Article Text

Abstract
Background Depression, which is a serious medical illness, is prevalent worldwide and it negatively impacts the adolescent lifestyle. Adolescent depression is associated with adverse emotional and functional outcomes and suboptimal physical health. Over the last decade, it has been found that approximately 9% of teenagers meet the criteria for depression at any given time, and one in five teenagers have a history of depression during adolescence. Ninety per cent of paediatricians believe that recognition of child and adolescent depression is their responsibility; however, it has been reported that 46% lacked confidence that they could recognise depression.
Methods In this study, adolescents between 12 and 17 years of age were screened during their well-child visits using the Patient Health Questionnaire Modified for Adolescents. A score of 10 or higher warrants a referral to a social worker and psychiatrist. The goals of this quality improvement project were to implement a standardised questionnaire and to improve the screening, diagnosis and treatment of depression in children from 12 to 17 years of age.
Results It was found that the adolescent depression screening rate significantly improved within 6 months of implementing this quality improvement project. The screening rate improved to 50% by mid-cycle (Plan-Do-Study-Act (PDSA) cycle 3) and up to 70% at the end of the 6-month period (PDSA cycle 5). Improvement was noted among all providers, across all age groups, and in both male and female patients by the end of the study period.
Conclusion Standardised screening tests with a scoring system help providers to identify and monitor depression symptoms using a common language, especially in the outpatient clinical setting where the patient may be seen by different providers.
- quality improvement
- mental health
- PDSA
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Depression is a serious medical illness that is prevalent worldwide, and it negatively impacts the adolescent lifestyle. Major depressive disorder is defined as depressed mood (eg, feels sad, empty or hopeless) or loss of interest that is associated with at least four of the nine other symptoms that reflect a change in functioning, such as problems with appetite, energy, concentration, disturbed sleep–wake cycles, and self-image that last for a period of 2 weeks or more.1 Adolescent depression is associated with adverse emotional and functional outcomes and suboptimal physical health.
According to studies from the last decade, approximately 9% of teenagers meet the criteria for depression at any given time, and one in five teenagers have a history of depression during adolescence.2–6 Another study conducted in 2006 showed that the lifetime prevalence of depression in the adolescent population was 13%.7 Changes in the social environment and puberty, along with cognitive maturation, may lead to the increased prevalence of depression among teenagers.8
In 2009, the US Preventive Services Task Force (USPSTF) noted that screening tools for depression can help to identify depression.9 Such screening tools include the Patient Health Questionnaire Modified for Adolescents (PHQ-A) and the primary care version of the Beck Depression Inventory (BDI). Adolescent depression may be undiagnosed if appropriate screening at periodic intervals is not performed by the primary care doctor/paediatrician. The Bright Futures/American Academy of Paediatrics recommends yearly screening of child and adolescent patients aged 12–18 years for emotional and behavioural problems.10
Another study showed that implementing PHQ-A in a paediatric primary care setting led to increased diagnosis of depression among adolescents.11 Major depressive disorder has short-term effects that include poor school performance, suboptimal growth and development, behavioural changes and impairment in normal interaction with family members and peers. Some of the long-term consequences include poor education rates that lead to low socioeconomic status, aggressive behaviour, the diagnosis of depression and anxiety in adulthood, increased risk for self-injurious behaviour and suicidal ideation.
A study conducted in 2001 in New Hampshire, USA, reported that 90% of paediatricians believe that recognition of child and adolescent depression is their responsibility; however, 46% lacked confidence that they could recognise depression.12 Therefore, the goal of this quality improvement (QI) project was to implement a standardised questionnaire to improve screening for depression by 60% in adolescents from 12 to 17 years of age.
Materials and methods
The study was formally reviewed and deemed exempt from further review according to the Institutional Review Board at Monmouth Medical Center. This study was conducted in a Federally Qualified Health Centre wherein more than 50% of the patients have Medicaid as their insurance provider and over 20% pay out of pocket. The study aimed to include all adolescents between 12 and 17 years of age who presented for a well-child visit. Children younger than 12 years old and adolescents coming for a visit due to illness were not included as screening for depression is not recommended in that age group. Patients aged 18 years or older were not included in the study as they are typically seen by internal medicine residents. Additionally, adolescents coming for a visit due to illness were not included. The PHQ-A was used as the depression screening tool. A score of 10 or higher13 would warrant a referral to a social worker and psychiatrist. PHQ-A has a sensitivity of 73% for a positive test and specificity of 94%.14
Adolescent well visit appointments from age 12 to 17 years who presented to the FQHC were retrospectively analysed via electronic medical record. The list of patients was generated by final diagnosis code Z00.129 in the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). All patients were usually seen by a resident physician and precepted by an attending physician. Demographic data of patients including age, gender, race and language spoken were studied. The baseline data regarding the percentage of patients screened and percentage of referrals to mental health services for a well visit 1 month prior to the implementation phase (Plan-Do-Study-Act (PDSA) cycle) of the study were obtained.
