Article Text

Abstract
Introduction Effective implementation of standard precautions specific to COVID-19 is a challenge for hospitals within the existing constraints of time and resources.
Aim To rapidly design and operationalise personal protective equipment (PPE) donning and doffing areas required for a COVID-19 care facility.
Methods Literature review was done to identify all issues pertaining to donning and doffing in terms of Donabedian’s structure, process and outcome. Training on donning and doffing was given to hospital staff. Donning and doffing mock drills were held. 5S was used as a tool to set up donning and doffing areas. Instances of donning and doffing were observed for protocol deviations and errors. Plan–do–study–act cycles were conducted every alternate day for 4 weeks. The initiative was reported using Standards for QUality Improvement Reporting Excellence (SQUIRE) guidelines.
Results Best practices in donning and doffing were described. Our study recommends a minimum area of 16 m2 each for donning and doffing rooms. Verbally assisted doffing was found most useful than visual prompts.
Discussion Challenges included sustaining the structure and process of donning and doffing, varied supplies of PPE which altered sequencing of donning and/or doffing, and training non-healthcare workers such as plumbers, electricians and drivers who were required during emergencies in the facility.
Conclusion Our study used evidence-based literature and quality improvement (QI) tools to design and operationalise donning and doffing areas with focus on people, task and environment. Our QI will enable healthcare facilities to rapidly prototype donning and doffing areas in a systematic way.
- checklists
- continuous quality improvement
- healthcare quality improvement
- infection control
- PDSA
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Personal protective equipment (PPE) use in healthcare involves three phases: donning, while providing patient care, and doffing. Issues during any of these phases can lead to a risk of contamination to the healthcare worker (HCW).1 Incorrect technique or sequence in donning can expose HCWs during patient care or sets HCW up for a doffing failure.2 Contamination of HCWs can occur during patient care if PPE is damaged, has design flaws or if HCWs circumvent protection. Risks of contamination during doffing can be due to an incorrect removal technique, improper handling and disposal of PPE, or by damaging PPE to expose HCWs.1–6
HCWs endure extreme heat, long periods of standing during patient care and then remove PPE, which requires patience, attention and some unusual movements. Doffing is a physically rigorous task that demands flexibility, balance and constant vigilance.7 It is a high-risk process8 that requires a structured procedure and a designated area for removal to ensure protection.9 However, deviations from recommended doffing protocol are common with self-contamination rates ranging from 13% to 90%.1–6 Quantitatively, the amount of self-contamination that is clinically meaningful to transmit SARS-CoV-2 during doffing is not yet known. However, SARS-CoV-2 contamination of common objects in the intensive care unit (ICU) and wards, virus aerosolisation in a confined space or spread from asymptomatic infected persons is documented, implying a potentially high infection risk for medical staff and other close contacts even though the amount of viable virus could not be determined.10 11 Comparatively, despite wearing PPE, 1 in 10 HCWs contracted Ebola during the epidemic.12–14 Routine breaches in PPE use do not generally result in highly visible disease outbreaks but may contribute to ongoing transmission of nosocomial infection.4
Studies describing the layout and design for doffing rooms specific to Clostridium difficile and Ebola virus have established that the space and design of built environment for donning and doffing improves HCW safety, influences compliance and has a measurable impact on HCW contamination risk while doffing PPE.15–18 The coronavirus is not transmitted in the same way and it is not clear if these recommendations translate to COVID-19. Also, literature is limited on the ideal size for a donning and doffing room and managerial issues of donning and doffing areas.
The aim of our quality improvement (QI) initiative was to rapidly set up PPE donning and doffing areas in a hospital. The objectives were to define the structure (size, layout and design) of an ideal donning and doffing room, identify the process issues pertaining to donning and doffing and take systemic measures to improve the same.
Methods
The initiative was undertaken at an acute cancer hospital that was converted into a COVID-19 care facility with 400 isolation rooms, 400 beds in wards and 25 beds in ICU. Care was provided to more than 2358 patients for 12 weeks out of which more than 90% had mild to moderate symptoms. A rapid QI event was conducted for 6 weeks. The team comprised hospital administrators, infection preventionists, and supervisors of nursing assistants and environmental service personnel. Inputs were taken from infectious disease specialists as well as the apprehensions, suggestions, comments and feedback of resident doctors throughout.
