Article Text

Abstract
Medical inpatients often have important risk factors for venous thromboembolism (VTE). In our institution, VTE prophylaxis in this group was underused. The main barriers identified were inattention to VTE prophylaxis, competing priorities and lack of confidence in the decision-making. We aimed to improve the rate of VTE prophylaxis use by introducing a paper-based risk assessment tool, with actionable management recommendations within the prescription chart. The rationale was that an assessment tool at the point of prescribing can reduce steps between decision-making and prescribing process, thus promoting confidence and acting as a reminder. A total of 552 prescription charts completed over a period of 29 weeks were examined during the baseline period. In the postintervention period, 871 charts completed over 40 weeks period were examined. The risk assessment tool was completed in 51% of the cases examined in the postintervention period. The introduction of the risk assessment tool was associated with a significant change in the pattern of VTE pharmacological prophylaxis use. The change occurred when the form was made highly visible and enclosed in the prescription chart. The pharmacological prophylaxis use was higher with a completed assessment form than without (mean (SD) 97.5% (7.6%) vs 70.1% (19.4%); p<0.0001). The rate of appropriate prophylaxis decision was 98.2% (SD 5.2%) with a completed assessment form, and 80.7% (SD 17.9%) when it was not used. The qualitative interviews revealed positive themes; many users found it useful, easy and convenient to use. Our data have shown that a paper-based VTE risk assessment tool placed within the prescription chart could substantially improve the rate of appropriate assessment and VTE prophylaxis implementation. This suggests that tool clearly needs to be a seamless integration into the workflow to capture users’ attention and mitigate the influence of time perception.
- venous thromboembolism
- quality improvement
- patient safety
- medication safety
- clinical practice guidelines
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- venous thromboembolism
- quality improvement
- patient safety
- medication safety
- clinical practice guidelines
Problem
Venous thromboembolisms (VTEs) can be life threatening. If not life threatening, then they can carry large associated morbidity with the need for anticoagulation, pain and post-thrombotic complications. Previous audits have shown a low and variable rate of adequate assessment and prescribing of VTE prophylaxis. To understand the problem, this quality improvement project was carried out within acute and general medical wards at a tertiary hospital in Edinburgh. The department of acute and general medicine receives an average of 70 medical admissions per day. All patients who have been assessed and clerked for admission were included. The quality improvement team comprised foundation year doctors, a core trainee in acute medicine, a pharmacist, ancillary support staff and consultants.
Our previous interventions have been largely focused on prescribing rather than supporting a clinical decision-making process and assessment. Our prescription chart (paper-based) does not include a VTE risk assessment tool. Thus, in this project, we aimed to increase the rate of appropriate VTE prophylaxis among medical patients by introducing a risk assessment tool within the prescription chart. The rationale was that a risk assessment tool at the point of prescribing can reduce steps taken between clinical decision-making and prescribing process in a busy environment, promote confidence and act as a useful reminder. We also introduced educational sessions (as part of the quality improvement educational programme) after each staff changeover to promote awareness and to provide feedback on VTE prophylaxis performance.
Background
Hospital-associated VTE accounts for 25%–50% of all VTE events.1 In the UK, hospital-associated VTE causes between 25 000 and 32 000 deaths each year.2 Hospitalisation is an important risk factor for VTE, and the risk is not limited to those hospitalised for surgery.3 4 Almost a quarter of all VTE events occur in acutely ill hospitalised medical patients.1 Furthermore, previous studies have shown that the incidence of fatal pulmonary embolus (PE) is higher in hospitalised medical patients than that seen in surgical patients.5 6
Both pharmacological and mechanical prophylaxis have been shown to decrease the risk of VTE.7–9 The National Institute for Health and Care Excellence recommends a formal assessment of VTE risk, together with a decision about prophylaxis to be undertaken for each new patient admission, taking into account relevant contraindications and dose adjustments to low molecular weight heparin based on renal function and the relevant clinical illness.10 The implementation of the national guidance has been associated with reduction in hospital-acquired VTE events.11
The problem is that the use of VTE prophylaxis in medical patients is underused.12 13 Various interventions have been introduced to encourage appropriate VTE assessment and prophylaxis use.14 In our institution, a full guidance to VTE risk assessment and prophylaxis was available on the intranet and advertised through strategically placed posters. The rate of VTE prophylaxis implementation, however, varied considerably. Previous efforts such as preprinted prescriptions and prescribing prompts on the prescription charts did not result in sustained improvements in the rate of assessment or prescription of VTE prophylaxis.