A fishbone (Ishikawa) diagram (figure 1) of the possible challenges to the implementation of the PHQ-A was created. Five PDSA cycles were performed and the project leaders (MM and DK) met to determine strategies to improve the screening rates. The primary outcome of this study was to implement the PHQ-A to improve screening for depression among adolescents in a Federally Qualified Health Centre. Observing the rate of referral to mental health specialists and a social worker was the secondary outcome of this QI project.
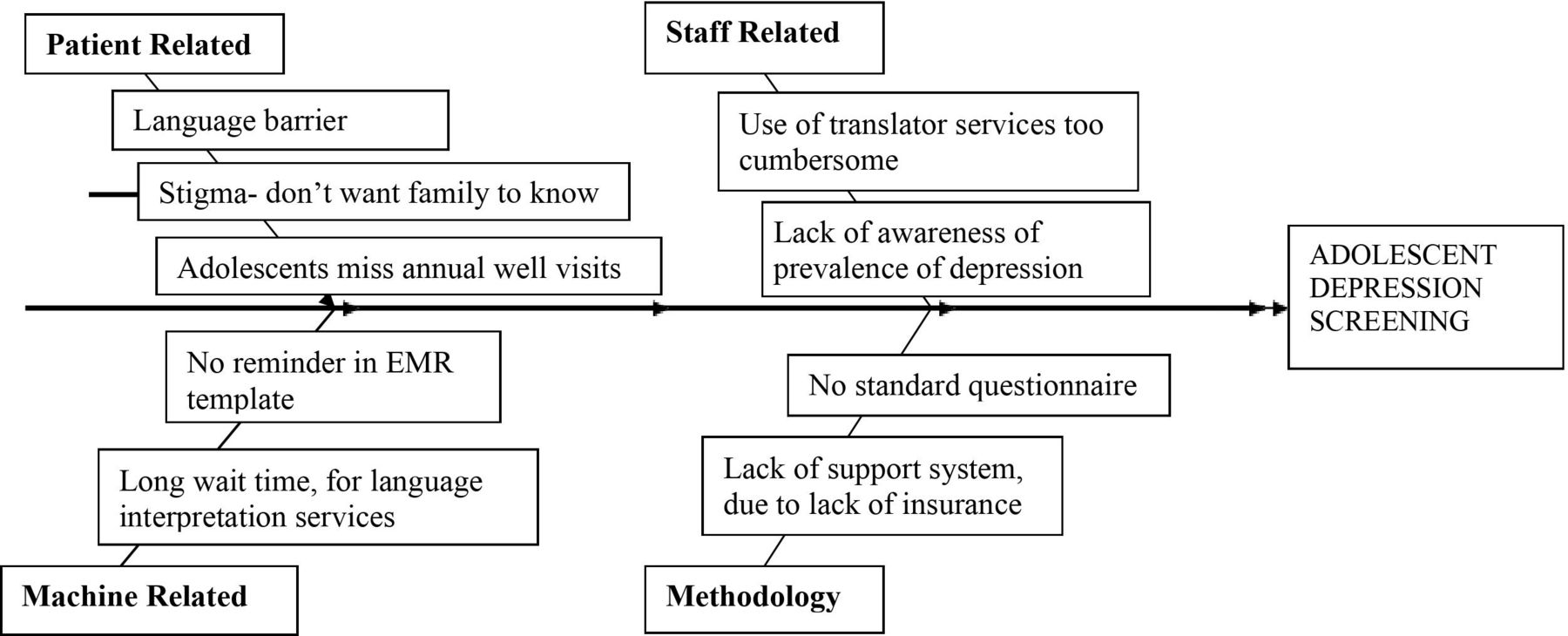
Fishbone (Ishikawa) diagram depicting challenges to the implementation of the Patient Health Questionnaire Modified for Adolescents.