Our initial literature review identified all issues pertaining to donning and doffing in terms of Donabedian’s structure, process and outcome.19 This was used as a tool to strategise planning and training. Training of trainers was done who later trained HCWs in small groups every day. Physical distancing was maintained between participants during group trainings. Initial training in PPE was done with a commercial PPE ensemble that comprised an impermeable surgical gown, a hood cap, a pair of goggles and a pair each of gloves, arm guards and knee-length impermeable leggings. Ankle-length shoe covers, another pair of gloves, one face shield and one N95 respirator were added separately to complete the full-body PPE. The hospital provided surgical scrubs and slippers to HCWs before donning PPE. Personal clothing was not advised.
The tool, 5S,20 was used to set up and sustain the structure and process of donning and doffing areas. This tool addresses planning in a structured way: sort, set in order, shine, standardise and sustain. Plan–do–study–act (PDSA) cycles were done to further improvise the structure and process of the areas. The PDSA is a cycle of planning goals and measuring progress during implementation, studying results through careful analysis, and enacting needed changes rapidly to ensure ongoing improvement and assess impact.21
Results
Based on literature review, we identified the best practices related to donning and doffing (box 1).
Best practices related to donning and doffing3 15 16 28–31
Dedicated room each for donning and doffing.
The doffing area has a unidirectional flow from contaminated to cleaner areas to the outside in a continuous forward motion.
The floor demarcation indicates the contaminated areas and clean areas.
Designated location of key items such as the trash can and chemical mat.
The size of the doffing area should ensure that all items are always within arm’s reach of the healthcare worker (HCW).
Placing mirrors to assist during shoe cover removal, improve posture and enable self-inspection.
The HCW is adequately trained regarding proper location and orientation when doffing.
The HCW is acquainted with available personal protective equipment in advance before donning in practice.
Defined space to reduce risky behaviours among HCWs.
Presence of large observational windows to observe the doffing personnel.
Ensuring good visual and voice contact between the doffing personnel and the observer.
Minimum 10 air changes per hour for airborne infectious isolation room for doffing.
The HCW should be able to extend the arms, bend at the wrist and go through a range of motions sufficient for patient care delivery while all remaining correctly covered.
