Article Text

Abstract
Background and objectives Cystic fibrosis (CF) is known to reduce lung function as measured by per cent predicted for the forced expiratory volume in the first second (ppFEV1) over time. Our paediatric CF programme demonstrated significant gaps in benchmarked ppFEV1 predicted compared with the national median. Our objective was to assess whether the implementation of a modified Re-Education of Airway Clearance Techniques (REACT) programme could lead to an improvement in lung function as measured by ppFEV1.
Methods This 2-year prospective quality improvement study at Lurie Children’s CF Center for children aged >6 years used improvement methodology to implement a modified REACT programme. Outcome measures were assessed for our entire programme via the CF Foundation Patient Registry (CFFPR) and statistical process control. Comparisons were also made before and after REACT for outcome measures.
Results By the end of implementation, monthly participation rate achieved 100%. Using CFFPR data and SPC, median ppFEV1 increased by 3.9%, whereas only body mass index (BMI) as a secondary outcome increased. Comparison of pre and post REACT showed improvements in average ppFEV1 (95% vs 96%, p<0.0001), FEF25%−75% (82% vs 83%, p=0.0590), rate of ppFEV1 decline (+2% vs −4%, p=0.0262) and BMI percentile (57% vs 60%, p<0.0001).
Conclusions Implementation of a modified REACT at Lurie Children’s paediatric CF programme led to an increase in ppFEV1, FEF25%−75% and BMI percentile.
- clinical microsystem
- control charts/run charts
- education
- paediatrics
- quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Cystic fibrosis (CF) is an autosomal recessive disorder causing abnormal chloride secretions resulting in thick secretions. CF is characterised by respiratory impairment from thick mucus, causing airway obstruction, infection, lung damage and ultimately death.1 A major treatment focus is airway clearance and attention to lung function decline.1
Pulmonary function is assessed by measuring per cent predicted for the forced expiratory volume in the first second (ppFEV1). For patients with CF, the steepness of the rate of decline in ppFEV1 is inversely related to age at death2 and patients with ppFEV1 <30% have a 50% chance of dying within 2 years.3 Thus, slowing down the decline in ppFEV1 is critical.
Evidence-based pulmonary therapies, such as airway clearance techniques (ACT),4 5 are essential to clear secretions and increase ppFEV1. However, adherence is low,6 with medication possession rates as low as 48%.7 Non-adherence to prescribed CF therapies has been associated with healthcare utilisation, increased hospital stays and increased pulmonary exacerbations.8 9
Health education programmes help improve chronic disease management.10 Zanni et al addressed adherence in the Re-Education of Airway Clearance Technique (REACT) programme, which helped in improving median ppFEV1 from 84% to 93% in 1 year. REACT was designed to reinforce and re-educate patients on the importance of daily ACT, assess ACT skills and improve adherence.11
At the paediatric CF programme at Ann and Robert H. Lurie Children’s Hospital of Chicago (Lurie Children’s), 2014 data from the CF Foundation Patient Registry12 (CFFPR) revealed significant gaps from benchmarked ppFEV1; for patients aged 13–17 years, the median ppFEV1 was 83.2%, whereas the top 10 centres in the country achieved 99%. Additionally, comparing the overall ppFEV1 over 10 years, our ppFEV1 in patients aged 6–17 years rose very little (from 85.8% to 89.9%), whereas in the country, it rose from 85.8% to 92.5%.12
If our centre was below the median ppFEV1 of the top 10 centres, then gaps existed in our process for providing optimal respiratory care to our patients with CF. Thus, our hypothesis was that by implementing REACT and thereby improving adherence, knowledge and skills of our patients related to ACT, ppFEV1 would improve. Additional outcome variables were expanded to include forced expiratory flow at 25%–75% (FEF25%–75%), body mass index (BMI) percentile and rates of pulmonary exacerbations requiring intravenous antibiotics to further understand the impact of REACT.
Methods
Context
Lurie Children’s is a 336-bed, paediatric hospital in a major metropolitan area. A unique feature in the Chicagoland area is the presence of five CFF-accredited CF centres. Lurie Children’s CF Center (both paediatric and adult programmes) follows approximately 275 patients, with nearly 150 in the paediatric programme. The centre’s patients consist of almost 20% Hispanic, 8% non-Caucasian, non-Hispanic ethnicities and about 72% Caucasian. Close to 50% receive public health insurance.