Measurement
Baseline measurement
Baseline measurements were conducted between 5 July 2017 and 1 February 2018 to establish the pattern of VTE prophylaxis prescribing. The main outcome measure was the proportion of eligible cases that received appropriate VTE prophylaxis as recommended by the local protocol. Prescription charts were examined to determine if VTE prophylaxis was implemented. In cases without a pharmacological prophylaxis prescription, contraindication to (or lack of indication for) prophylaxis was ascertained from the medical records to determine the rate of omission (no VTE prophylaxis prescribed when there was an indication in an eligible patient). The rate of mechanical prophylaxis prescription was also recorded. During this period (week 5), electronic medical records were introduced throughout the medical division to replace paper-based case notes. The electronic medical records included a structured entry for ward rounds with a checklist that targeted a broad spectrum of care processes including VTE prophylaxis assessment (‘VTE prophylaxis assessed? Y/N’).
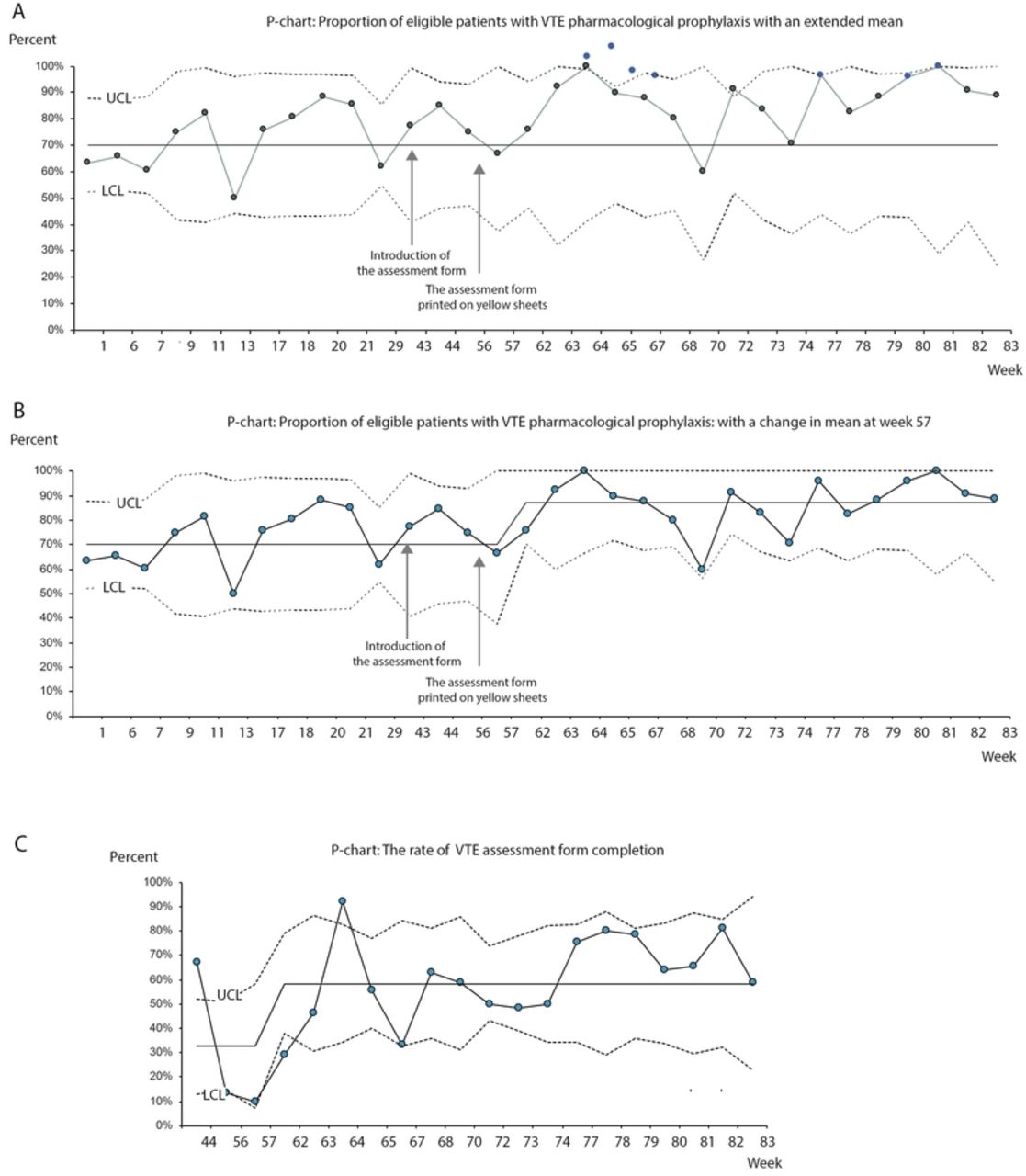
A total of 552 prescription charts completed over a period of 29 weeks were examined during the baseline period. As shown in figure 1, VTE prophylaxis (either pharmacological or mechanical) was implemented in 59.1% (SD 10.8%) of all cases examined. Mechanical prophylaxis accounted for 3.9% (SD 5.4%) of the VTE prophylaxis.

