Article Text

Abstract
Introduction Debriefing is a process of communication that takes place between a team following a clinical case. Debriefing facilitates discussion of individual and team level performance and identifies points of excellence as well as potential errors made. This helps to develop plans to improve subsequent performance. While the American Heart Association and the UK Resuscitation Council recommend debriefing following every cardiac arrest attended by a healthcare professional, it has not become part of everyday practice. In the emergency department (ED), this is in part attributable to time pressures and workload. Hot debriefing is a form of debriefing which should occur ‘there and then’ following a clinical event. The aim of this quality improvement project was to introduce hot debriefing to our ED following all cardiac arrests.
Methods A hot debriefing tool was designed following simulated cardiac arrest scenarios and team feedback. This tool was then introduced to the ED for use after all cardiac arrests. The team lead was asked to complete a debrief form. These completed hot debrief forms were collated monthly and compared with the department’s cardiac arrest register. Any changes made to cardiac arrest management following hot debriefing were recorded. Qualitative feedback was obtained through questionnaires.
Results During the 6-month study period, 42% of all cardiac arrest cases were followed by a hot debrief. Practice changes were made to resus room equipment, practitioners’ non-technical skills and the department’s educational activities. 95% of participants felt the hot debriefing tool was of ‘just right’ duration, 100% felt the process helped with their clinical practice, and 90% felt they benefited psychologically from the process.
Conclusion The introduction of a hot debriefing tool in our department has led to real-world changes to cardiac arrest care. The process benefits participants’ clinical practice as well as psychological well-being.
- human factors
- cardiopulmonary resuscitation
- resuscitation
- human error
- continuous quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Problem description
The changing nature of our population means that emergency medicine is dealing with an expanding number of patients with an increasingly complex case load. Increasing attendance in a stretched and under-resourced system leads to greater clinical risk and potentially unfavourable outcomes.1 2 These are among the factors that contribute to high levels of staff burn-out and turnover in emergency medicine and nursing.
Debriefing is a process that allows for discussion of both individual and team level performance. The process allows medical teams to analyse performance, develop processes to improve subsequent patient experiences and minimise the risk of future adverse outcomes. Hot debriefing is a form of debriefing which takes place ‘there and then’ following a clinical event. Hot debriefing has the advantage of earlier intervention, improved participation and improved recall of events.3
St Vincent’s University Hospital emergency department treats on average 5000 patients and 7 cardiac arrests per month. There are 5 whole time equivalent consultants, with 20 non-consultant hospital doctors and over 60 nursing staff. To date, there has been no formally established debriefing process used in the department.
A survey of Irish emergency medicine trainees suggests that debriefing is an underused tool in Ireland. There are no formal processes in place in these departments. Instead, debriefing takes place on a case-by-case basis only. Only 2 out of the 14 training sites partake in regular debriefing; both of these were in specialist paediatric hospitals.
Available knowledge
The American Heart Association recommends debriefing following all cardiac arrests attended by a healthcare professional.4 This has been their recommendation since the release of their 2010 guidelines. This recommendation was emphasised by an unbiased report from the Institute of Medicine in 2015: Strategies to Improve Cardiac Arrest Survival: A Time to Act.5 This report highlighted future areas of focus in order to improve cardiac arrest care. One of the findings was the need to adopt continuous quality improvement programmes. The use of debriefing post cardiac arrests was deemed an essential tool to ensure this took place.
It is difficult to establish the quantitative benefits of a debriefing tool in emergency departments, as there are many confounding variables.6 However qualitative improvements in staff morale and education have been identified.7 8 The relative benefits of different debriefing techniques to performing debriefing in emergency departments have been compared,3 9 10 and no one tool has been identified as being superior to others. It is suggested that the process should be adapted to fit local circumstances. Options suggested include a ‘hot debrief’ immediately after the clinical event or a ‘cold debrief’ at a later date.
Specific aims
The SMART aim of our project was to facilitate a hot debrief after cardiac arrests in the emergency department by the end of September 2019. Our secondary aim was to implement continuous quality improvement changes to our cardiac arrest management, based on suggested actions from hot debriefs.
Baseline measurement
We assessed baseline data by performing a chart review and a survey of nursing and medical staff in the department. All in-hospital and emergency department cardiac arrest cases are logged into a hospital cardiac arrest register. Charts for cardiac arrest cases were reviewed for the 6 months from October 2018 to March 2019. There was no documented evidence of a debrief process following any of these cases. These findings were supported by our baseline survey of medical and nursing staff. None of our respondents had taken part in a debriefing process in our emergency department. As part of this survey, we sought suggestions as to why debriefing was not a common practice in our department. The reasons given were lack of awareness, increasing workload and fear of admitting personal faults. Despite these reasons, staff were eager to participate in formal debriefing if a suitable process could be designed and implemented.