Intervention
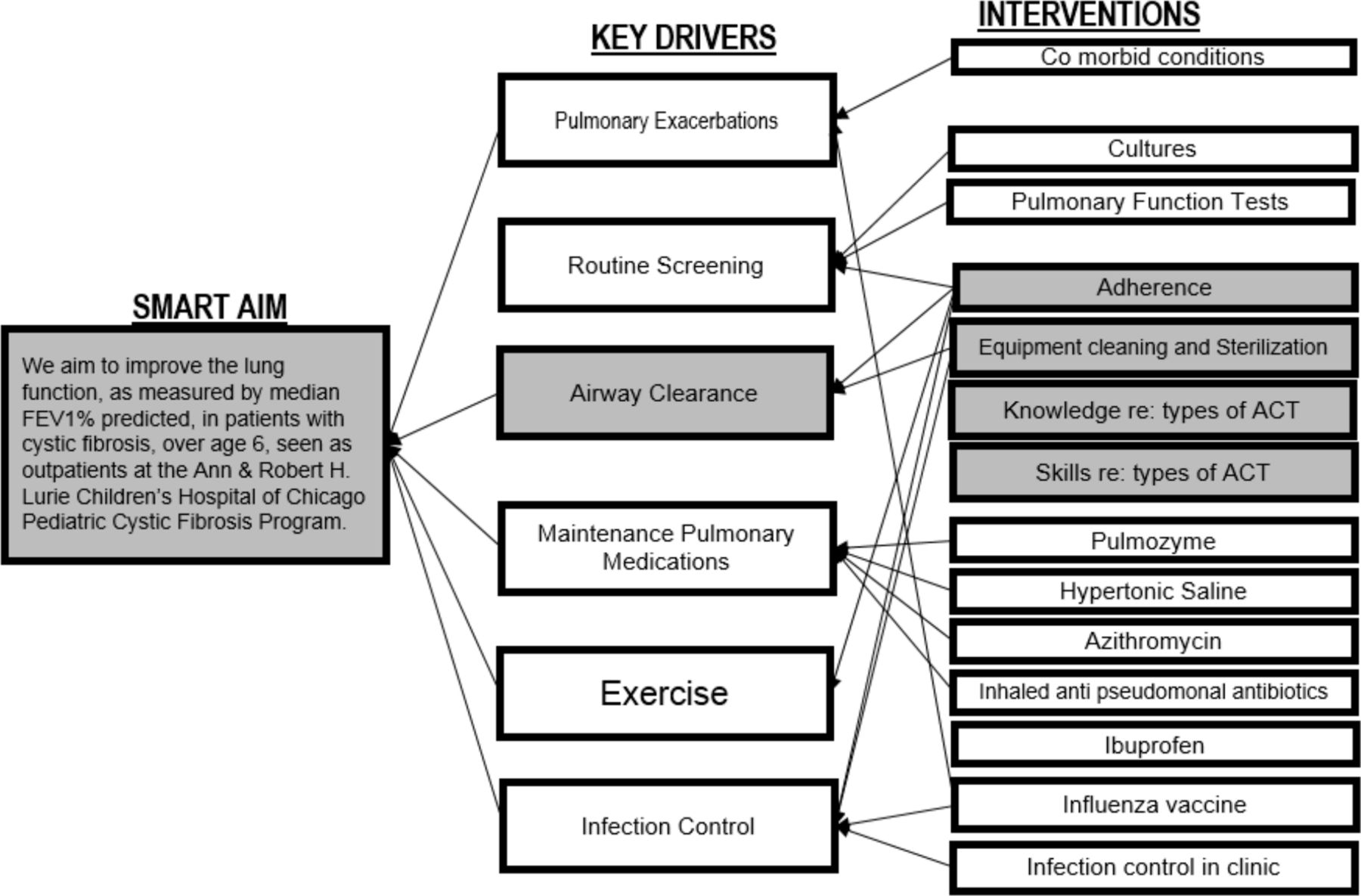
After recognition of a gap in our outcomes, a team was formed, consisting of a physician, medical student, respiratory therapist (RT) and research coordinator. The team explored evidence-based drivers for improving CF pulmonary health using a key driver diagram to facilitate a focus on specific change ideas to increase median ppFEV1 (figure 1). Paediatric CF programme team members determined prioritisation for initial efforts, choosing a focus on fundamentals of knowledge, skills and adherence to ACTs.
