Article Text

Abstract
The demand for systemic anticancer treatment continues to rise due to the increasing numbers being diagnosed with cancer and developments in treatment options. The net result is greater pressure on services and subsequent patient delays. Delays in treatment could decrease the benefit of the therapy and be detrimental to patient experience. Patients with human epidermal growth factor receptor-2 (HER 2) positive breast cancer within Raigmore Hospital waited an average of 41 min from the scheduled appointment time despite the administration of subcutaneous (SC) trastuzumab being scheduled for a 15 min treatment window. Given the frequency of these injections, this was having an adverse impact on patients and services. The aim of this project was for patients with breast cancer to receive treatment within the 15 min window. Lean principles were applied to reduce waste and increase value. Exploration of the problem led to the solution of relocating the administration of SC trastuzumab from the Macmillan Day Bed Unit (MDBU) to the Highland Breast Centre (HBC). Multiple improvement tools and techniques were used to implement the change. Data were collected on the median number of treatment episodes of SC trastuzumab per week at baseline and patient wait from appointment time to treatment completion was calculated at baseline and as an ongoing measure. Patient experience feedback was gathered following relocation of the treatment. Following relocation, the average time from scheduled appointment to discharge was 14 min (66% reduction). Patient experience feedback was positive and identified an unanticipated outcome; the regular Friday afternoon clinic, identified as most efficient for the service, was found by patients to be particularly convenient for their own planning. Through the application of Lean principles, the service was redesigned in a cost neutral way and resulted in a reduction in the wait time for treatment.
- continuous quality improvement
- efficiency
- organisational
- healthcare quality improvement
- lean management
- PDSA
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- continuous quality improvement
- efficiency
- organisational
- healthcare quality improvement
- lean management
- PDSA
Problem
In 2018, there were approximately 2.1 million newly diagnosed female breast cancer cases in the world.1 The demand for systemic anticancer treatment (SACT) continues to rise due to the increasing numbers being diagnosed with cancer and developments in treatment options.2–4 The administration of subcutaneous (SC) SACT is part of the standard treatment for people with a diagnosis of human epidermal growth factor receptor-2 (HER 2) positive breast cancer.5 6 Timely treatment improves patient outcomes and experience. An audit within Raigmore Hospital found that patients with HER 2 positive breast cancer waited an average of 41 min from the scheduled appointment time despite the administration of SC trastuzumab being planned as a 15-min treatment window.
SACT is delivered in six areas throughout NHS Highland as a hub and spoke model, with the majority of treatment administered within Raigmore Hospital. The oncology/haematology ward and the Macmillan Day Bed Unit (MDBU) are the designated areas for SACT administration within Raigmore Hospital. Since the MDBU was opened in 2003, the estimated population of NHS Highland has increased from 316 474 to over 320 000 people,7 increasing the number of people who may require the use of cancer services in NHS Highland. Furthermore, as SACT regimen options increase and treatments become more successful, more people may be receiving SACT for longer. But, despite rising demand, the capacity for delivering SACT treatment in NHS Highland remained unchanged. This resulted in four key challenges: greater pressure on the oncology/haematology ward and MDBU to accommodate increasing numbers of patients, more patient feedback of long waits, limited physical space in the two designated administration areas and a shortage of SACT trained nursing staff.
NHS Highland is well versed in quality improvement (QI) methods and some staff have expertise in Lean improvement methods. The project aimed to ensure all patients receiving SC trastuzumab in Raigmore Hospital for breast cancer would be treated within 15 min of their scheduled appointment by end July 2019. The project commenced in January 2019.