Design
We formed a quality improvement team which included an emergency medicine consultant, clinical nurse facilitator and an emergency medicine specialist registrar. The emergency medicine consultant is the head of the resuscitation committee in the hospital. He helped with the hot debriefing tool design and holds overall clinical governance over this project. The clinical nurse facilitator helped to provide nurse education. The emergency medicine trainee designed and modified the hot debriefing document. They were also in charge of medical staff education, data collection and analysis. Prior to cycle 2, we realised we needed to create as many stakeholders and debriefing ‘champions’ as possible within the department. We chose two senior staff nurses to join our project team. These two nurses had recently completed postgraduate courses in emergency nursing and were eager to get involved in continuous improvement initiatives. They contributed to the redrafting of the hot debriefing tool, nursing educational sessions and the day-to-day promotion of the project.
We formulated multiple drafts of the hot debriefing tool to ensure an efficient hot debriefing process, while covering the main points of interest. All drafts were trialled during specifically designed simulation sessions and the final draft was then agreed (online supplementary appendix). The finalised hot debriefing tool ensured discussion would focus on the treatment of cardiac arrests under the following headings: prealert/handover, delegation of roles, airway and breathing, circulation, equipment issues, communication, and documentation. The document prompts the team to agree on two proposed ‘actions’ or areas to improve. These actions should be accompanied by a volunteer who will ensure they are implemented. Finally, areas to document key performance indicators such as time to cardiopulmonary resuscitation(CPR), time to defibrillation, time to airway management and time to resus drugs were added to aid with future auditing.
Supplemental material
We ran information sessions focusing on the process of hot debriefing and its benefits. During these sessions it was emphasised that the process was not aimed at finger pointing or finding blame. Instead the aim of the process was to facilitate a group discussion in order to address staff’s mental health, patient safety and risk management issues.10
Study of intervention
We performed monthly audits of all completed hot debrief documents. The cardiac arrest registry in the department was used to establish the number of cardiac arrests per month and we compared this with the number of debriefs completed.
We recorded the suggested action points from the hot debriefing documents and followed up with the proposed volunteers to establish if suggested changes had been made.
Measures
The outcome measure recorded was the number of debriefs performed and documented per month as compared with the number of cardiac arrests treated in the emergency department. The process measures we focused on involved looking at the practice changes made as a result of the hot debriefing process.
Qualitative feedback was obtained through participant surveys. We sought to establish feedback regarding length of time for completion, psychological benefits and clinical changes.
Analysis
Completed forms were collected monthly. Clinical scenario, participants, outcomes and suggested action points were all recorded. The number of hot debriefs performed was compared with the total number of cardiac arrests treated within the department. This figure was obtained from the cardiac arrest registry. Participant surveys were analysed using SurveyMonkey and Microsoft Excel.
Strategy
Our SMART aim was to have a hot debrief after 100% of cardiac arrests in the emergency department by the end of September 2019. We aimed to implement continuous qualitative improvements to cardiac arrest care as a result of debriefing. We planned to promote the new hot debriefing tool among all staff in the department through simulations, signage and educational sessions. The results of monthly audits were presented to staff at monthly morbidity and mortality meetings. Emphasis was placed on the proposed changes to cardiac arrest care identified by the debriefing process. We felt by highlighting real-life changes it would allow us to showcase the value of debriefing to staff.
Our quality improvement team had regular progression meetings to discuss proposed strategies and interventions. Through these discussions, we adopted the hot debriefing process through repeated plan, do, study, act (PDSA) cycles.
Cycle 1 (April–May)
Our initial cycle began on 1 April with the introduction of the hot debriefing tool. Prior to this start date, didactic and simulated educational sessions were provided to medical and nursing staff. The initial debrief following a cardiac arrest took place in April. Following the first closed loop feedback session provided during April’s morbidity and mortality meeting this figure improved to four debriefs during May, representing 57% of cardiac arrests for that month.
