Article Text

Abstract
Background Over recent decades, CT scans have become routinely available and are used in both acute medical and outpatient environments. However, there is a small increase in the risk of adverse consequences, including an increase in the risk of both malignancy and cataracts. Clinicians are often unaware of these facts, and this represents a challenge for medical educators in England, where almost 5 million CT scans are done annually. New whiteboard methodologies permit development of innovative educational tools that are efficient and scalable in communicating simple educational messages that promote patient safety.
Methods A short educational whiteboard cartoon was developed to explore the prior observation that adolescents under the care of paediatricians had a much lower risk of receiving a CT scan than those under the care of clinicians who care for adults. This explored the risks after receiving a CT scan and strategies that can be used to avoid them. The educational cartoon was piloted on new doctors who were attending induction training at a busy teaching hospital.
Results The main output was the educational whiteboard cartoon itself. Before the new medical trainees’ induction, 56% (25/45) had received no formal training in radiation awareness, and this decreased to 26% (6/23) after the exposure to the educational cartoon (p=0.02). At baseline, 60% (27/45) of respondents considered that young females were at highest risk from exposure to ionising radiation, and this increased to 87% (20/23) after exposure to the educational cartoon (p=0.06).
Conclusions This proof-of-concept feasibility study demonstrates that whiteboard cartoons provide a novel and feasible approach to efficiently promote patient safety issues, where a short succinct message is often appropriate.
- medical education
- patient safety
- communication
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The use of ionising radiation in diagnostic imaging is an integral part of modern medicine, and enables the prompt diagnosis and delivery of appropriate treatment globally. As a consequence, CT scanning in particular has become readily available in hospitals in high-income countries, and is often a first line investigation for acute medical and surgical admissions.
However, although CT scans facilitate optimal medical treatment, exposure to ionising radiation is associated with a small risk of adverse health outcomes in the longer term. These include an increased risk of malignancy1 and cataracts,2 which while small in absolute terms, is higher in younger patients and because of the high volume of CT scans is potentially important from a public health perspective.3 While assessment of the appropriateness of any clinical decision making is often challenging, with a variation of practice within an acceptable spectrum, there is an almost threefold increase in the risk of receiving a CT scan when moving from care under a paediatrician to that of a physician for adults.4 This is unlikely to be a consequence of an increase in rates of disease, and a reflection of the emphasis placed by paediatric clinicians in avoiding exposing their younger patients to ionising radiation.
We have recently evaluated awareness of the long-term health consequences of exposure to ionising radiation by clinicians in a busy acute medical teaching hospital in the UK.5 This demonstrated that 35% of respondents had received no formal training on the risks of exposure to ionising radiation with the implication that medical training has struggled to respond to the use of CT scanning becoming commonplace in recent decades.3 A variety of educational approaches including simple scalable interventions are required to rectify the asymmetry between CT availability and awareness of their long-health consequences by clinicians who request them. Advances in cartoon software have made simple educational messages deliverable and relatively affordable. Whiteboard video, whereby pictures are drawn by a hand on a white background in a time-lapse motion accompanied by narration, have recently been shown to improve patient knowledge in a healthcare context.6 Messages that involve familiar brands, individuals and places are often more interesting and hold the attention longer than generic messages that have little familiarity to the viewer. This facet of human psychology is called the mere-exposure effect and is often used by the advertising industry to capture attention and sell products.7 We used this approach to develop a pilot educational cartoon on the long-term risk of radiation exposure using two local clinicians, and evaluated the efficacy of this approach in clinical trainees who were starting work at the teaching hospital using a before and after study design.
Methods
Educational cartoon development
The educational cartoon was generated in a number of stages. The first was to produce a short narrative with an educational message. This involved a radiologist and a paediatrician, who initially discussed the potential benefits and costs of ionising radiation exposure, and then how paediatricians minimise these exposures when possible. The second stage was to collect an audio of the narrative, using a combination of scripted prose and a more interview-based approach to addressing the matters of interest. Once the final audio was edited, this was then sent to the whiteboard animation team along with some photographs of the narrators and the hospital environment. These were converted into the final educational cartoon using Adobe Creative Suite and Videoscribe software.
