct drugs, identify and open syringes and blunt ended drug preparation needles and prepare the medication with an appropriate amount of saline in syringe prior to attending the patient.
We aimed to reduce the number of steps that nursing colleagues need to undertake prior to attending the patient via the use of an emergency ‘grab bag’. Within this bag would be two preprepared syringes of sedatives and analgesia. The bag would be secured to the inside door of the controlled drugs cupboard, thus keeping the controlled substances secure. This would therefore mean that nursing staff would only need to secure the keys to the controlled drug cupboard once they have been made aware of a catastrophic haemorrhage.
Although this study uses simulated methods, we do propose a pathway for this to be implemented in practice. Once a patient at risk of carotid blowout has been identified by the clinical team, anticipatory medications would be prescribed and pharmacy contacted to approve the use of the grab bag. The medications could then be preprepared and the medications would be accounted for as prescribed within the controlled drug book. The bag itself would be marked specifically with the patient’s details including name, date of birth and unit number, and would then be secured to the inside door of the controlled drug cupboard. Training of this new pathway would be provided to all clinical staff to ensure this could be implemented safely and effectively.
Strategy
Our first aim was to quantify the drug to patient time once a catastrophic haemorrhage was identified by nursing staff on the head and neck ward. There were anecdotal reports from the staff on the ward that some patients experiencing carotid blowout die prior to receiving either anxiolytics or analgesia due to the time taken to prepare the medications from the controlled drug cupboard. We aimed to quantify the time it takes to prepare and deliver these crisis medications using the current standard NHS Ayrshire and Arran protocol.
The difficulty in studying catastrophic head and neck haemorrhage is that the complication is thankfully relatively rare, not all patients at risk of carotid blowout will be admitted to the hospital and the complication by its very nature is extremely unpredictable. Also, these haemorrhages are high stress situations which are not amenable to research protocols. As such, we decided to use simulated scenarios in order to facilitate timing of the delivery of crisis medications. A cannula was placed within the treatment room within the head and neck ward and secured to a table using tape. Two 10 mL vials of sterile water were labelled as dummy drugs, one labelled as midazolam and one as morphine, and were placed inside the controlled drug cupboard. Nursing staff were then informed that emergency simulation scenarios would be being conducted where a patient represented by the cannula would suffer a catastrophic head and neck haemorrhage that would necessitate the delivery of crisis medications from the controlled cupboard. They were informed to use the dummy medications and to assume that the prescription of the drugs is correct and the dose on the vial is also correct. During daylight working hours, the emergency buzzer would be pulled by one of the investigating team and a stopwatch started. Nursing staff were then timed as to how long it took to attend the patient with the prepared medications and the also the time taken for the complete delivery of these medications.
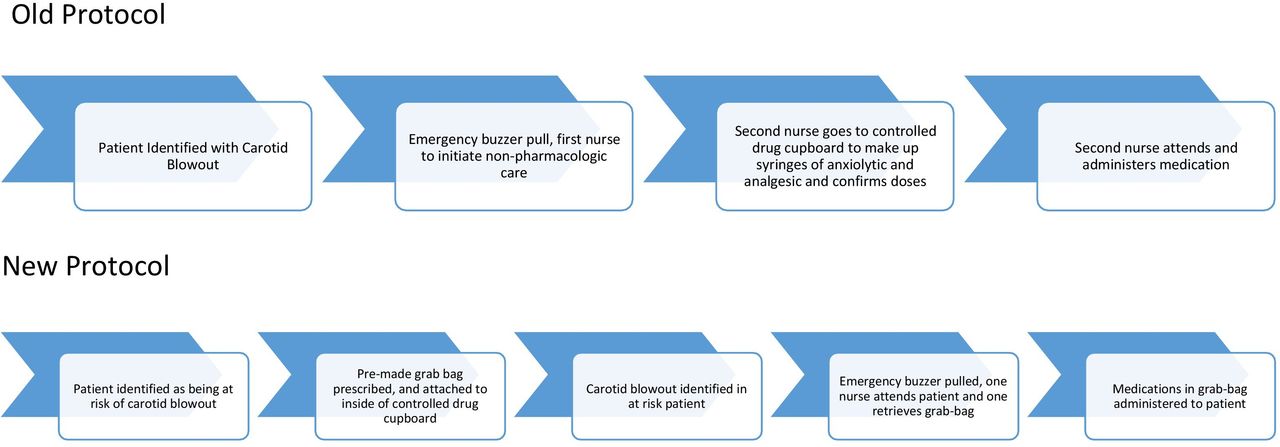
Following this initial simulation, we wanted to see if we could improve the drug to patient time with a simple intervention. In this intervention, two syringes were placed in a sealed polythene bag and were again labelled as dummy medications (one midazolam and one morphine as per the previous simulation). The bag was then taped to the inside door of the controlled drug cupboard. This was to ensure that the controlled drugs were still kept securely. The simulation was then conducted as before but on this occasion the nursing staff were advised to use the medications placed within the grab bag instead of preparing the medications themselves. As previously, nursing staff were again advised to assume the doses and the prescription of the medications was correct. The differences in the two protocols is outlined in figure 1. In total, 11 members of the nursing team participated in the project. Each scenario was then performed 16 times; this was performed to reduce the effect of times that could be considered as outliers. This also was done to ensure times were replicable. Data were analysed using the Wilcoxon ranked test.