Background
Trastuzumab is a monoclonal antibody that interferes with the HER2 and inhibits cancer cell growth. Trastuzumab belongs to the group of cytotoxic chemotherapy drugs and forms part of the standard treatment offered to people with HER2 positive breast cancer who are suitable for chemotherapy.5 8 A randomised clinical trial found comparable efficacy in administering SC trastuzumab compared with the traditional intravenous route, an increased patient preference for SC trastuzumab, and cost savings for nurses time.9 Others have echoed the usefulness of Lean principles to reduce waste and increase value when administering SC trastuzumab.10 11 However, overall evidence of the effectiveness of Lean application in healthcare remains limited.12 13
Given the risks associated with handling and administering SACT treatments such as trastuzumab, those handling and administering SACT must comply with nationally applied guidance.14 15 SACT medications are administered by nurses who have undergone additional training. There are, however, shortages of such nurses within the UK, as well as internationally.16 17 Shortages are exacerbated as at least two staff, who are fully trained in the safe administration of SACT, are required in order to administer the treatment.14 This training may be part of a programme to equip staff to administer both SC trastuzumab and intravenous chemotherapy to patients, which typically requires 200 learning hours.18 However, separating out the administration of SC trastuzumab from other chemotherapy regimens reduces the need for the formally accredited course; rather an understanding of SC Transtuzumab administration and waste disposal is sufficient.14
Patients have reported that waiting for SACT administration is an important aspect of their experience. A study by Mitchell19 exploring patients’ experiences of receiving SACT on a mobile chemotherapy unit found waiting time in a clinic for treatment to be of great importance to patients and supporting significant others. The study also found that patients’ quality of life dramatically improved by less waiting.19 This project aims to improve this important aspect of patient experience, specifically, to reduce patients wait time to less than 15 min per each administration of SC trastuzumab.
Measurement
A measurement plan was developed collaboratively with the Project Team (see online supplemental additional file 1: measurement plan). Data were retrospectively collected for 123 weeks on the median number of treatment episodes of SC trastuzumab per week at baseline from ChemoCare (Chemotherapy electronic prescribing system) to guide capacity and determine whether changes were improving the system. The baseline data found that, over the 13 weeks, there was an average of 10 treatment episodes per week. As treatment was scheduled for 15 min per treatment episode, this equated to 150 min of scheduled treatment time required per week. Baseline data also showed that there was an average time of 41 min from patients’ scheduled appointment time to their treatment episode discharge. As SC trastuzumab is scheduled as a 15 min treatment, this showed an average waste of 26 min per appointment episode. For patients having adjuvant SC trastuzumab for primary breast cancer following their chemotherapy regimen, 15 treatment episodes are recommended, with a 3-week interval between each treatment. For people having SC trastuzumab as treatment for secondary breast cancer, the number of treatment episodes is typically longer, sometimes for as long as tolerated. This frequency of treatment episodes gives context to how the patient’s quality of life is adversely affected by the ongoing waste of waiting in the clinic for this treatment.
Supplemental material
Patient wait time from scheduled appointment to treatment completion per patient episode was calculated at baseline and as an ongoing measure. Scheduled appointment time, arrival and discharge time are routinely captured on ChemoCare. Wait time was recorded and presented on an individual chart (i-Chart) per appointment episode for 12 months of data.
Given that the central premise of Lean is to reduce waste and increase value from the customers’ (in this case patients’) perspective20 it was important to capture patient experience. This was captured using an open-ended patient feedback form with the statement “Please leave your comments on having your Herceptin treatment at the breast unit today”. Additionally, some staff highlighted concerns that the change of location might upset some patients, particularly patients with secondary breast cancer who may not have ever been seen in the Highland Breast Centre (HBC), but were familiar with the staff and environment at MDBU. It is important to consider and measure whether improving one aspect of care has unanticipated impacts on other aspects of care—often referred to as balancing measures.21 The feedback form was offered to patients for the first month following administration of SC trastuzumab in the HBC.
Design
The Lean approach was selected as the Macmillan Person Centred Care Project Lead (AM) had recently completed a postgraduate module in Lean application; she coached other staff in the process. Many staff had previously used Plan, Do, Study, Act (PDSA) cycles. There are various definitions of what constitutes Lean methodology.13 However, there is consensus of the five key Lean principles. Namely, determining value from the customers (ie, patients’) perspective, understanding the value stream (how much is value and how much is waste), improving flow, creating a pull system and continually striving for perfection.12 Waste had been identified in the system, that is, patients waiting. This waste was highlighted by audit data, listening to patients and staff and completing a process flow map of the current process (see online supplemental additional file 2: process flow maps. Locally, very few formal problems are reported from this patient group, but patients often waited long periods for staff availability. Reports of patients having to reschedule other appointments and commitments were not unusual. The project focused on reducing the wait by redesigning the service and testing aspects of change, using PDSA cycles.22
Supplemental material
A collaborative team was identified. The project team consisted of the Medical Divisional Nurse Manager, Cancer Services Manager, SACT Nurse Consultant, Head of Oncology Pharmacy, Surgical Assistant Divisional Nurse Manager, Cancer Quality Manager, Divisional Midwifery/Nurse Manager, HBC Senior Charge Nurse and the author (as QI facilitator). As the project progressed, an Oncology Pharmacist and the SACT Advanced Nurse also joined the project team.