In this QI project, we used the PHQ-A as it is readily available, easy to download in multiple languages and free of cost. As the PHQ-A also has fewer questions than the BDI, it easier for the patients to answer and is less time-consuming for the medical staff.
During our study, we followed the Institute of Healthcare Improvement’s model for QI projects; that is, the PDSA cycles.
Results
The adolescent depression screening rate significantly improved within 6 months of implementing this QI project. After the intervention, we reviewed a total of 109 well-child visit charts of the adolescents (12–17 years) between February 2017 and June 2017 through five PDSA cycles. The demographics for the study population (table 1) showed that the mean age was 14.74±1.65 years (range 12–17 years), and that it included 59 boys and 50 girls. Fifty per cent of the adolescent females who present to our clinic for well visit were screened for depression; 53% of the males in this population were screened for depression. The ethnicity of the population was varied, including adolescents who were African–American (8), Native American (1), Asian (1), Caucasian (17), Hispanic (77) and other (5).
Demographics of the study population
The baseline data showed that no standardised screening tool was used and the referral rate to mental health services was 0% as the symptoms of depression were not identified.
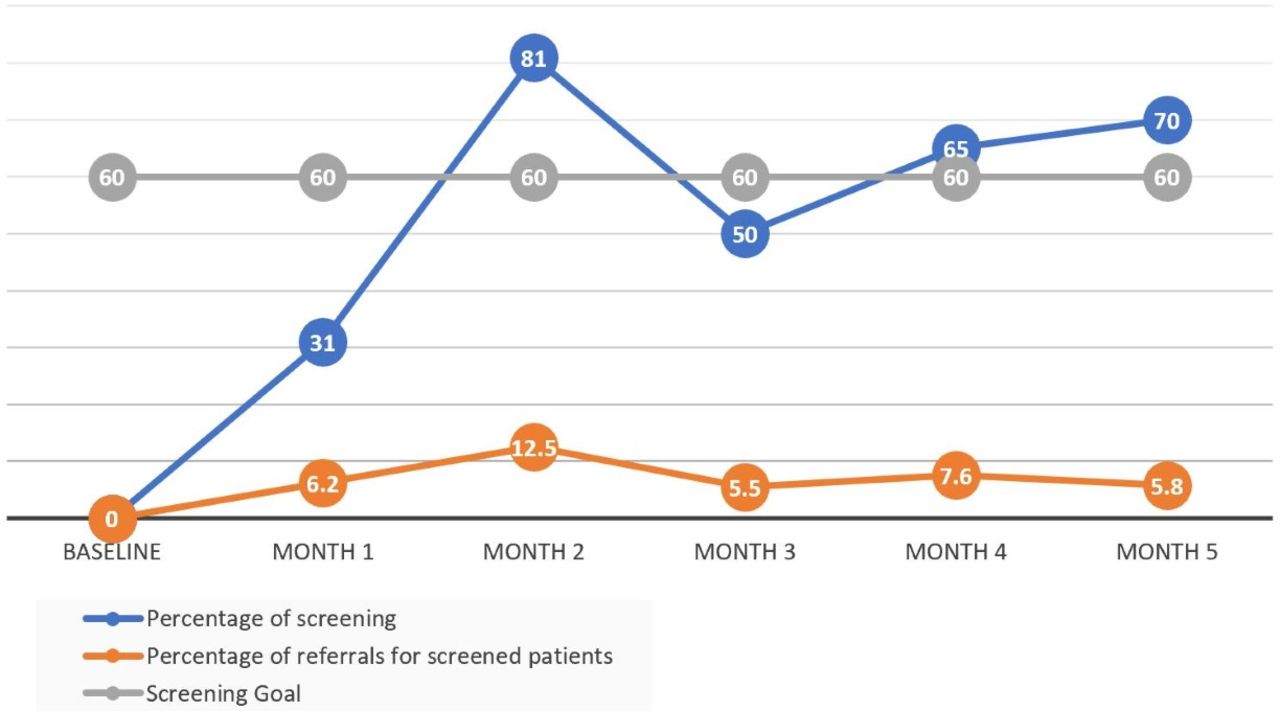
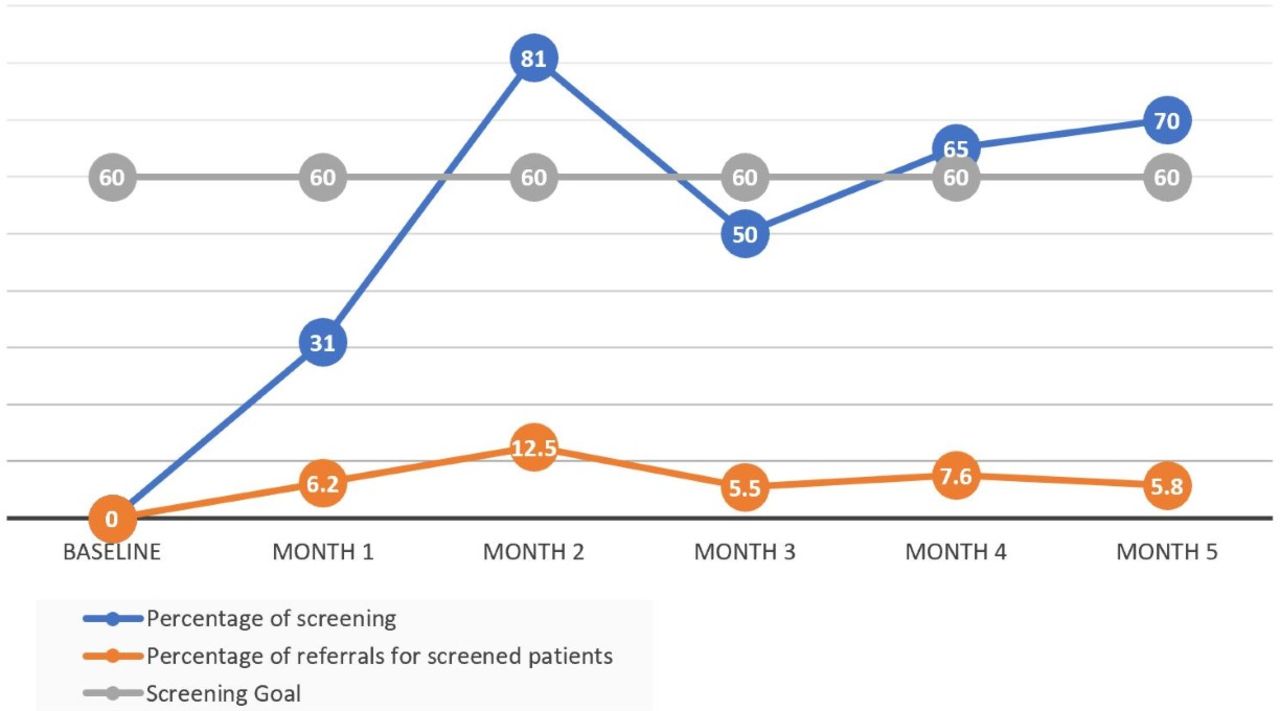
By the end of the study period, screening rate had increased to 70% (figure 2). The overall rate of referral to mental health services had also increased to 5.8% (figure 2). The patients who scored 10 or higher on the questionnaire had a 100% referral rate to social and mental health services.
{kind=link}