Percentage of eligible patients with venous thromboembolism (VTE) prophylaxis.
Of all the cases examined, pharmacological prophylaxis was contraindicated in 111 (20.8%). In the remaining 441 cases, the mean (SD) proportion of cases with pharmacological prophylaxis was 71.6% (12.2%) with significant variations. The introduction of prompt for VTE prophylaxis assessment in the structured entry for ward rounds (week 5) and educational sessions (week 9) introduced did not result in significant change.
Design
The project team was led by a foundation doctor and a core trainee, and also consisted of a medical consultant and pharmacist. We recognised the need for increasing awareness and education regarding the importance in prescribing correct VTE prophylaxis and documenting the assessment process. We also recognised previous attempts to increase accurate prescribing and decided how we could improve on this, needing a quick and easy tool that would be used on busy shifts.
Educational sessions were launched on 9 November 2017 (week 9). This 1 hour session comprised case-based learning and a presentation on the VTE prophylaxis compliance rate within the department. The session was held at the beginning of each staff changeover (the first week in December, the first week in April, the first week in August). Additionally, the VTE prophylaxis compliance rate within the department was also presented to the junior staff before the end of each rotation.
Focus group sessions were conducted on 20 January 2018 and 6 February 2018 to examine barriers to VTE prophylaxis prescribing. The questions were based on the following dimensions: confidence to implement VTE prophylaxis based on the current protocol, difficulties encountered, suggestions for improvement and whether a risk assessment tool would be helpful.
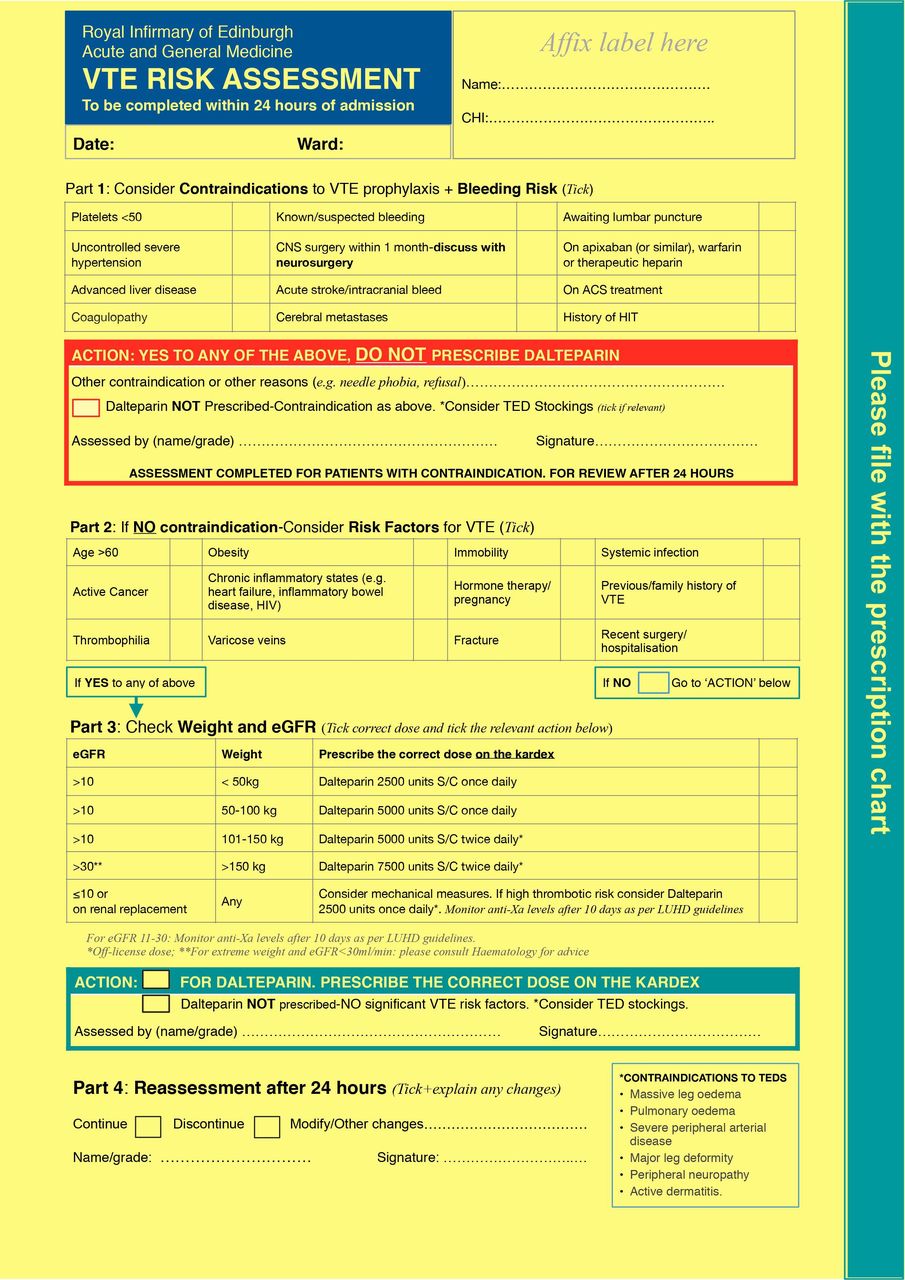
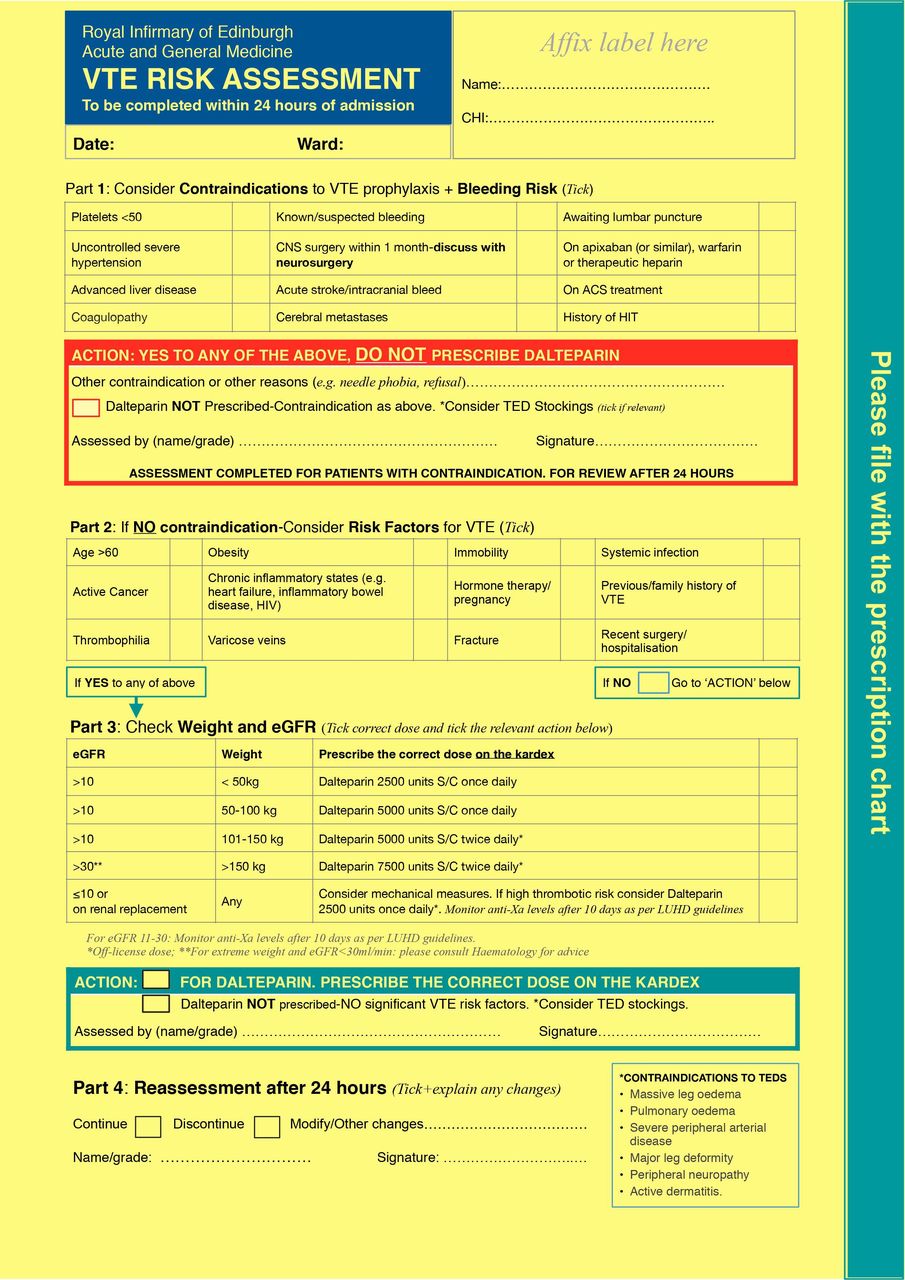
We designed a paper-based VTE risk assessment algorithm based on the current Trust guidelines to be incorporated within the prescription chart (figure 2). Feasibility assessment was performed between 12 and 15 February 2018. The form was first tested in clinical setting on 5 March 2018 and gradually introduced to the entire department. Iterative changes were made to the layouts, wordings and contents based on feedback from junior doctors, consultants and the pharmacy team. It was discussed at departmental meeting and an email was sent to notify all staff within the department. A version for clinical use was launched on 20 March 2018.
{kind=link}
{kind=link}
Paper-based venous thromboembolism (VTE) prophylaxis assessment form.
Strategy
The SMART aim was to improve assessment and correct prescribing by doctors for VTE prophylaxis on the acute medical admissions ward. We undertook 3 PDSA cycles.