The height and width of the sink must be at a good working level of HCWs to prevent self-contamination during handwashing.
Visual cues to enhance provider safety.
The height of the alcohol-based hand rub dispenser should be mounted at a height of 106–114 cm from the floor.
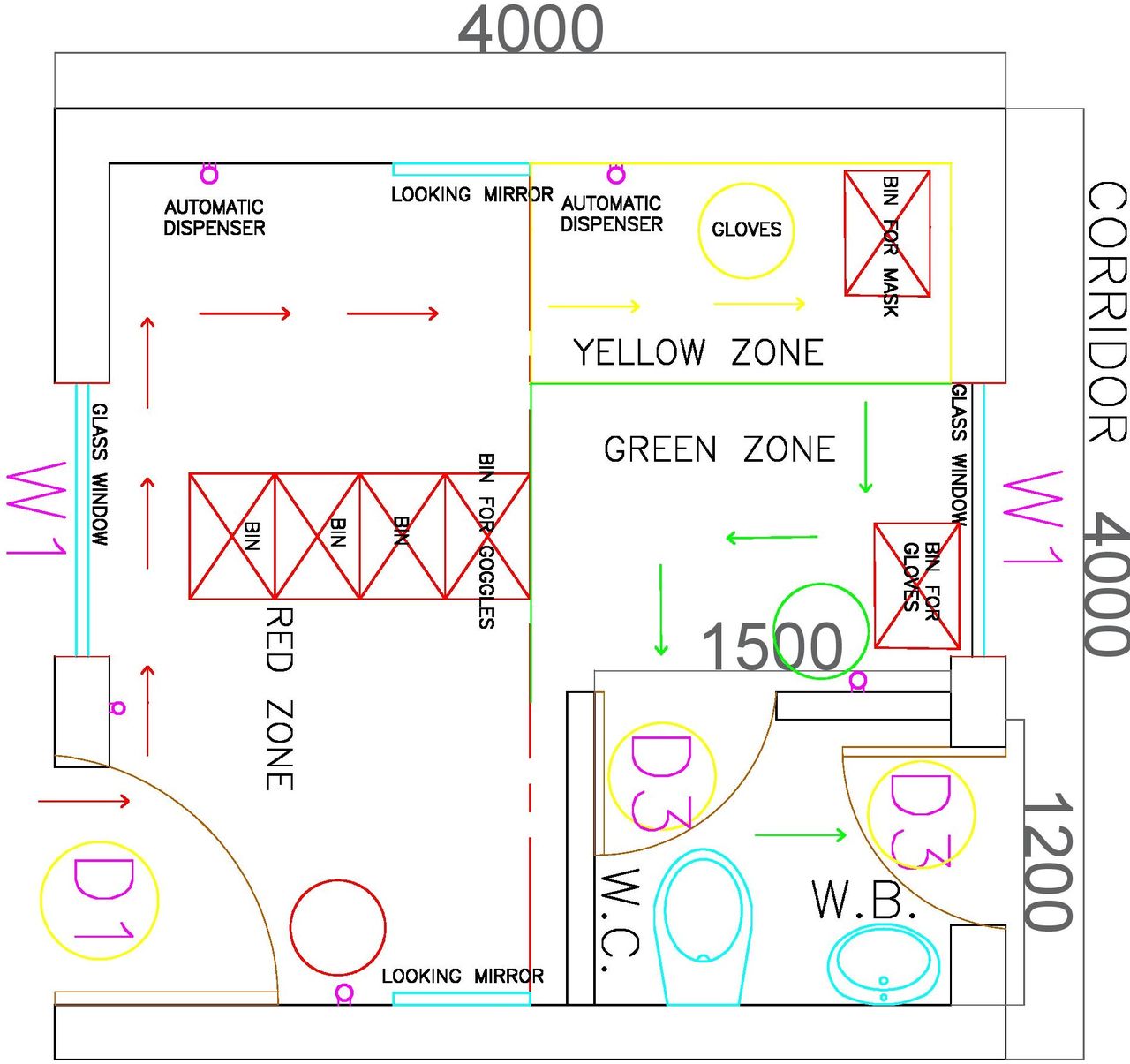
We recommend an area of 16 m2 each for donning and doffing areas (figure 1). This was calculated based on the best practices which, inter alia, included that there should be space to permit a wide range of movements of the HCW without restricting movement or causing to bump into obstacles. The measurements of range of movements of individuals ranging in height from 152 to 189 cm were calculated. Space required for each step of doffing was calculated as the HCW progressively proceeded from a more contaminated to a less contaminated area in a unidirectional manner. Space for various supplies and waste bins that should be within hand’s reach was calculated.

Size, layout and design of the doffing room.
We line listed the set of supplies required to operationalise the donning and doffing rooms (table 1).
Supplies required to set up a donning and doffing area
A doffing area was designed based on the available space (figures 2 and 3) in the hospital.

Layout of the floor in the doffing room.

{kind=link}
{kind=link}
{kind=link}
Design of the doffing room.
Based on literature review, the commonly recognised errors in donning and doffing are listed in table 2. These potential errors were highlighted during training. Fifty HCWs were observed for protocol deviations during donning and doffing. They were immediately corrected by a doffing assistant wherever possible.
Recognised errors in donning and doffing based on literature review that need to be emphasised in training28–30 32–36
We used the 5S tool to set up and sustain the donning and doffing areas (table 3). We created a checklist for the donning and doffing areas (table 4).
5S tool
Checklist for doffing area
We performed repeated PDSA cycles to improve compliance to recommended donning and doffing (table 5). We described measures taken to reduce the different aspects of task load pertaining to doffing (table 6)
PDSA cycle for donning and doffing.
Measures taken to reduce task load during doffing (task load parameters derived from Hart and Steveland’s NASA Task Load Index)26
We used literature review to further refine our PDSA cycles (table 7).
Lessons learnt from literature review used as a strategic tool to refine our PDSA cycles27 37–40
We suggested a theory of change canvas to plan and manage donning and doffing areas (table 8).