{kind=link}
Screening and referrals for depression in adolescents.
PDSA cycle 1
An email was sent to the residents with the instructions for using the screening tool. The method of calculating the scores, and the cut-off values for referral, were outlined. After this cycle, screening rate was 31%.
Plan: Start educating residents on using depression screening tool using email and assess the response. Electronic communication via electronic mail (email) was noted to be effective with all residency/research-related communication in the past with other studies in our institute. Residents were also able to refer to the existing email if needed.
Do: Sending emails to residents with instructions on how to use the depression screening questionnaire.
Study: Depression screening rate increased from 0% to 31%. Ten patients out of the 32 adolescent patients who presented for a well visit were screened for depression using the PHQ-A tool.
Act: It was clear that we were moving in the right direction, however, new interventions were needed, and we started PDSA 2.
PDSA cycle 2
We determined that lack of resident education about the problem was a possible cause of poor adherence. To improve this, Microsoft PowerPoint was used to create educational lectures regarding depression screening, and the need for implementing the PHQ-A was highlighted. Literature supporting the use of a standardised tool was reviewed during the presentation. In addition, after analysing the data of cycle 1, it was found that some patients could not be referred to psychiatry due to lack of insurance. With the assistance of a social worker, resources were identified and information about psychiatrists who accept uninsured patients was included in the educational lectures. After this cycle, screening rate was 81%.