{kind=link}
A process chart demonstrating the differences between the old protocol and the new protocol.
This quality improvement project was discussed an approved by the local departmental research team following consultation with both senior clinical staff, nursing staff and the departmental management team.
Results
Each of the scenarios were run 16 times. Staff who took part in each scenario routinely worked on the head and neck ward and were familiar with the current catastrophic haemorrhage protocols at NHS Ayrshire and Arran. The mean drug to patient time for intravenous administration in scenario 1 (current protocol) was 124 s with a range of 78–202 s. In scenario 2 (grab-bag protocol) the mean time for intravenous administration was reduced to 48 s. The range also reduced and narrowed to 33–53 s. The mean time to attend the patient in scenario 1 was 115 s compared with 42 s in scenario 2. Both the time to attend the patient and the intravenous administration time were shown to be statistically significant using the Wilcoxon ranked test, with p values of less than 0.01.
The variability in time noted in scenario one can at least in part be attributed to how nursing staff interacted with the controlled drug book. As investigators we did not specifically state in either scenario that controlled drugs were accounted for or not in the controlled drug book. In scenario 1, some of the longer scenarios occurred where the nursing staff opted to sign the controlled drug book prior to the administration of intravenous drug. Shorter scenarios occurred when the nursing staff opted to bring the controlled drug book to the patient. However, in scenario 2, all participants stated that as the drugs were placed in a separate storage area to the standard vials that something would be written in the controlled drug book to account for this, even though this was not explicitly stated to the participants.
Lessons and limitations
Catastrophic haemorrhage from head and neck malignancy is a commonly fatal complication and is distressing for patients, families/carers and nursing and medical staff. Previous guidelines focus on non-pharmacological measures primarily. The administration of sedative medication is now widely recommended in the literature with primary aim of alleviating the distress of the patient. There is some variation as to exact medications recommended and the route, but the most common is midazolam and second most common is an opioid such as morphine or diamorphine. While these medications are often prescribed for patients deemed at risk of carotid blowout, the time taken to prepare the medications combined with rate of bleeding and overall frailty of a terminal head and neck cancer patient means these medications are often not administered in time. The evidence we have for this is anecdotal as it is a difficult area to study.