Theory of change canvas used to create ideal donning and doffing space
Discussion
We designed and operationalised PPE donning and doffing areas for a COVID-19 care facility within a span of 1 week. The biggest challenge was to train the housekeeping staff and environmental service personnel who had no experience in PPE and to translate the training into practice within a short span of time.
There was considerable awareness and interest in COVID-19 among staff due to social media coverage. However, apprehensions related to the disease were also huge. Focus groups, lectures, picture-guided posters, online training videos and demonstrations on donning and doffing were conducted by infection preventionists. Evidence shows that traditional learning methods (eg, watching educational videos and learning PPE guidelines) are inferior to immersive learning methods, including audiovisual devices and active learning involvement using simulation training that includes feedback on performance in guiding the PPE procedures.22–24 Hands-on practical training should be provided to allow HCWs to develop muscle memory.6 Though instructional videos were circulated to all HCWs, most did not go through the videos on their own unless under supervised persuasion. The anticipated PPE shortage restricted the staff to practise using PPE extensively. We did a literature review to line list all identified donning and doffing errors and used this as a tool to strengthen training and improvise HCW donning and doffing. Repeated PDSA cycles minimised protocol violations during donning and doffing.
The PDSA cycles also enabled us to identify practical issues that every healthcare facility must address while operationalising donning and doffing areas in its facility. Limited hospital layouts disrupt space management for PPE use. Since it was not possible to construct an ideal doffing facility or even make major alterations due to constraints of space, time and raw material supply chain logistics due to national lockdown, the identified available space within the ward and the isolation facility was reconfigured optimally.
Initially, items were frequently moved and placed in inconsistent locations when design did not provide standard, convenient locations, leading to errors, frustration and risky behaviours such as retracing into contaminated area to use alcohol-based hand rubs (ABHRs). However, if items such as bins were immovably fixed at identified locations in the doffing room, then this impaired cleaning. Therefore, the floor was marked with coloured tapes to indicate the placement of bins and stools.
Donning was dissected into nine sequential objective steps to reduce cognitive effort. Nine sequential unidirectional stations were created in the donning room. A poster corresponding to each step of donning was pasted on the wall at each station in sequence along with supply of the relevant PPE on tables at that station. Similarly, 11 sequential stations were created in the doffing room corresponding to each step of doffing. At each station, a poster corresponding to the step was pasted on the wall. Automatic no-touch dispensers were provided in each zone (red, yellow and green) in the doffing room to eliminate the risk of contamination and to prevent wastage of ABHRs, which were being used indiscriminately otherwise.
Apart from the errors recognised in literature, the most frequent behaviour was touching the front part of the mask to adjust the positioning of mask at intervals. Individualised seal checks were not possible due to supply of universal size N95 masks. Fogging of goggles occurred often due to poor fit of masks. HCWs used surgical tapes to seal the masks on the face. This carried a risk of contamination during doffing. However, Bell et al reported that taping may not present significant contamination risk.25 HCWs who used prescription glasses perceived risk of contamination of glasses while doffing.
Engineering staff (plumbers and electricians) were required to enter patient isolation rooms to rectify emergency complaints such as seepage of water and faulty drains. Others such as phlebotomists, physiotherapists, radiographers, dieticians, ambulance drivers, laundry personnel and kitchen stewards also required training in PPE use. These were big challenges as it is known that personnel donning and doffing PPE that they are unfamiliar with or have not received training on during emergency situations increase the likelihood of a doffing error.8 Just-in-time training was provided to them. However, some of these staff doffed expeditiously with less regard to safety and required explicit verbal instructions and prompts by a trained observer on all occasions.
After a few days of regular usage of PPE, some staff exhibited automaticity and reduced compliance to doffing sequence even after being explicitly guided by an observer. The presence of a peer guiding the process may have contributed to their reduced compliance. However, in the presence of a senior supervisor, compliance improved. The mean time spent by HCWs in PPE in the wards or isolation facility was 2.4 (±0.04) hours. Some staff (5%) needed to doff within 2 hours of donning PPE due to extreme discomfort or dizziness.