Plan: Increase screening by increasing residents’ education not only about how to use the questionnaire, but also about why we use it. Physicians and residents are analytical thinkers at baseline. Education regarding the use of questionnaire, the importance of screening for process, lack of adequate screening added to value to the importance of tackling the inadequate screening process. Also, it was noticed that some patients were not able to see a psychiatrist because of lack of insurance.
Do: PowerPoint presentation discussing prevalence of depression and the social and emotional impact it has on children and that residents are in a position to help in early diagnosis of depression among adolescents by using the depression screening questionnaire. Thirteen out of the 16 paediatric residents attended this lecture. We also worked on helping patients who did not have insurance by connecting them with the social worker and providing information about psychiatrists who accept uninsured patients.
Study: Screening rate increased from 31% to 81%. During the second PDSA cycle, 13 out of the 16 adolescent patients were screened for depression during their well visit.
Act: Although screening and referral rates were increasing, we noticed that the depression questionnaire was available in the clinic only in English and Spanish. We worked on addressing this problem in PDSA 3.
PDSA cycle 3
A meeting was conducted, and residents were asked to express their opinions and concerns regarding the use of the PHQ-A screening tool. Initially, copies of the questionnaire were given only in English and Spanish; however, there were concerns that some patients spoke Portuguese, Vietnamese or Creole, which prevented the use of the screening tool. As a result, copies of the questionnaire were provided in all these languages, and a link to a website where the questionnaire can be downloaded was given to each resident physician. After this cycle, screening rate was 50%.
Plan: Feedback from residents regarding their concerns and opinion helped us improve our subsequent PDSA cycles as we started providing depression screening questionnaires in multiple languages.
Do: Print screening questionnaires in English, Spanish and Portuguese, as well as provide the web address to download the questionnaire in more languages if needed.
Study: Screening rate dropped from 81% to 50%. Nine of 18 adolescents were screened for depression. We found that a specific group of patients who were self-pay was missed and not screened during the well visit.
Act: Identify the patients that needed to be screened through PDSA 4.
PDSA cycle 4
A significant number of patients were missed, we printed the list of patients that each resident has every day and manually marked the patients who are registered for a well-child visit who are 12–17 years old. This served as a reminder to perform the screening. After this cycle, screening rate was 65%.
Plan: Highlighting patients between 12 and 17 years of age on the printed patient schedule for each resident daily was a visual reminder for adolescents to be screened for depression. Identify patients that need to be screened to increase screening rate.
Do: Print the patient list for each resident and mark the patients 12–17 years of age who have a well visit that day.
Study: Screening rate increased from 50% to 65%. Seventeen out of the 26 adolescent patients were screened for depression.
Act: Rates were improving, and we were looking at keeping the screening going and we started the last cycle PDSA 5.
PDSA cycle 5
The results of the previous four cycles were shared with other residents via email to provide positive feedback and reinforcement and to promote the idea that providing quality patient care involves team work and that the contribution of every member of the team is necessary. After this cycle, screening rate was 70%.
Plan: Continue depression screening practices by showing the residents the impact of the screening tool they use. We thought that sharing the screening percentage (including the graph) which showed the incremental improvement may aid to motivate the residents to continue their screening during well visits.
Do: Share results of the previous four PDSA cycles and showing the increased rate of diagnosis of depression cases that could have been missed without using the screening tool. Using standardised depression screening tools help identify patients with depressive symptoms that could have otherwise been missed.
Study: Screening rate increased to 70%. Twelve of 17 patients were screened for depression during their well-child visit.
Act: Residents were encouraged to continue using the screening tool even after the conclusion of the QI study.
Discussion
Our baseline data showed that no systematic screening tool was used for screening adolescents for depression. The USPSTF makes recommendations about the effectiveness of specific preventive care services for patients without related signs or symptoms of depression.14 Many of these patients are at higher risk for depression as they have additional stressors, including low socioeconomic status, recent immigration, limited English proficiency, lack of access to subspecialty care due to lack of insurance, and sometimes one or both parents are in their home county and the patient is taken care of by another family member.