Data collection on radiation awareness in trainee clinicians
All trainee clinicians from all medical specialties who started working at the Royal Derby Hospital in August were invited to attend an induction session which aims to prepare them for their new workplace. The educational cartoon was presented to 189 attendees who attended this session, and not available subsequently. The trainees did not have the opportunity to watch the video if they did not attend the induction. Nevertheless, all trainees that completed the pre-induction questionnaire did attend the induction. All doctors who were known to be starting were sent an email with a simple internet-based survey of their training in and knowledge of the long-term effects of ionising radiation exposure (www.surveymonkey.co.uk) before the induction session. Six weeks later, the same group of doctors were asked to participate in second survey consisting of the same questions. Only a few questions were asked and the responses were simple categorical options. This was to try and optimise the response rate as in our experience doctors-in-training are very busy and unlikely to be able to complete long, complicated questionnaires. To provide an incentive to respond, an electronic tablet was offered to one respondent who had participated in both surveys and was selected randomly.
Patient and public involvement
There was no formal patient and public involvement. However, from their clinical roles, the authors are aware that overuse of CT scans is a potential concern for both patients and hospitals.
Results
Whiteboard cartoon
The final whiteboard educational cartoon can be seen at https://www.youtube.com/watch?v=cZRBmSLTnWA&feature=youtu.be.
Before and after whiteboard cartoon exposure surveys of trainee doctors’ radiation awareness
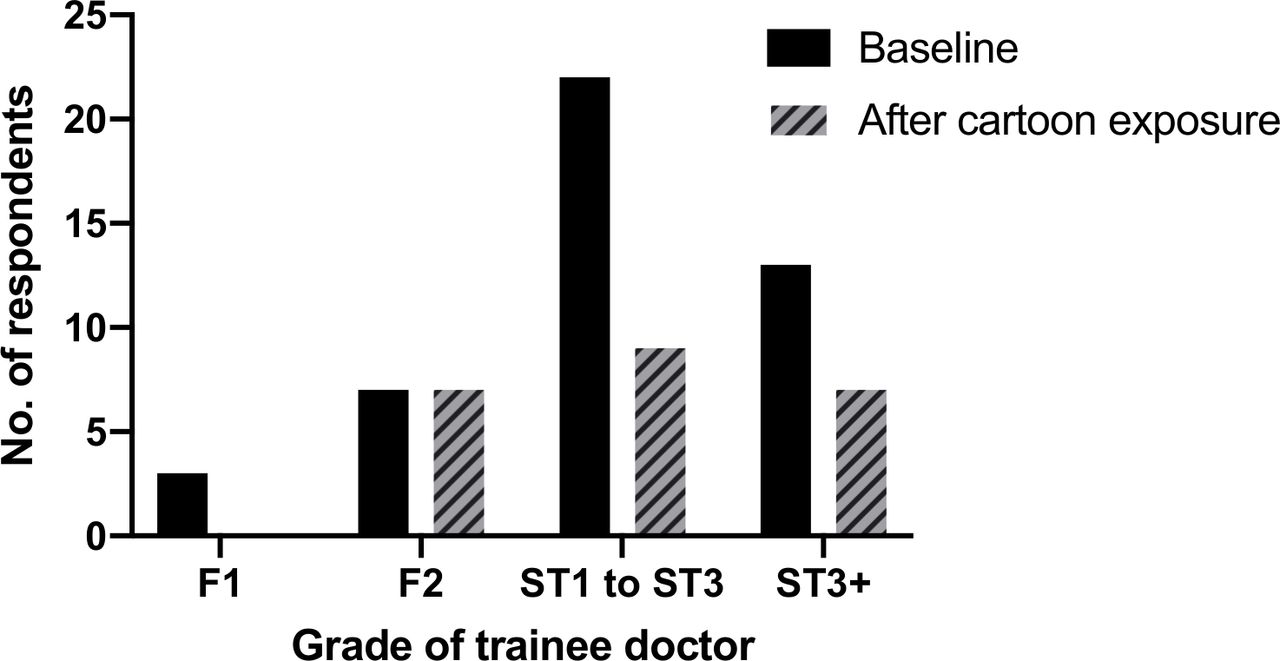
There were 45 responses from the baseline survey and 23 responses from the radiation awareness survey after the doctors in training were exposed to the educational cartoon (figure 1).