The project team explored potential solutions for the SACT service. It was suggested that SC trastuzumab (which is typically administered in MDBU) may be administered out with the designated SACT areas, if the SC trastuzumab is not given alongside intravenous SACT. Further exploration identified the HBC as an alternative location. The HBC had times of unused clinical space and potential nursing staff capacity. Furthermore, for women receiving SC trastuzumab as adjuvant treatment for primary breast cancer, the HBC offers a familiar environment from their initial diagnosis and follow-up care. The full implications of relocating the treatment were explored and a driver diagram was created collaboratively to identify the implications and actions (see online supplemental additional file 3: driver diagram).
Supplemental material
Staff at the HBC agreed to administer SC SACT following training. The HBC team welcomed the change and identified Friday afternoon as a suitable time for this service, when there was known physical space capacity and available HBC nursing staff. Following agreement of the proposed change by HBC staff a plan was created (see online supplemental additional file 4: project plan). The project plan focused on preparing staff, systems and patients for the administration of SC trastuzumab within the HBC.
Supplemental material
With regards to the environment for administering SC trastuzumab, group members were mindful to comply with national requirements for delivery of SACT out with designated cancer units.14 The oncology pharmacy team assessed the HBC clinical areas and ensured all necessary processes were in place for administration of SC trastuzumab. This included arranging suitable transportation of the drug, providing sharps disposal containers and a SACT spillage kit.14 It was agreed that a pharmacy technician would deliver the drug, batched together for the patients, half an hour prior to the first appointment and that the drug would be stable at room temperature for the duration of the treatment episodes.
For administrative systems planning, forms were completed to install ChemoCare in the HBC. A clinical template was created to trigger patient notes to be delivered to the HBC rather than the MDBU. Administrative staff at MDBU were available to assist administrative staff at the HBC should guidance be required.
The SACT consultant nurse arranged training for the HBC nurses in safe administration and disposal of SC trastuzumab, which included direct teaching and observation. Trastuzumab is a monoclonal antibody and not a chemotherapy drug. Therefore, training focused on the differences between administration of SC trastuzumab in comparison to other SC injections, that is, injections should be given at least 2.5 cm from the old site, ideally alternating administration sites.23 24 All agreed that the competency for administering SC trastuzumab would be the same in principle as other medications.24 Staff observed the procedure, asked questions and carried out supervised practice until competent before practising independently.
A patient letter was created to advise patients who were having their SC trastuzumab at the MDBU of the change of location. This letter was sent to patients 1 month prior to the planned change to allow patients adequate time for questions and planning. The letter was drafted and tested for understanding with an existing patient.
The HBC Senior Charge Nurse and clinic nurses were trained to check, administer and dispose of the drug safely, and populate ChemoCare accordingly. The SACT senior nurse was also available at the HBC for advice and support on the day of the proposed change, and thereafter as required. The first author (AM) would also be in attendance in the role of QI facilitator. Being present in the workplace or ‘Going to the Gemba’ is a key Lean strategy to understand the process and people in context.25 The QI facilitator observed the patient flow and captured feedback from staff. The ergonomic design of the workplace and processes are key Lean tools to improve flow.26
It was anticipated, through training of HBC administrative and nursing staff, involvement from pharmacy, data collection to anticipate the volume of treatment episodes and clear communication with relevant patients, that all possible preparations were in place to ensure a smooth transition of administration of SC trastuzumab from MDBU to the HBC. It was hypothesised that relocating the service to an area with some capacity would reduce waiting times (reducing waste) for patients to receive their SC trastuzumab and therefore enhance the patient experience by receiving treatment in a timely manner (increasing value). It was also hypothesised that this change would release some capacity for more complex SACT to be delivered in MDBU.
Strategy
Numerous PDSA cycles were conducted to test and implement new ways of working. Initially, lengthy PDSAs were used in planning before using rapid PDSA cycles for testing and implementation. Example summaries are detailed below.