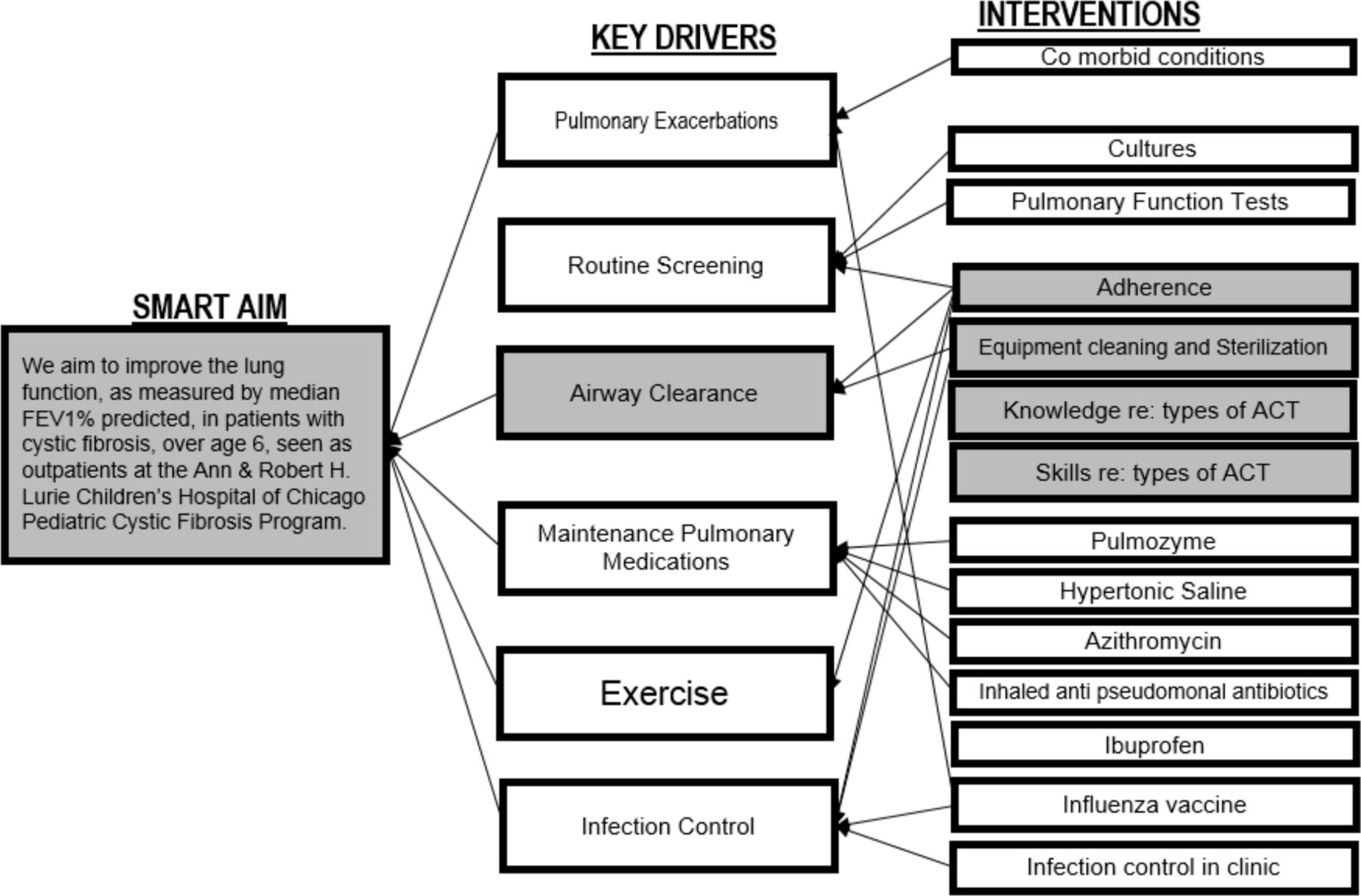
Key driver diagram: a diagram of key drivers of ppFEV1 and interventions that can affect these drivers are shown in the figure. Highlighted in the grey are the drivers and interventions affected by REACT. ACT, airway clearance technique; ppFEV1per cent predictedfor the forced expiratory volume in the first second ; REACT, Re-Education of Airway Clearance Technique.