PPE kits should not be changed frequently to minimise errors during donning and doffing.26 However, PPE supplies changed on four occasions due to unavoidable supply chain logistics and apprehensions regarding the quality of PPE among resident doctors due to a few instances of PPE getting torn while donning. The initial PPE ensemble earlier was replaced with an assembled set consisting of a category III protection level tychem coverall, an N95 respirator, a pair of knee length shoe covers and one pair of goggles due to exhausted supplies. Gloves and hood caps had to be obtained separately. This was followed by a supply of two different kinds of coveralls made of spun bound fabric with one layer of microfilm, which differed in their breathability. The other accessories of PPE were separately obtained and assembled. Non-availability of extra-large size gowns or coveralls was an issue of concern for some HCWs due to exposure of the uncovered areas. Due to change in PPE ensemble, the sequence of donning and doffing of shoe covers had to be altered, which led to confusion and errors among HCWs. This required just-in-time training on multiple occasions. Face shields were preferred compared with goggles. However, evidence is limited about the effectiveness of goggles versus face shields.27
Another managerial issue that required monitoring was sustaining the practice of discarding used N95 masks, goggles, face shields and coveralls in separate containers in the doffing room by HCWs for reuse after disinfection. Ensuring round-the-clock availability of supplies in the doffing room and postdoffing bathroom was another issue. Direct supervision of the doffing room was comparatively less due to perception of high risk of room contamination and required fresh donning to go inside to check and replenish supplies carefully without contamination. The next issue was to ensure that goggles and face shields were disinfected as per the protocol and transported out from the doffing room safely by the nursing assistants. Ensuring availability of supplies such as towels and scrubs in the lockers always required constant monitoring. A checklist (table 4) was created for the supervisor of environmental service personnel who was made accountable to address these issues in the donning and doffing rooms in every shift.
The availability of all supplies within doffing room, visual prompts and affordances were not sufficient to ensure full compliance with doffing protocols. Fogging of goggles hindered reading doffing posters on the wall for some HCWs. Fatigue also contributed to lack of attention by the HCW during doffing. The presence of a trained observer who provided verbal prompts to the doffing HCW promoted compliance the most. However, some HCWs reported hearing difficulty while in PPE due to which the vocal prompts provided by the doffing assistant during doffing were not heard. This led to the idea of prompting instructions by an observer using a microphone from outside while being able to visualise the doffing process through a glass screen. However, since HCWs doffed at random intervals, ensuring the presence of a doffing assistant always was resource intensive.
Biomedical waste bins for coveralls got filled up faster due to the size of the coveralls. This required more frequent inspection and proactive initiative by environmental service personnel who needed supervisory nudging.
Our experience recommends that water or oral rehydrating solutions should be provided to HCWs at the time of donning and after doffing. There must be space designated for the HCW to sit before entering the doffing room, if the HCW needed to take rest. It was also important to make it known to all the HCWs that these were available for them.
Donning and doffing by different HCWs occurred multiple times due to random arrivals of patients. This caused overcrowding in the doffing room, at times, leading to prolonged waits for other HCW. Some HCWs doffed simultaneously without waiting, which would lead to one of these HCW waiting in the doffing room to enter the bathroom that was already occupied. The waiting in the doffing room without PPE caused apprehensions of exposure to the coronavirus. This was circumvented by preventing simultaneous doffing and by using a set of two rooms, one room to doff and the other room with an attached bathroom to wait if required. Initially, overcrowding happened due to uniform shift timings of staff. We, therefore, staggered the staff duty timings so that at least any one category of staff always remained donned inside the isolation facility at any time, PPEs were not used unnecessarily and doffing of all staff at the end of a shift did not occur en masse.
Conclusion
Our study used evidence-based literature and QI tools to design and operationalise donning and doffing areas with focus on people, task and environment. Our QI will enable healthcare facilities to rapidly prototype donning and doffing areas systematically.
References
Footnotes
Contributors LW conceived, designed the work, collected, analysed and interpreted the data, and wrote the draft of the manuscript. SSi analysed and interpreted the data, provided critical feedback on drafts of the manuscript and finally approved the version to be published. ARS and SSi contributed to the analysis of the write up of the study results, provided critical feedback on drafts of the manuscript and finally approved the version to be published. LW, SSa and ARS implemented the planned actions and agreed to be accountable for all aspects of the work, ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval Our quality improvement (QI) was done as part of the institute’s approved plan to set up a COVID-19 care facility. No personal information of any participant was elicited during any part of the study. SQUIRE guidelines were used to report this QI.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.