Example of planning PDSA: establish minimum training required, check with nurses in HBC if they are confident in this, and complete training by week 12
Plan: the purpose of this PDSA was to prepare designated HBC nursing staff for safe administration and disposal of SC trastuzumab in the HBC. The indicators of success were the HBC nurses completing agreed training, the SACT nurse assessing HBC nursing staff as competent in this activity and the HBC nurses’ self-reported confidence in this activity. The data for these indicators of success were gathered informally from discussions between the experienced SACT and HBC nurses. This plan involved one HBC clinic nurse, the HBC charge nurse, the MDBU senior SACT nurse and the SACT Nurse Consultant. The time frame for this training was estimated to be 10 weeks.
Do: from February 2019 to April 2019, designated HBC nurses observed SC trastuzumab being administered in MDBU. During this period, the HBC nurses also received training from SACT nurses in safe handling and disposal of the drug, and potential side effects of treatment.
Study: the HBC nurses involved were deemed as competent to administer SC trastuzumab. This was 2 weeks ahead of the planned prediction for HBC staff readiness. This also increased confidence in all the staff involved that the training plan was effective.
Act: training was successful and within time planned. Any queries from HBC staff regarding SC trastuzumab not yet covered in training will be directed to SACT nurses or oncology pharmacy and be captured for future PDSA cycles.
Although the use of PDSA cycles was not as tests of change per se, but rather as readiness towards a change date, the eventual strategy was effective as all staff were confident of the systems and strategies in place by the time of relocation to HBC. Furthermore, there were no adverse events on the first day (or indeed to date).
Example of rapid PDSA: administering SC trastuzumab in HBC
Plan: gather views of HBU staff on progress of SC trastuzumab service in HBU.
Do: QI facilitator spoke to HBU nurses to gain feedback.
Study: one staff nurse was unclear of the process when variations occur, such as patients who do not attend, or a patient who attends with influenza like symptoms. Also, new staff are attending to help administer SC trastuzumab, but are not trained to use ChemoCare. On one occasion, the two HBC nurses trained in SC trastuzumab administration and ChemoCare were both off work, so one had to come in from annual leave to cover the clinic.
Act: a checklist was created for all aspects of SC trastuzumab administration. As well as being a useful aide memoire for the HBU staff, it would also ensure standard work. ChemoCare training and permissions were extended to other staff members to reduce dependency on two staff members only.
Results
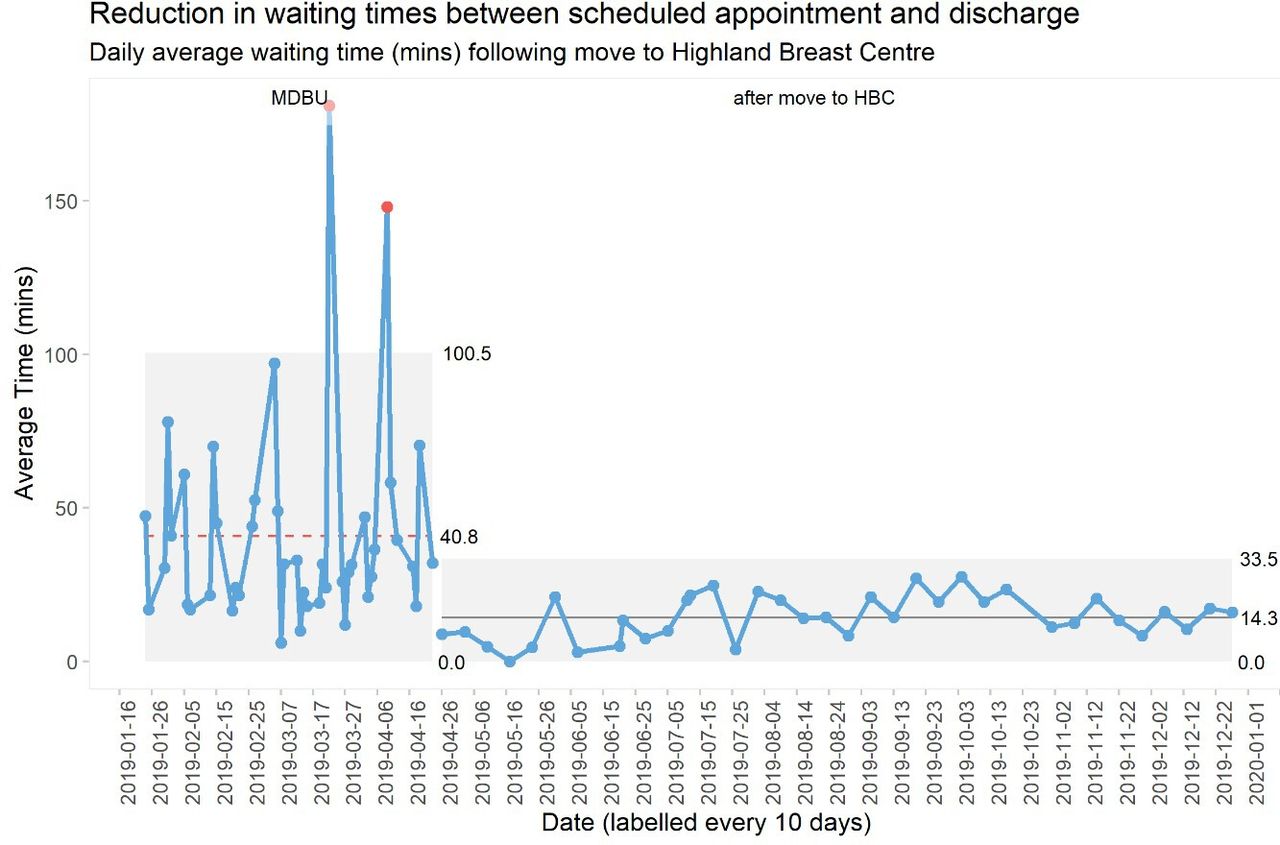
The i-Chart at figure 1 plots the number of minutes taken for each treatment episode. Waiting times for patients between scheduled appointment and discharge for SC trastuzumab were presented on an i-Chart as each data point has a single data value for each treatment episode.27 Results displayed in figure 1 show a marked reduction in waiting times. The median waiting time goes from a baseline of 41–14 min, therefore achieving the main outcome of the project. The clinic was relocated in April and the data on the run chart show an improvement even at the end of December 2019. This i-Chart shows evidence of a sustainable change over time, therefore indicating actual improvement, rather than random variation. Note that those figures plotted below zero indicate patients who arrived earlier than their scheduled time. As the HBC nurses were solely dedicated to this service, they were regularly able to take patients slightly earlier than their scheduled time and administer the drug immediately.