Implementation of the REACT programme was chosen to improve lung function.11 Permission and resources were obtained directly from the original REACT creators. Our team followed the methodology of the model for improvement in order to ensure that the changes made led to improvement13 and applied REACT to our microsystem. Patient and family involvement were not included in the design or conduct of this study, other than garnering occasional real-time feedback during implementation as part of clinical care. Once the aim, measures and interventions were planned, we proceeded with implementation using the following Plan Do Study Act (PDSA) cycles.
In May 2016, in concordance with the original REACT programme, a letter was sent to introduce families to REACT and invite participation. A modification included translation for Spanish speaking families. The initial letter included an anonymous survey to assess baseline adherence. Unfortunately, only 13 responses were received; therefore, we abandoned the use of the survey.
REACT launched in July 2016. Prior to the annual respiratory care visit, a call to action letter was sent to re-invite participation and remind families to bring the tools used for ACT to their appointment, including ACT devices, air compressor, nebuliser, spacer and inhaled medications. Additionally, a reminder call was made prior to their appointment by a member of the office staff. Despite these efforts, many families arrived unaware of REACT. They did not receive the letters, due to a slow mail system, therefore, letters were sent out earlier. Despite this change, families continued to come to the clinic unprepared/unwilling to participate, so a reminder call was made by the RT, which led to success. The RT was better suited to call because it allowed for any questions or concerns to be answered.
In the clinic, the patient/family completed a form identifying their specific ACTs, adherence to ACT and barriers to adherence, similar to the original REACT programme. If barriers were reported, then the RT worked to problem-solve these issues. Following this, the RT observed the patient demonstrate their ACT to assess the patient’s skills, re-educate and correct any techniques.
A key tool used during the visit was the ‘flip chart’, designed similar to the original REACT programme.11 The flip chart is an educational summary that points out why airway clearance contributes to lung health, lists ACT options and asks key questions to address adherence. The flip chart also had information about the common maintenance pulmonary medications.
Based on findings during the REACT visit, the RT determined to follow-up. If the patient was adherent and had the correct ACT technique, then the return interval was 3 months. Conversely, if they had either incorrect technique or were non-adherent, they returned in 2 months, whereas when they had both poor technique and non-adherence, they returned in 1 month.
Despite our best efforts, patients continued to not bring in equipment. Initially, REACT would not be performed; they would simply receive the typical annual respiratory review, leading to fewer patients participating; therefore, a modified REACT was implemented. Modified REACT allowed for the completion of the in-clinic assessment form, re-education, introduction of a new ACT if desired/necessary and discussion around adherence. We felt this was superior to not doing REACT. Follow-up at subsequent visits with pieces of equipment allowed for further knowledge, skill and adherence assessment.
Modified REACT also included changes to the script for the flip chart when we observed younger children were often confused by certain language. A simpler language depending on the age of the child was used. In addition, educational focus directed at the parent(s) was completed for sections more suited for the parents than younger children.
Time is always an issue during the clinic, with all CF team members working to keep an efficient flow. To minimise clinic time for our patients, annual reviews were limited to one discipline (dietician, social worker or RT) per visit. A typical annual respiratory review covers ACTs, adherence, equipment and a chest wall assessment; therefore, the addition of REACT with the assessment form, demonstration of the technique and use of the flip chart was time consuming. Setting expectations with families about the increased time was valuable. Although most families/patients were very engaged with REACT, not everyone was pleased with how long REACT took, therefore, additional modification occurred. If a family/patient expressed an issue with the time, then the RT adjusted, including eliminating/reducing the use of the flip chart, removing request to bring in inhaled medications, eliminating completion of aerosol treatment and/or excluding chest wall assessment. Documentation facilitated completion at a future appointment.