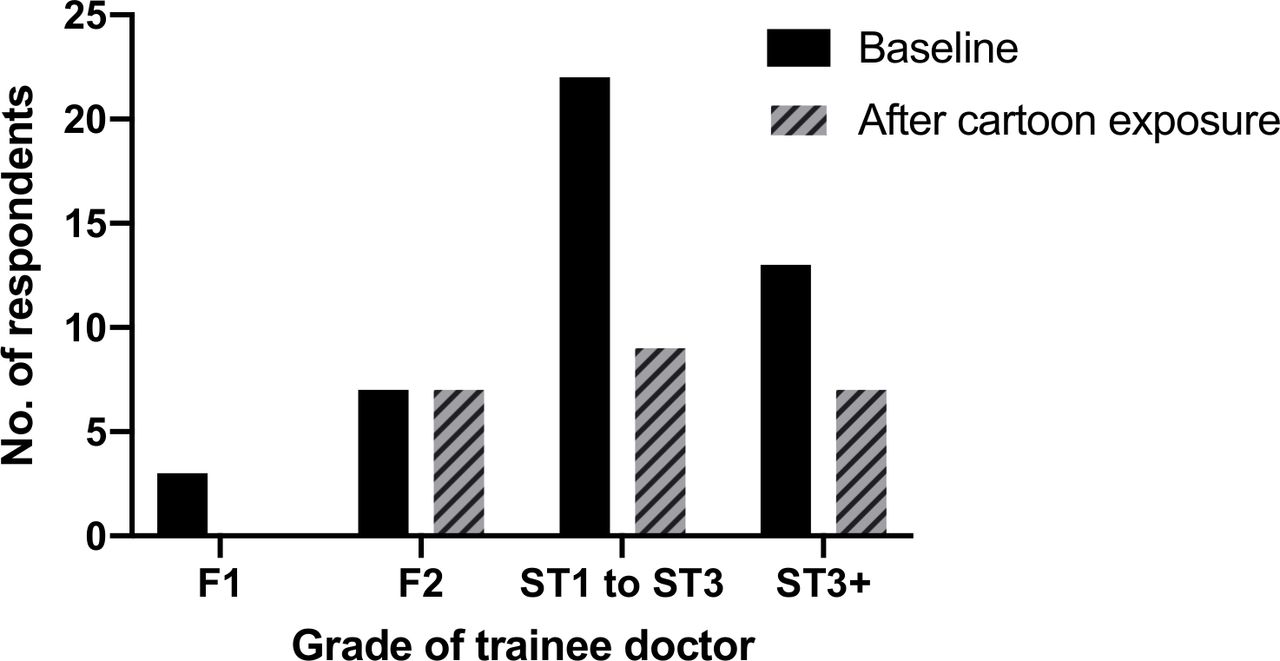
Grade of trainee doctor who responded to baseline and follow-up surveys.
At baseline, 20% (n=9) of respondents had received formal training on radiation safety with regard to diagnostic investigations at medical school, 24% (n=11) after medical school and 56% (n=25) had received no such training at all (figure 2). After induction training, the number of respondents who considered that they had received no formal training in radiation awareness had decreased to 26% (n=6) (p=0.02, χ2 test).

Previous experience and location of place of formal training on radiation safety with regard to diagnostic investigations.