Cycle 2 (June–July)
We recognised that although there was good participation in May, this was unlikely to be sustainable as there was a high level of cross-over of staff involved in a lot of the debriefs. We also noted that the period of doctor changeover was fast approaching. It was for these reasons for our second PDSA cycle we invited two senior staff nurses to join the quality improvement team. They were given the task of increasing awareness among nursing staff, as we felt this was key to ensuring the sustainability of the project. We introduced laminated signage to clinical areas involved in cardiac arrest cases, that is, the resuscitation room, and beside the blood gas analysers. During our next cycle, there were three debriefs performed in both June and July, representing 60% and 30% of cardiac arrests, respectively. It should be noted that this period saw a high level of doctor turnover and the continuity of results may represent a small success in itself.
Cycle 3 (August–September)
Prior to the third PDSA cycle we recognised through a participant survey that staff enjoyed the hot debriefing process and were eager for it to continue. The main obstacles to performing hot debriefing following a cardiac arrest were not time constraints as proposed in our baseline survey. Participants felt the ‘there and then’ element of hot debriefing along with the concise document cut down greatly on time constraints. Issues were raised around staff awareness and high turnover of staff. Therefore, our aim for cycle 3 was to provide education to all incoming nursing staff. We also assigned a ‘debriefing champion’ for the resus room at every nursing handover to provide a daily reminder of the process. Of the cardiac arrests, 60% were followed by a hot debrief in August and 25% in September.