Study of the intervention
Data were collected monthly and quarterly from the CFFPR and analysed using statistical process control (SPC). Baseline data were collected from quarter 1 of 2012 through quarter 3 of 2016. Prospective data were monitored for 2 years after the initiation of REACT. For our process measure, data extended through November 2018 due to significant success with our modification of REACT.
Measures
For each value in our demographics, the best for each patient was used per study period. To identify positive cultures, any culture within the year was considered positive. Our process measure was participation rate, defined as the per cent of patients per month due for annual respiratory care review who completed REACT. Additional process measures we endeavoured to track included baseline adherence data, per cent of completed/incomplete REACT sessions, per cent requiring modification of REACT and follow-up intervals based on adherence and technique. Outcome measures tracked per quarter were each patient’s maximum for median ppFEV1, median FEF25–75, median BMI percentile and number of intravenous antibiotic courses for all patients. Of those patients who completed REACT, outcome measures and rate of decline in ppFEV1 were assessed for six quarters prior to and six quarters post REACT.
Methods of measurement/analysis
Statistical analysis:
Ongoing analysis of both process and outcome measures were tracked on SPC charts using standard criteria to detect a shift.14 In addition to using SPC to analyse significance, comparisons were made between outcomes for patients who participated in REACT compared with those who did not participate in REACT using the Student t-test.
Ethical considerations
REACT received approval from our Institutional Review Board. As this was a quality improvement effort and part of routine clinical care, specific assents/consents for participating were not required. Individuals who participated in REACT and had signed consents for the CFFPR were included.
Results
Demographics
Baseline demographics for our entire CF centre, for REACT participants and for non-REACT participants are shown in table 1.
Baseline demographics
Process measure
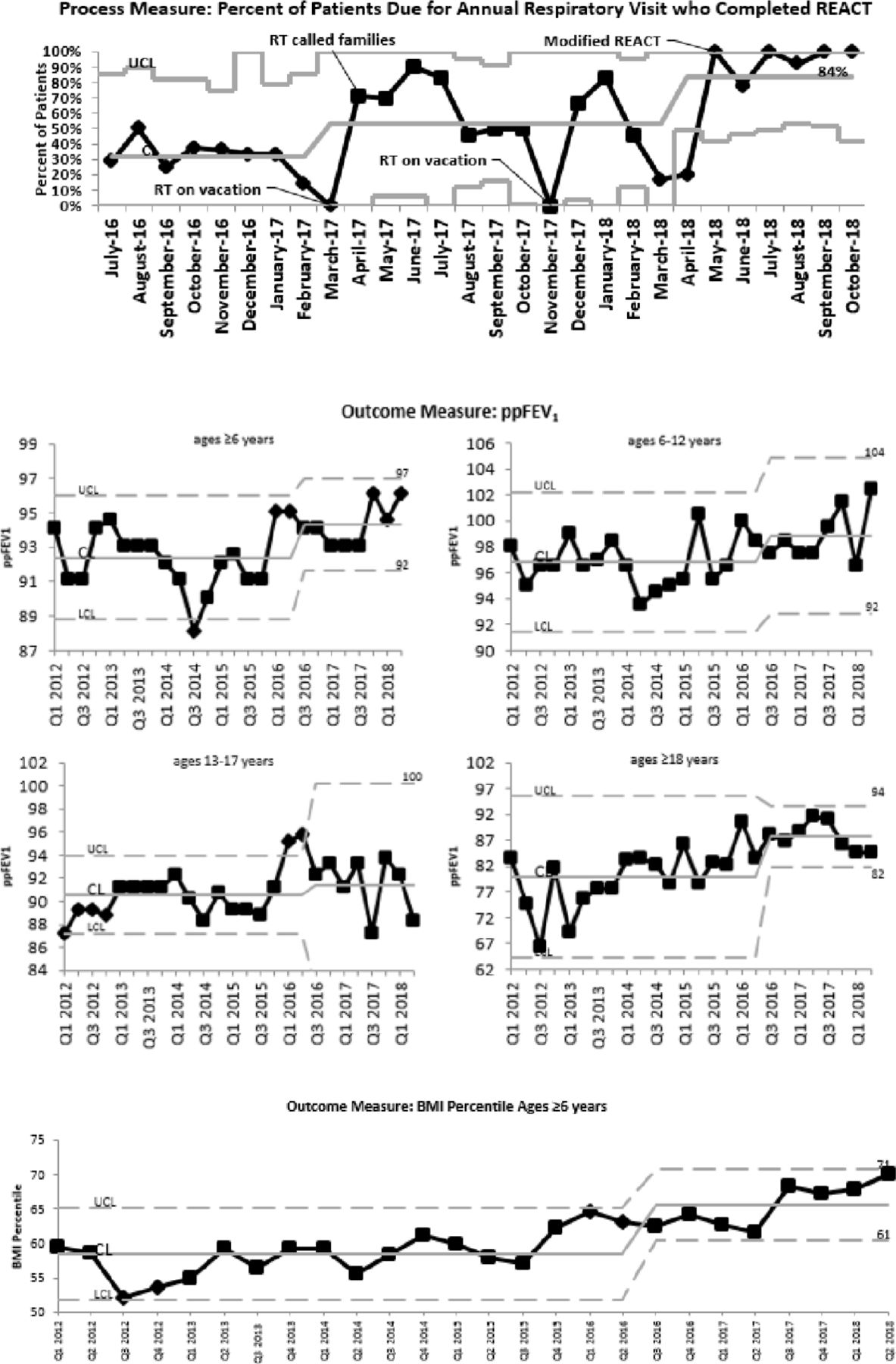
Figure 2 demonstrates the SPC chart displaying the participation rate by month. No baseline data were available, however, in the first 10 months, the centre line of 29% of patients completed REACT, after which, four of five data points were above one sigma, therefore a shift was made, demonstrating an increase to a median of 53% after April 2017. A second shift occurred when two of three points on the same side of the centre line were above two sigma, as indicated with an increase in the median to 95% after May 2018. Both shifts demonstrated significant changes in the process. Unfortunately, our PDSA cycles for baseline adherence data, per cent of completed/incomplete REACT sessions, per cent requiring modification of REACT and follow-up intervals were not successful.