Due to the unpredictability of a carotid blowout event coupled with the rapid decline of the patient, nursing staff are often the first responders to a catastrophic haemorrhage in secondary care, and may be the sole caregivers depending on how rapidly the patient declines prior to death. Nursing staff also therefore report feelings of helplessness and anxiety when managing a catastrophic haemorrhage. Similar negative feelings are reported within the literature with respect to interviews with family. These include: feared, traumatic, horrific and dreaded. A review of terminal haemorrhage also clearly states that the ‘imminence of death’ causes ‘overwhelming distress’ to patients.3
Scottish palliative care guidelines focus on non-pharmacological methods in the management of carotid blowout including: not leaving the patient, the use of dark coloured towels to cover blood loss, staying calm and not shouting for help. Pharmacological methods are only currently recommended if time allows and if a second staff member can prepare the medications so as not to leave the patient.10 From our simulation, where the average time to administration is over 2 min and was as long as 3 min and 20 s, the current guidance would appear sensible as one would expect a patient to derive reduced benefit from the medication following this delay. However, by implementing a fairly simple alteration in practice with a grab-bag, these times can be reliably reduced to under a minute. We feel that this means that pharmacological therapies could be given further credence in the management protocol, without compromising non-pharmacological methods. This also provides nursing colleagues with another strategy in the management of a major haemorrhage.4 11–14 As a group would advocate a single grab-bag be prepared once a patient on the head and neck ward be identified by a senior clinician as being at risk of catastrophic haemorrhage. The contents is prescribed to the at risk individual only and would only be replaced if the medications expired or the syringe was noted to be damaged. It had been proposed that the drugs could be kept in patient’s individual rooms; however, this raises some safety concerns regarding controlled drugs being left unmonitored. We feel our current approach represents a compromise between efficient pharmacological treatment and patient safety.
However, it should be noted that the overall efficacy of both pharmacological and non-pharmacological management of terminal haemorrhage is based on low level evidence. Two recent systematic reviews both noted that the majority of all management recommendations with respect to terminal haemorrhage arises from level 5 evidence (expert opinion). Both studies also note the need for further high-level research into the area, although this may be extremely challenging due to ethics and emotion regarding the event and the practical ability to recruit a large enough patient cohort.4 9
The aforementioned variance in timings with respect to the controlled drugs book was an interesting and unexpected finding. Prior to the simulation, there was no explicit instructions regarding the controlled drugs book. Participants were informed to behave as they would in a real emergency scenario but to assume that correct doses of medication were prescribed and the dummy vials represented that correct dose. Participants stated that as the syringe was already drawn up, they assumed that doses would already be accounted for within the controlled drug book even though this was not explicitly stated. The variable responses with respect to this aspect of the simulation demonstrates the need for an explicit statement about how nursing colleagues should document the administration of a controlled drug in a time dependent emergency.
As carotid blowout is a rare event, simulation modelling was deemed to be the best method to assess team performance. Simulation also allowed for a predesigned clinical episode, as waiting for multiple actual clinical episodes would not have been possible. However, the efficacy simulation studies have only been studied with observational studies although with largely positive results. There has yet to be validation with experimental studies. Also, some observational studies have noted that repeated simulation can promote abnormal learning, for example, if the scenario was run too many times in one shift the nurses may run straight to the drugs cupboard on hearing the emergency buzzer rather than to the patient room. Simulation studies also rely on a rigid protocol to ensure reliability but as a result this makes simulation less flexible and adaptable than a more common quality improvement methodology such as a plan, do, study, act (PDSA) model.15–17
Conclusion
Carotid blowout is in most circumstances a terminal event in a patient with advanced head and neck cancer being treated with palliative intent. Anxiolytics and analgesia administration are well reported in the literature to alleviate the patients distress and pain. However, due to time taken to prepare these medications and the rapid decline of the patient, these medications may never reach the patient. Policy documents promote the importance of non-pharmacologics in the management of an acute major haemorrhage.
Our simulation demonstrate that the time taken for intravenous anxiolytics and analgesia to be prepared and administered can take on average 2 min. However, with a preprepared grab bag for patients identified at being at risk of carotid blowout, this time can be reliably and repeatedly reduced to under 1 min.
Following this quality improvement project, we aim to produce a local guideline policy document for the management of catastrophic haemorrhage in patients with head and neck cancer being managed with palliative intent within NHS Ayrshire and Arran. We are in discussions with our pharmacy colleagues to enable the introduction of the grab bag of drugs for patients deemed at risk of a carotid blowout within the ENT ward. These drugs will be preprescribed and also accounted for in controlled drugs book prior to any major haemorrhage. We have taken this project forward by providing further training to our nursing colleagues regarding the management of this difficult situation, particularly focusing on non-pharmacological methods and pharmacological methods.
References
Footnotes
Contributors PS and RT planned and developed the idea for the quality improvement project. PS conducted the literature search, undertook some of the data collection, undertook the statistical analysis, and produced the manuscript. AT undertook a significant part of the data collection and also aided with statistical analysis. RT supervised the project and aided with review of the manuscript and performed liason with our pharmacy colleagues.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.