PDSA 1: after creating our VTE prophylaxis algorithm tool, and having it in the department next to the kardexes for doctors to fill in, we allowed at least 4 weeks of an embedment process before measuring the impact of our intervention. Postintervention data were collected between 28 April 2018 and 31 January 2019. The outcome measures were as described above. We also assessed whether any increase in the prophylaxis use was paralleled by an increase in the proportion of patients who had VTE prophylaxis prescribed even though it was not indicated, or when there were contraindications (error of commission).
PDSA 2: we decided that the white form in the kardexes was not visible and ‘stand out; enough among all the other paperwork, and so from 1 September 2018 (week 61), the form was printed on yellow sheets in order to increase visibility and likelihood of completion and awareness. We also decided to insert the a4 algorithm page into the inside of the kardex so that the user did not have to get a kardex and a piece of paper to fill in, therefore aiming to minimise a further step, and to increase usage uptake.
PDSA 3: a revision was made on 8 October 2018 to accommodate changes to the local VTE guidelines, and staff were updated once again. The rate of VTE risk assessment form completion was recorded. We also conducted a qualitative survey to seek users’ experience in October 2018 and January 2019. The questions were based on the following dimensions: participants’ views on whether the form was useful, any difficulties encountered, time to complete and suggestions to improve VTE prophylaxis implementation.