{kind=link}
{kind=link}
Process measures: annotated statistical process control chart showing P chart for per cent of patients who were due for their annual RT visit who completed REACT. Outcome measures: statistical process control chart showing XmR (mR chart not displayed) for median ppFEV1 for patients per quarter and median BMI percentile for all patients aged over 6 years per quarter. BMI, body mass index; CL, centre line, LCL, lower control limit, ppFEV1, per cent predictedfor the forced expiratory volume in the first second; REACT, Re-Education of Airway Clearance Technique; RT, respiratory therapist; UCL, upper control limit.
Outcome measures
Per cent predicted for the forced expiratory volume in the first second
Results from the CFFPR demonstrated a median ppFEV1 of 89.9% in 2015 for patients aged 6–17 years at Lurie Children’s prior to REACT, and 93.8% in 2017 after 18 months of REACT. Data for the top 10 centres’ median ppFEV1 in this age were not available in 2017, however, it rose from 99.9% in 2015 to 100.5% in 2016, an increase of 0.6%. During this same time, at Lurie Children’s, an increase for this age was 1.8%, from 89.9% to 91.7%.
In 2015, the median ppFEV1 for patients aged 6–12 years at Lurie Children’s was 92.4%, increasing to 97% in 2017. Data for the top 10 centres’ median ppFEV1 in this age were not available in 2017, but in a comparison between 2015 and 2016, the median ppFEV1 in this age at the top 10 centres increased from 104% to 104.3%, an increase of 0.3%, whereas at Lurie Children’s, it rose from 92.4% to 93.6%, an increase of 1.2%.
The median ppFEV1 for patients aged 13–17 years at Lurie Children’s rose from 87.9% to 98.5%. At the top 10 centres, it rose by 0.8%, from 97.7% to 98.5% between 2015 and 2016, whereas at Lurie Children’s, it increased from 87.9% to 88.9%, an increase of 1%.
Lurie Children’s median ppFEV1 in patients aged >18 years increased from 78.8% in 2015 to 79.2% in 2016, an increase of 0.4%. During this same time frame, at the top 10 centres, in patients aged >18 years, it rose from 85.6% in 2015 to 85.7% in 2016, an increase of only 0.1%, whereas at Lurie Children’s, it rose from 3% to 81.8% in 2017. Data from CFFPR include all patients at the centre level over age 18, not exclusive to the paediatric programme.