The National Institute of Mental Health reports that, in 2016, the prevalence of major depressive episode ranged from 19.4% among adolescent females to 6.4% in males,15 which is close to the data in our study that showed that the percentage of adolescents who scored high on the PHQ-A ranged from 5% to 12%. In another study done from January 2017 to August 2018 including 2107 adolescents, the percentage of positive screening was 11%.16
We found improvement in the screening rates and documentation rates along with an increase in the rate of referral to mental health services. The screening rate improved to 50% by mid-cycle (PDSA cycle 3), and up to 70% at the end of the 5-month period (PDSA cycle 5). There was an initial good spike in screening to 81% after two PDSA cycles. However, this dropped by 31%, and screening rate was half of the entire adolescent population mid-cycle. The initial spike is likely to have been due to the Hawthorne effect, and the initial increase in screening was due to the residents’ excitement about the project that gradually waned over time. Residents needed to be re-engaged through monthly meetings, and although the screening rates have increased, we were not able to reach 80% again. A similar study done in a rural clinic in South Carolina showed a compliance rate of 88% for administering depression screen in the adolescent population.11 A study done in Michigan showed screening rate of 82%. Researchers were able to integrate the depression screening questionnaire into the clinic’s EHR which made the screening process easier and also served as a reminder for the physicians.17 We recognised that having the questionnaire built into the visit’s template in the EHR would increase the screening rate. However, after consulting IT department, we were not able to have the questionnaire added to the clinic’s EHR. Another contributing factor for the decline in screening rates was availability of the PHQ-A only in English and Spanish. Residents were educated regarding online access for other languages and were provided with the website link which resulted in better compliance.
Other potential challenges were identified and represented in the fishbone diagram. One of the challenges was to arrange mental health services for those who score high on the screening test but have no insurance. Prior studies on screening adolescent for depression did not mention this particular challenge wherein a subset of patients without insurance had difficulty to obtain mental healthcare services/follow-up. Fortunately, in our FQHC with the help of the clinic’s physicians and social worker, we were able to arrange such services, even for patients with other mental health diseases.
This study shows that screening in primary care can help physicians to identify patients. Initiation of appropriate mental health treatment may in turn improve the quality of life of patients. This was evident from a Cochrane review done in the UK which showed significant improvement of short-term and long-term outcomes in adults with depression.18
Limitations
One of the limitations of this study is the use of a single centre study with a relatively small sample size.
Another limitation of this study was our inability to add a reminder prompt into the well-child visit template. As a result, the screening was missed during some of the visits in the teenage population. A gap in the systematic follow-up of the patients, after referral to psychiatric facilities, was noted. Although the follow-up may have been performed by the clinic’s physicians, reviewing it was not in the scope of the study. Referral rates to psychiatry are not equivalent to cases diagnosed with depression since some patients would have had a false-positive screening test. However, a limitation of this study is the lack of follow-up with psychiatry offices to see the percentage of patients diagnosed with depression in relation to the total number of patients screened.
Future initiatives
Currently, depression screening for adolescents has been included as a part of the well-child visits in the clinic. The screening process is under direct supervision of the attending physician supervising the residents who ensures administration of the questionnaire as well as training new residents on using it. There will be another PDSA cycle conducted 12 months later to assess ongoing compliance and to examine the rates of admission to the hospital’s inpatient psychiatric unit with depressive symptoms before and after implementation of the screening using the PHQ-A. We will look at the admission rates for the patients who received their routine medical care at our clinic.
We also hope to be able to do a multicentre study involving multiple outpatient clinics.
Conclusion
Improvement in screening for depression among adolescents using a standardised and validated screening tool led to improvement in the rate of referral to mental health services. Standardised screening tests with a scoring system help providers to identify and monitor depression symptoms using a common language, especially in the outpatient clinical setting where the patient may be seen by different providers. This study also showed that, during the preparation of QI projects, potential challenges can lead to solutions that can then benefit the study population even after the project is over. In this QI project, we were able to arrange mental health services for uninsured or underinsured patients and these patients continued to use these services for other mental health problems that were not related to depression. This project is an example of a combination of child advocacy, practice-based learning and system-based practice.
Acknowledgments
The authors acknowledge the IT team at Monmouth Family Health Center for their support in this project.
References
Footnotes
Contributors MM designed the study, did substantial work in the analysis and interpretation of the data, revised the work, approved the final version to be published and agreed to be accountable for all aspects of the work. DK did substantial work in the analysis and interpretation of the data, revised the work, approved the final version to be published and agreed to be accountable for all aspects of the work. JL designed the study, did substantial work in the analysis and interpretation of the data, revised the work, approved the final version to be published and agreed to be accountable for all aspects of the work. JT did substantial work in the analysis and interpretation of the data, revised the work, approved the final version to be published and agreed to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to this study are included in the article.