Results
Outcome measures
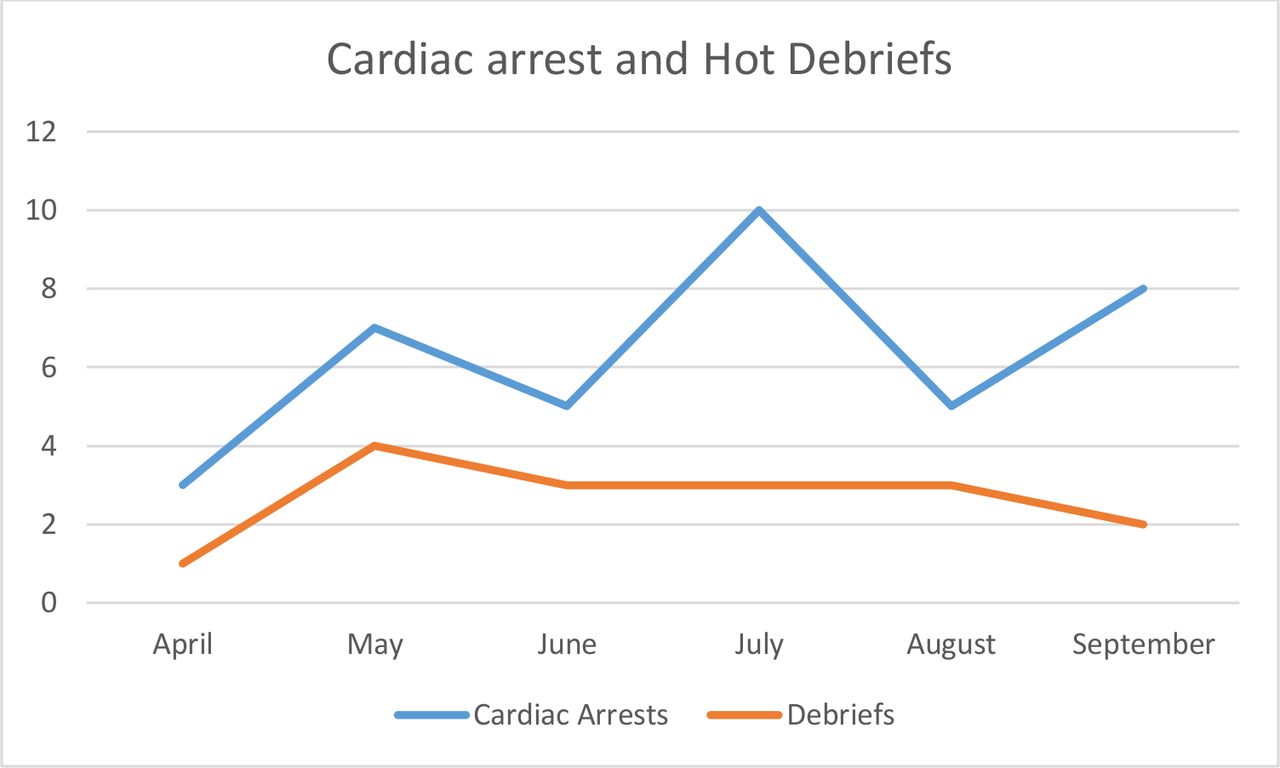
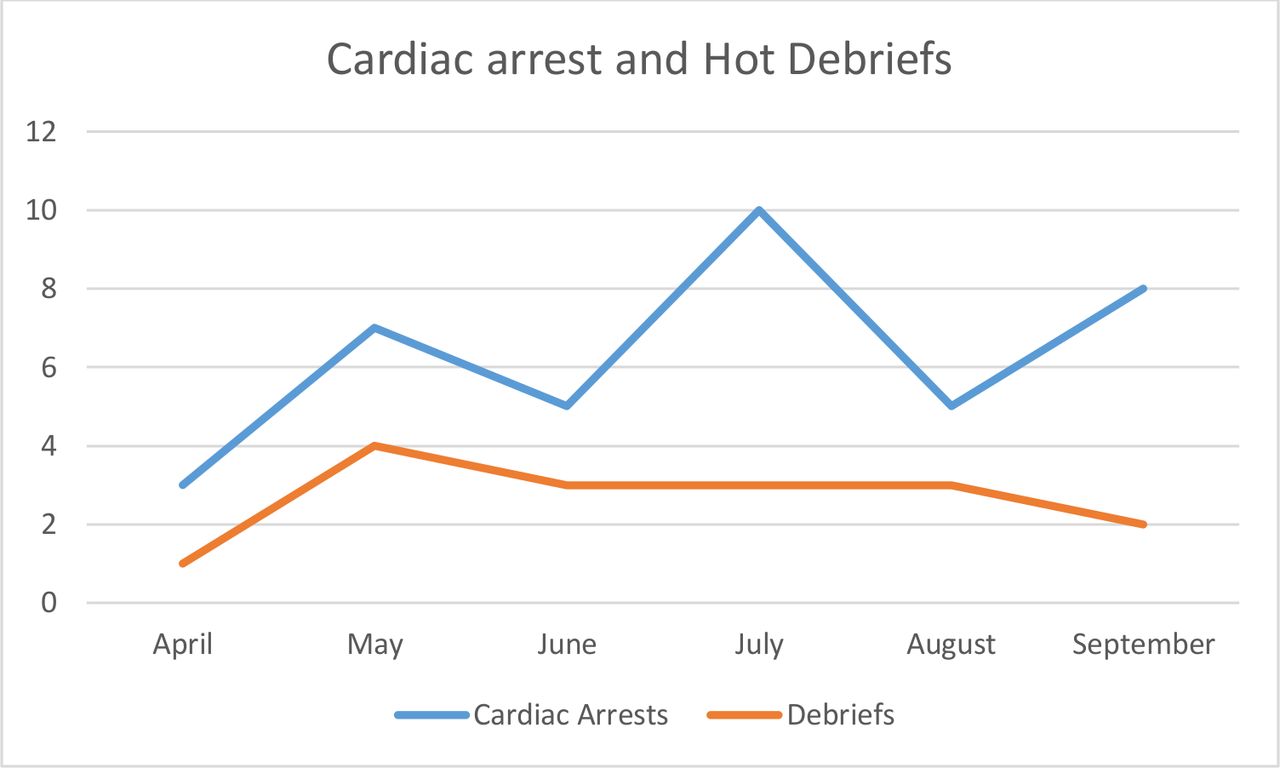
Our primary aim was to facilitate the performance of a ‘hot debrief’ following every cardiac arrest treated within the emergency department. Our baseline audit revealed no hot debrief had taken place following a cardiac arrest in the 6 months prior to our project introduction. As seen in figure 1, the introduction of the hot debriefing tool resulted in 16 hot debriefs being performed over our 6-month study period. This represents 42% of all cardiac arrests treated in our department during that time. The highest absolute monthly figure was in May; four hot debriefs were performed during this month. The highest percentage figure was in June, with 60% of all cardiac arrests followed by a hot debrief.
{kind=link}
Run chart of cardiac arrests treated in the emergency department versus the hot debriefs performed. The study period was from April to September 2019. There were 38 cardiac arrests treated in the emergency department and 16 hot debriefs. Of all cardiac arrests, 42% were followed by a hot debrief.
Process measures
The secondary aim of our study was to record real-world changes and improvements to cardiac arrest care as suggested through the hot debriefing ‘actions’ section. Since the introduction of hot debriefing, changes have been made to resuscitation equipment, non-technical skills and department education. A number of recurrent issues were identified around airway management, such as correct positioning and availability of simple equipment, and as a result the department has purchased tube holders, catheter tips for nasogastric tubes and we are stocking extra pillows in resus to aid with intubation. We have also replaced multiple malfunctioning O2 and CO2 sensors.