During REACT time periods, locally pulled data of the maximum ppFEV1 per person per quarter were displayed on SPC charts (figure 2). Baseline data were used to determine control limits and centre line. A shift in the centre line and control limits was placed at the time of starting REACT (quarter 3 2016) to signify a new process. For ppFEV1 in both patients aged ≥6 years and patients aged ≥18 years, a run occurred (defined as more than eight points above centre line). For patients aged ≥6 years, the median ppFEV1 increased from 92.3% to 94.24% after REACT. For patients aged ≥18 years, the ppFEV1 increased from 80.2% to 88.1%. Neither the ppFEV1 for patients aged 6–12 years nor those aged 13–17 years demonstrated any significant change, increasing from 96.3% to 98.4% and from 90.3% to 91.2%, respectively.
Forced expiratory flow at 25%–75%
Evaluation from locally pulled data for FEF25%–75% showed no difference for all ages (not shown).
BMI percentile
Using CFFPR data, the median BMI percentile for patients aged 2–19 years at Lurie Children’s increased from 61.9% in 2015 to 65.9% in 2016 and 68.2% in 2017. Data for the top 10 centres were not available in 2017, however, median BMI percentile rose from 67.8% in 2015 to 69% in 2016, an increase of 1.2%, whereas for Lurie Children’s, it increased by 4%.
During REACT, locally pulled data of the median BMI per person per quarter for patients over age six are displayed in an SPC chart in figure 2. A run occurred with more than eight points above the centre line, rising from a median of 58.6% to 65.7%.
Intravenous antibiotics
Using CFFPR data, the per cent of patients with one or more pulmonary exacerbation who were aged <18 years at Lurie Children’s was 26.8% in 2015 prior to REACT and 21.2% in 2017, after 18 months of REACT. For patients aged >18 years, the per cent of patients with one or more pulmonary exacerbations decreased from 50% to 41.3% during the same time. Note that for CFFPR data in patients aged >18 years, data from both paediatric and adult programmes are included.
Pre and Post
The average ppFEV1 of patients who completed REACT prior to completion was 95% and rose to 96% post REACT (p<0.0001) (whereas median went from 95% pre to 97% post). The average FEF25%–75% rose from 82% to 83% over the same time frame (p=0.0590) (with median remaining 83 for both pre and post) and average and the median BMI increased from 57% to 60% (p<0.0001). The mean decline in ppFEV1 1 year prior to initiation of REACT was −4% compared with the year post REACT increase of 2% (p=0.0262), with similar changes in the median from −4.5% decline prior to REACT and median of 0 decline post REACT.
Discussion
Interpretation and summary
Implementation of a modified REACT at our programme contributed to an increase in ppFEV1, BMI percentile and a decline in intravenous exacerbation rates as determined by CFFPR data. Individuals who participated in modified REACT had improvements in ppFEV1, FEF25%–75% and BMI percentile and a decrease in the rate of decline in ppFEV1. To our awareness, this report is the first to demonstrate the effect of REACT on outcomes such as FEF25%–75%, BMI and intravenous exacerbations.
Numerous drivers lead to improved pulmonary function as outlined in our key driver diagram (figure 1). Various efforts have been published, such as improving the treatment of outpatient pulmonary exacerbations defined by decline in ppFEV1,15 inpatient exacerbations16 and increasing the usage of maintenance pulmonary medications.17–20 Our modified REACT programme focused on improving knowledge, skills and adherence to airway clearance.
Successful implementation of a modified REACT programme in the clinic was demonstrated by the significant increase in participation. During the last 3 months of implementation, we established 100% participation. Achievement of high participation was due to tracking data over time and problem-solving barriers to incorporating REACT into the clinic. In comparison, 91% of the patients participated in the original REACT; however, information regarding the time it took to achieve this result was not described. Other improvement efforts in CF show variable rates of adherence to process measures, ranging from 51% to >90% over periods varying from 1 year to several years.15 18–20 Our achievement of >90% completion rate is a success and comparable with other reports.