{kind=link}
Time from scheduled appointment to discharge for subcutaneous trastuzumab. HBC, Highland Breast Centre; MDBU, Macmillan Day Bed Unit.
While there were initial concerns regarding the possibility of patient experience transferring the location of treatment being negative, the patient feedback did not support this. There were also initial staff concerns that prompt treatment episodes at HBC would be ‘too quick’, potentially limiting therapeutic discussions. However, patient feedback did not support this either.
Patient feedback was summarised into key areas and frequency counts to give an ‘at a glance’ view of findings (see table 1). As well as supporting the aim of the project, the patient feedback indicated many positive experiences. Every Friday afternoon had been identified as a suitable time for clinic space and staffing in the HBC (a service perspective). Interestingly, from a patient perspective, this timing was found to be particularly convenient for ease of transportation and forward planning.
Patientfeedback
The patient feedback on waiting times supported the patient centred aim of reducing the length of time waiting for SC trastuzumab. Waiting is a commonly recognisable waste.28 Important factors with regards to patients’ perspectives of quality of care include a compassionate care provider, trust in their clinician and a minimum waiting time to be seen for appointments.29–31 Encouragingly, all these factors were evident in the patient feedback.
Lessons and limitations
This project achieved the aim of reducing patients wait for the administration of SC SACT. Complex problems can sometimes be fixed with simple solutions. Simply changing the location of SC SACT enabled reduced patients waits. Changing the location of SACT treatment for patient centred reasons has been demonstrated by others.19 The transfer of administration of SC trastuzumab from one setting to another, involving new staff, is an excellent example of what Nelson et al32 describe as an adaptive healthcare clinical microsystem working to its aims by flexibly addressing the needs of the microsystem. Small changes can have larger effects on the system. Beyond the capacity for flexibly addressing organisational needs, evidence of what Krantz33 termed ‘sophisticated change efforts’ in the behaviours of all involved in the change was apparent. This was exemplified in the careful planning ahead of the change, combining both human and technical factors to enable project success. Involvement of all stakeholders from the initial idea to implementation was essential.
The use of checklists was a popular concept for staff, both as a transition aid memoir and ensuring consistency of the procedural administration of SC trastuzumab. Checklists have been widely used in QI and can be helpful in mistake proofing.34 However, we think a combination of both technical QI tools and team involvement enabled this successful project.