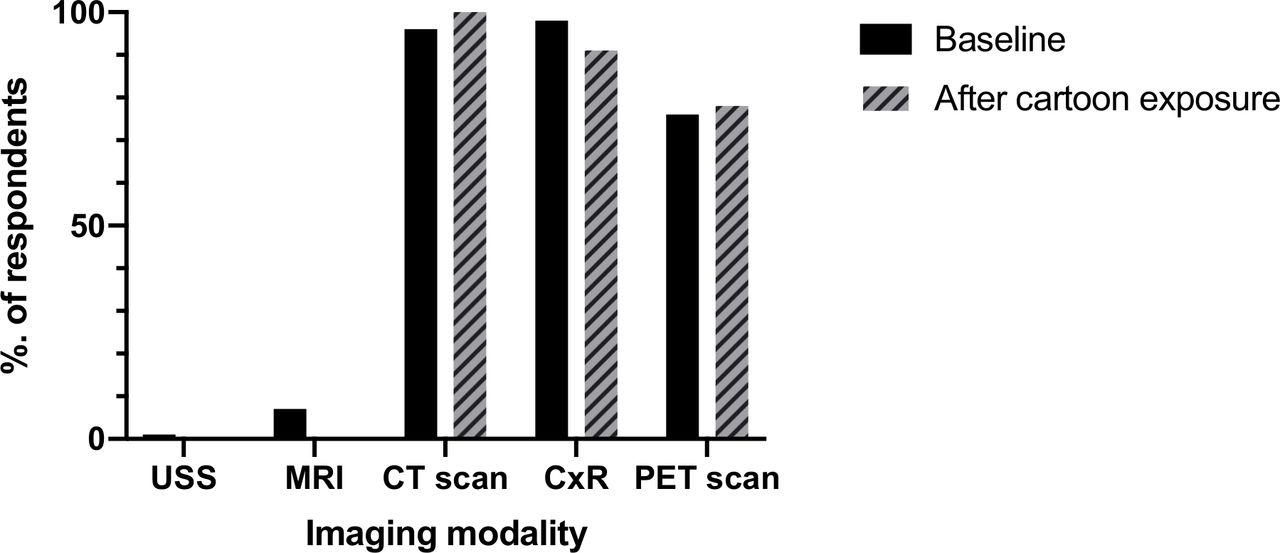
At baseline, 96% (n=43) of respondents were aware that a CT scan involved ionising radiation, and this had increased to 100% (n=23) 1 month after induction training (figure 3). At baseline, 60% (n=27) of respondents considered that young females were at the highest risk of developing long-term complications after exposure to ionising radiation, while 33% (n=15) considered that the risk of ionising radiation was equal across different ages and sexes (figure 4). After the induction training, these percentages had changed to 87% (n=20) and 13% (n=3), respectively (p=0.06, χ2 test).
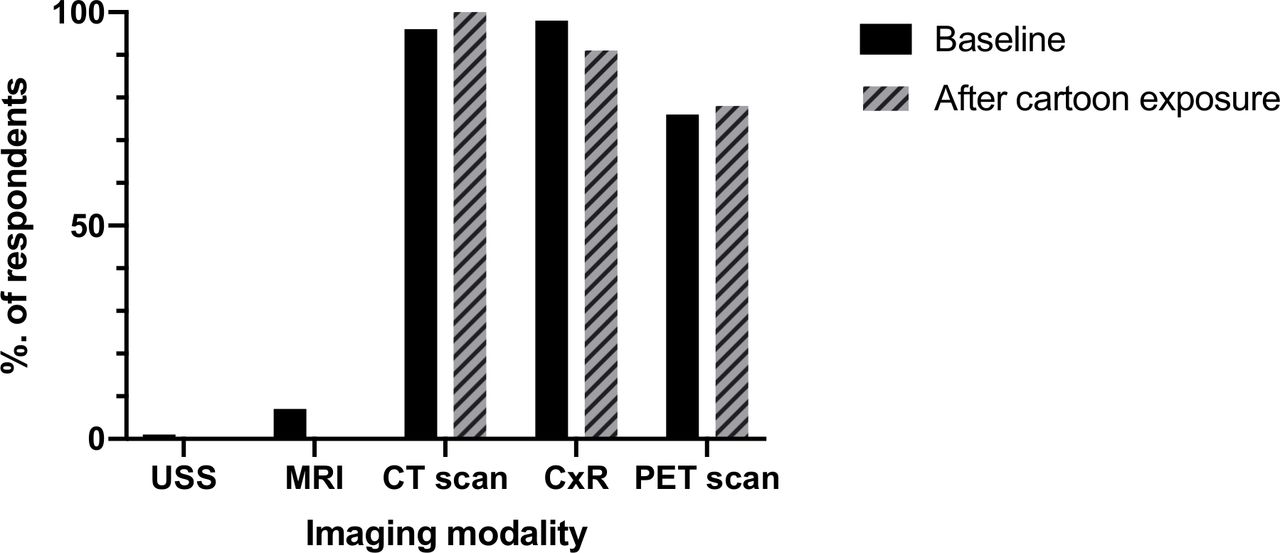
Response to the question ‘which of these imaging modalities involve ionising radiation*?’ *Correct answers are CT scan, chest X-ray (CxR), positron emission tomography (PET) scan.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Response to the question ‘which group is a highest risk of developing long-term complications after exposure to ionising radiation?*’ *Correct answer is ‘young females’.
Discussion
A novel short educational tool has been developed to address a clear educational need for clinicians to become more aware of the long-term health impacts of the ionising radiation delivered by routine diagnostic imaging techniques. These pilot data suggest that this is associated with an increase in self-reported formal training in radiation awareness, and increased awareness of the higher susceptibility of younger females to long-term complications as a consequence of ionising radiation. These data suggest that the use of a cartoon whiteboard is feasible in delivering medical education and has potential in communicating important patient safety messages to clinicians.
The unique strength of this approach is that the educational cartoon represents a new approach to educating doctors in training, which complements more traditional teaching practice. The content was generated by local concern about high use of CT scans in acute medicine which is likely to be relevant in other secondary care centres. The cartoon is relatively short at 7 min, 10 s which allows it to be incorporated into a very busy induction programme for new doctors. The internet-based format means that it can be disseminated at no additional cost, and hence could