Implementation of the original work on REACT11 resulted in a 9% increase in median ppFEV1, whereas our programme’s median ppFEV1 increased by 3.9%. One possible reason for this difference is the distance from the national median at the time of initiation. In the original REACT,11 the baseline ppFEV1 was 7% below the national median, whereas our centre’s baseline ppFEV1 was only 3% below. Is there a greater opportunity for improvement when outcomes are further from the national median? Variation in degree ppFEV1 improvement has been demonstrated in other reports: a 9% increase15 over 5 years, starting 5.4% below the national median, a 5% increase in 1 year,19 starting 3.8% above the national median, and 2.9% increase over 4 years, starting 2.4% above the national median.20 National medians were obtained from the CFFPR as they were not reported in these studies. Additionally, interventions in these efforts were focused on other key drivers of ppFEV1 compared with ours, therefore they are not directly correlated to our work.
Another outcome we studied was the rate of decline of ppFEV1. In the natural progression of CF, ppFEV1 declines over time, with recent estimates demonstrating negative rates of decline for all ages21; however, our patients had a decrease in the rate of decline after completing REACT, from −4% to +2%. Another quality improvement project that studied adding an annual review found that 28.9% of patients had a better ppFEV1 in 2015 than at baseline in 2012.17 In our population of patients, 66% had an increase in ppFEV1, when comparing the quarter immediately prior to completing REACT and 1 year later.
During the time frame that REACT was implemented, an increase in BMI percentile occurred within the population; however, the participants in REACT started with a higher BMI during year 1 of implementation that contributes to some confounding. Although REACT did not specifically target nutrition, nutrition and lung function outcomes are tightly linked.22–24 Additionally, as BMI drops to <50th percentile, ppFEV1 also declines.25 Therefore, it is not surprising that as ppFEV1 increased, BMI increased.
Limitations
This study was limited by the inclusion of data from one small paediatric programme. All patients were included, and confounding interventions were not controlled. Education and initiation of chronic maintenance pulmonary medications could occur during the REACT session but could also be done outside of a REACT session and were not controlled for during the implementation of this programme. Furthermore, our data may be skewed by CFTR modulators. Ivacaftor was approved for patients aged 6 and older in 2012 and lumacaftor/ivacaftor was approved for patients over age 12 in mid-2015 and expanded to 6–11 years of age in fall 2016. Based on CFFPR data for our centre, about 65% of patients of all ages, eligible for ivacaftor, were prescribed ivacaftor and about 75% were prescribed lumacaftor/ivacaftor. Additionally, the pre–post analysis of REACT had a small sample size which could mean that our findings are due to chance.
Additional limitations that require specific mention are those inherent to quality improvement work. Although the plan was to implement the REACT programme in a systematic manner using the model for improvement as our guide, our PDSA cycles were anything but linear. Specifically, we had an extremely low rate of return for our baseline adherence survey and we did not accurately track the per cent of completed/incomplete REACT sessions, per cent requiring modification of REACT, and follow-up intervals. In a review of the reporting of PDSA cycles in the literature, Taylor et al found that <20% of papers documented an iterative series of cycles.26 Tomolo et al describe PDSAs as a series of false starts, miss firings, plateaus, regroupings, backsliding, feedback and overlapping sessions.27 Our work definitely fits within these categories for some measures, and thus we do not have an exhaustive assessment of our processes, however demonstrate a more real-world improvement effort.
Conclusions
In summary, implementation of an evidence-based quality improvement initiative to improve knowledge, skills and adherence to ACTs in CF through the implementation of a modified REACT programme led to improvements in ppFEV1, BMI and reduction in pulmonary exacerbations treated by IV. In those who completed REACT, improvements in ppFEV1, FEF25%–75%, BMI and rate of decline of ppFEV1 were seen. We successfully implemented a REACT programme through modification for our microsystem, allowing for flexibility with our patients and families.
Acknowledgments
The authors thank the patients and their families who allowed them to work to improve the care they receive.
References
Footnotes
Contributors CR conceptualised and designed the study, analysed the data, drafted the initial manuscript, and reviewed and revised the manuscript critically for important intellectual content. CO'M conceptualised and designed the study, collected data, drafted the initial study, and reviewed and revised the manuscript critically for important intellectual content. JN acquired the data and reviewed and revised the article critically for important intellectual content. AS conceptualised and designed the study, analyzed and interpreted the data, drafted the article, and reviewed and revised it critically for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.