The QI culture embedded in NHS Highland7 was evident as the project team observed many behaviours aligned with QI processes, such as the language used and the fundamental value of daily management practice.35 However, on reflection, the evolving tone of the project became ‘let’s do it’ rather than ‘let’s test it’, due to the clinical urgency of capacity in the MDBU. For example, a small test of change using one patient being transferred to HBU for SC trastuzumab would have been informative. PDSA testing would also have likely highlighted the need for other staff members to be given access to ChemoCare. Instead, due to eagerness to solve the ever-increasing pressure on SACT delivery, the focus of the project team was on planning for whole transfer by a defined date. Even so, on reflection, the use of PDSA testing provided valuable learning points for the team. While some may think that small-scale PDSA testing will increase the length of implementation time, the reverse is likely to be true. We would advise trusting the process. More extensive small-scale testing would have helped to identify and resolve issues earlier, which would also have accelerated implementation, as well as reducing risk. This lack of adherence to the concept of small-scale testing to inform an improvement is common. Taylor et al,22 in their systematic review of the application of PDSA cycles, noted that only 15% of the reviewed improvement work reported the use of quantitative data at regular data intervals to inform progression of PDSA cycles, suggesting a lack of cohesive understanding of the use of PDSA cycles as an improvement method. While planning for the relocation of service was robust, and the measures have shown it was indeed an improvement in terms of patient waiting times, PDSA cycles could have provided quicker insights.
A limitation of the project could be that data were not collected beyond 12 months. We do not know whether the project was sustainable beyond this period. There was an ongoing necessity to balance sufficiency and necessity. However, the data demonstrated a signal of change over an 8-month period, as opposed to random variation.
One of the criticisms of Lean in healthcare is limiting application to reducing waste.12 13 While this project focused on reducing waste (waiting) other Lean principles were applied, but not all Lean tools were formally applied. For example, while we recognised value from the patients’ perspective, we did not create a value stream map (VSM). Creating a VSM would have provided more robust evidence of the waste in the current process and would have enabled patients to be more involved in the development of the value stream. The essence of Lean problem solving—empowering workers to problem solve while focussing on quality, the service user and respect for people36—was evident in all stages of this project, and this goes beyond considering just waste.
While patient needs, such as waiting time, were considered throughout the project, and patient involvement was sought, their level of involvement was limited. There was likely an element of serendipity that patients liked some of the aspects of the relocation, such as Friday clinics. With hindsight involving and engaging patients and public should have been evident throughout all stages of the project. Evidence suggests that their perspectives are unique and if used effectively can improve implementation and sustainability of improvements.37–39 For example, the nature of the patient feedback sheet may have been more considered. Although the open patient feedback sheet did provide insights, and it was noteworthy that reduced waiting time was commented on without prompting, a patient feedback tool with an appropriate level of reliability and validity would have provided more robust information.40
As with all QI projects, the context is a key factor in determining outcomes; therefore, these results may not be generalisable to other settings. Despite this there are valuable lessons for others, such as engagement with all stakeholders from the beginning of the project, using small scale PDSA cycles, listening to patients and a willingness to adapt plans en route.
Conclusion
In conclusion, patients were waiting too long for administration of their SC trastuzumab which impacted on their quality of life. Waiting for their administration within the Macmillan Day Bed Unit (MDBU) and general ward also added to the existing pressures on staff working in these areas. By creating a platform to brainstorm, foster cooperation across teams, maintain momentum and provide careful planning, this problem was creatively resolved while adding quality to the patient experience. The specifics of this particular project may not be generalisable to other settings. However, the improvement platform which supported it will be widely applicable to adaptive healthcare clinical environments working to flexibly address the needs of the microsystem.
Acknowledgments
The authors would like to thank the patients and staff from the Highland Breast Centre (HBC) who contributed to this quality improvement project. They would also like to thank John MacKintosh (QI Data Manager, NHS Highland), and Fraser Mackellar (Cancer Quality Manager, NHS Highland) for assistance with data display. Many thanks to Brian James for his thorough proofreading.
References
Footnotes
Twitter @BeattieQi
Contributors This project was codesigned by FC, DM, EG, LM and AM. MB supervised the project throughout. AM conducted data collection, observations and analysis. MB drafted the paper and all authors revised before agreeing the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This work met criteria for operational service improvement work exempt from research ethical review. The project was registered with the local Clinical Governance Department (Project Registration number 2019/20 – 011)
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.