be used to reach other audiences other than doctors in training. It is likely that these media could have utility in other areas of medical education, where there is a simple important message that can be encapsulated into a short cartoon. The prominent use of local clinicians in cartoon format along with familiar surroundings provides a novel spectacle that may keep the viewers’ attention, simply because they are familiar with the individual and working environment. This technique underpins many communication strategies used to develop brands and modify consumer choice.8
One limitation of our data collection methodology is that doctors-in-training induction in the UK are not attended by all eligible individuals, as some may be currently working or doing night-shifts during that time period to ensure that the clinical services are delivered. An opportunistic form of data collection was used with the before and after email surveys, which allowed data to be collected efficiently. This is a variant of ‘convenience sampling’, where data are collected from the available population. While not as methodologically rigorous as randomly selected sampling, it has a role in epidemiology as long as the limitations are acknowledged, particularly the concerns about bias and generalisability.9 Thus, we contacted all individuals who were eligible to attend the induction day, but do not confidently know how many people attended and stayed for the whole of the induction event, and hence how many people actually saw the radiation harm educational cartoon. Future evaluations may involve more complete data collection on the day of the induction from larger populations, which would establish a firm baseline cohort for the population of those who have seen the educational cartoon, and hence permit calculation of response rates and hence assessment of potential bias and generalisability of the data with confidence, as well as permitting subgroup analysis by medical specialty and experience. Although the definitive study would study the impact of the educational cartoon on clinician use of diagnostic tests, this would be methodologically challenging and hence subsequent studies in this area will probably also consider more proximal outcome measures related to clinician awareness of the risk of ionising radiation.