In relation to non-technical skills, the poor standard of scribing, note taking and communication during cardiac arrests was regularly recorded on debriefing documents. This resulted in procurement of a mobile white board which is now stored outside the resus room. This has led to a system which involves pertinent information being clearly documented on the white board. This allows all team members to remain informed throughout the case. Use of this technique also provides a prompt synopsis for team members who arrive later in the case.
Following some difficult cases educational topics have been suggested following hot debriefing. It was felt important for all department staff to revise certain high-acuity, low-frequency clinical scenarios. This focused education has taken place through topic presentations as well as immersive simulation scenario training.
Our participant survey revealed 100% of participants felt debriefing improved or changed their clinical practice, 90% of respondents felt the process helped their mental well-being, and 95% felt the time taken to complete the hot debriefing process was ‘Just right’.
Discussion
Lessons learnt
Within our project team we felt hot debriefing was a worthwhile and effective tool to promote quality improvement and improve patient care within the department. It was a false assumption on our part that department staff would appreciate these benefits as easily. We found the hot debriefing process had high participation rates on days when a member of the project’s team was working. Debriefing rates regularly fell off when team members were not present on the floor. We realised that increasing stakeholders and hot debriefing ‘champions’ would be needed to bring improved participation rates. We found monthly feedback sessions gave us a chance to create awareness around practice changes implemented as a result of hot debriefing. These sessions helped create discussion and enthusiasm for the process.
We learnt that, like any new hospital initiative, it is negatively affected by high turnover of the non consultant hospital doctors. The main changeover of staff in our department occurred in July and this contributed to the proportion of debriefs dipping to 30% of cardiac arrests for this period. This changeover made it necessary for us to facilitate re-education of the NCHD staff. The most important learning point from this was the benefit of involving senior nursing staff in our project team. This staff cohort are the most constant group in any department and they help ensure continuity of hot debriefing in spite of any NCHD changes.
Finally, it was presumed the biggest obstacle to hot debriefing completion within our department would be time constraints. On the contrary, we learnt from our participation survey after ‘cycle 2’ that although it was important for the process to be concise, participants did not find it too long. The survey results suggested the main reasons debriefs were not completed were due to lack of awareness and staff simply forgetting while on shift. This is when we introduced a debriefing nurse lead at each handover and erected laminated signage around the resus room.
Limitations
The hot debriefing tool was designed for use after clinical scenarios other than cardiac arrests. It can be used to facilitate open feedback following deaths in our department, unexpected negative outcomes or as requested by staff. We felt these scenarios would be harder to quantify and capture. As a result we decided to focus our present study on hot debriefs following cardiac arrests.
Although the tool is concise it can also be restrictive. We designed it with predetermined headings in order to facilitate efficient discussion, but this structure does not suit all scenarios. This can result in negatively affecting the natural flow of the case discussion.
The tool is currently paper-based only, and as a result this leads to limitations in data collection, data interpretation and expansion of the project. We are currently working on creating an electronic version to allow us to expand the tool to other areas of the hospital and other emergency departments nationwide.
Conclusions
The introduction of a hot debriefing document has led to a hot debrief taking place after 42% of all cardiac arrests treated in our emergency department. Hot debriefing as a tool in itself has allowed focused improvements for cardiac arrest care in our department. In addition, the process benefits participants’ clinical practice and psychological well-being.
This intervention required participation and buy-in from medical, nursing and non-clinical staff. One of our nursing staff team members has been appointed clinical nurse facilitator within the department. One of her new roles will be to familiarise new and existing staff with the hot debriefing process. This familiarisation process will be performed through didactic presentations and in situ simulations. Ongoing promotion and involvement of multidisciplinary staff will lead to increased ownership and sustainability of the debriefing process.
Acknowledgments
The authors would like to acknowledge their nursing and medical colleagues at St Vincent’s University Hospital emergency department for their ongoing support and enthusiasm throughout this project. Without their participation the success of this project would not have been possible.
Footnotes
Contributors SG designed the debriefing tool, simulation scenarios, collected the data, analysed the data, performed staff survey and wrote the manuscript. LM and SK helped with debriefing tool design and staff engagement. IC aided with concept creation, debriefing tool design and writing the manuscript. NS provided overall clinical governance, helped with debriefing tool design, staff engagement and writing the manuscript.
Funding SG was awarded funding from the Spark Innovation Programme to help design an electronic version of the hot debriefing tool.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.