The interval of approximately 6 weeks between the two surveys was selected pragmatically as a period of time over which medium-term memory and learning may be observed. Future studies of this topic could collect data on radiation awareness more than once to determine the temporal associations between exposure to the educational cartoon and awareness of ionising radiation, and retention of this knowledge. However, one role of a doctor-in-training is to accrue clinical experience, and the longer the interval between baseline data collection and final data collection, the higher the risk that other factors may confound the associations observed.
Nonetheless, the survey responses suggest that exposure to the radiation harm cartoon is associated with increased formal training in radiation awareness, and an increase in which subgroups of the total patient population are more at risk after exposure to ionising radiation. These are important preliminary observations, as the baseline data demonstrate that 56% of our population of doctors training had received no formal training in radiation awareness at all. This is reflected in the two individuals who had the capacity to request CT scans who were not aware that they delivered an ionising radiation dose to patients, although after exposure to the radiation harm cartoon, all respondents were aware of this important fact. We have previously surveyed all doctors in the same hospital in 2018, and, of this population, 35% reported no formal training on the risks of exposure to ionising radiation.5 As the current population consisted of relatively younger doctors compared with the previous survey, the higher prevalence of no radiation training may be a consequence of their shorter working career and hence less opportunities.
While these data are from a relatively small, pilot study, they demonstrate a clear unmet need for more education of doctors on the long-term harms of ionising radiation. As these consequences include malignancy1 and cataracts,2 they are not trivial, and as there were 4.8 million CT scans in England in 2017 with an increase in activity of 7.9% per annum,10 this constitutes an important public health issue. Addressing this matter is likely to involve a variety of interventional approaches that use both established conventional teaching methodologies supported by opportunistic communication strategies,11 and will require continual medical education from medical school onwards. Our data have demonstrated the feasibility of using short educational cartoons to increase awareness of ionising radiation among doctors-in-training. This is simply the first stage in a process that will require evaluation of where this approach may be used optimally in medical education. We speculate that for patient safety messages that aim to minimise harm in particular, the educational cartoon may complement rather than replace existing educational strategies, as the same message efficiently delivered in different ways may ultimately have a larger cumulative impact.
While the use of a short radiation harm educational cartoon led by recognisable local doctors that aims to increase clinicians’ awareness of the long-term risks associated with ionising radiation exposure will not rectify the situation alone, it does provide a cheap, scalable tool that can be used to reinforce the message that exposing patients to ionising radiation results in a small long-term increase of adverse health consequences. The advertising industry uses these approaches because they work.12 In areas that aim to improve patient safety, health services research can learn novel communication strategies from other disciplines to improve patient care. This is particularly pertinent in the context of the COVID-19 pandemic, where traditional medical meetings are challenging due to the necessity for social distancing, yet the efficient communication and awareness of patient safety information remains of paramount importance.
Acknowledgments
The authors would like to thank Nigel Sturrock, Mark Norwood, Dominick Shaw, Tessa Langley, Jo Cranwell, Sarah Lewis for helping deliver the work that preceded this project. The authors would also like to thank Navrose Chappell for helping distribute the survey.
Footnotes
Contributors The original concept was conceived by AF, RS and BY. The educational cartoon was designed by AF, PT, RB, RS and RL. The questionnaire was designed by BY and AF, and the data were collected by IB. The first draft of the manuscript and statistical analysis was by AF. All authors contributed to and approved the final draft of the manuscript.
Funding This work was funded by a Behavioural Insights project grant from the Health Foundation.
Disclaimer The funder had no role in the study and collection, analysis and interpretation of data and in writing the manuscript.
Competing interests This work was funded by a grant from the Health Foundation to the University of Nottingham. Both mediafortheweb.com and russlaw.co.uk received payment for services provided.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval The study was designed as an evaluation of a health services intervention. As a consequence, no ethics approval was required. The waiving of the need for Ethics Committee in this context complies with national guidelines described in Governance Arrangements for Research Ethics Committees (Department of Health and Social Care. Governance arrnagements for research ethics committees, 2011 [Accessed 12 Nov 2019]).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.