Statistical process control (SPC), specifically P-chart, was used to assess the proportion of cases with the specified outcome (quality improvement charts Add-in for Excel V.2.0.23, Process Improvement Products, Texas, USA). Postintervention data were compared with baseline data, and the presence of special cause (non-random) variation was assessed according to standard SPC rules. Quantitative data are presented as frequency and percentage for categorical variables and mean and SD for continuous variables data (Prism V.6.0 for Mac OS, San Diego, California, USA). Comparisons between two groups were analysed using unpaired t-test or analysis of variance for three or more groups. P value <0.05 was considered as statistically significant. Thematic analysis for qualitative data were analysed independently by AL, IS and HP. Briefly, all comments were carefully read, and themes were developed inductively. A thematic framework was devised using Microsoft Excel for Mac V.15.28 (Microsoft, Redmond, Washington, USA). This was deemed as a quality improvement project but the governance committee in our institution and therefore no formal ethical approval was required.
Results
Seven foundation doctors and one core trainee participated in the focus group sessions. The main barrier identified was inattention to VTE prophylaxis. Competing priorities and interruptions while completing the prescription chart were the main factors reported. An important theme emerged was lack of confidence in the decision-making. Participants perceived that VTE prophylaxis prescribing in general medicine was more complex than that experienced in surgical specialties, and this was largely attributed to the heterogeneity of medical presentations. Thus, the decision was often deferred until consultant-led ward rounds; however, this was not reliably undertaken due to time constraints. Another factor was the inconsistent use of the VTE guidelines that were available electronically. Participants felt that accessing these guidelines was a time-consuming and a cumbersome step in the prescribing process. Many were unaware of the posters that featured VTE risk assessment or the prompt that was introduced in the structured ward round entry. While most participants felt that a decision-making tool should be placed within the prescription chart, there were concerns that this can add to the overall time taken to complete the admission process.
Following the focus group sessions, a paper-based VTE risk assessment tool placed within the prescription chart was introduced (figure 2). A total of 871 prescription charts completed over 40-week period were then examined. The average proportion of cases with contraindication to pharmacological prophylaxis documented was higher than that seen preintervention (mean (SD) 40.8% (11.2%) vs 20.8% (7.5%), p<0.0001).
Among those eligible for pharmacological prophylaxis, the introduction of the assessment tool was associated with a significant change in the pattern of VTE pharmacological prophylaxis use; the proportion of cases with pharmacological VTE prophylaxis was higher and more consistent in postintervention than that seen during the preintervention period (mean (SD) 84.6% (10.7%) vs 71.6% (12.1%); p=0.004). As shown in figure 2A, printing the form on highly visible yellow sheets and ensuring that it was always enclosed in the prescription chart (started at week 57) resulted in improved prescription. These changes were associated with a change in the rate of form completion with the average compliance increased from 32.6% to 58.4% (figure 2C), although there were not enough measurements before intervention to determine whether this was a special cause variation. The proportion of mechanical prophylaxis use during this period remained unchanged (mean (SD) 3.0% (1.0%) postintervention vs 3.9% (5.4%) pre-intervention; p=0.6).
The VTE assessment form was completed in 447 (51.3%) of the cases examined in the postintervention period. The proportion of patients eligible for pharmacological VTE prophylaxis was similar between cases with and without the assessment form (mean (SD) 59.2% (15.2%) vs 60.9% (17.2%); p=0.7). However, the patterns of pharmacological prophylaxis used in eligible cases between these groups were significantly different. The proportion of cases with pharmacological prophylaxis was higher with less variations with the assessment form (mean (SD) 97.4% (7.6%) vs 70.5% (19.4%); p<0.0001). There was no difference in the proportion of mechanical prophylaxis (mean (SD) 2.9% (6.7%) vs 2.1% (3.6%); p=0.6).
Once the proportion of patients receiving pharmacological prophylaxis increased, we then assessed whether this was paralleled by an increase in the proportion of patients who had VTE prophylaxis prescribed even though it was not indicated, or when they had contraindications (error of commission). We followed up 290 cases at discharge (from week 72 onwards) and determined the overall rate of appropriate VTE decision. Of these, an assessment form was completed in 200 cases. There were two cases with error of commission identified from each group. One of these cases was when the assessment form and the prescription chart were completed by two different prescribers. The remaining cases involved instances where the prophylaxis was prescribed despite the presence of contraindications.
The rate of inappropriate omission during this period was less in cases with a completed form than those without (mean (SD) 1.7% (5.2%) vs 19.2% (17.2%); p=0.01). Thus, the overall appropriate VTE decision was 98.2% (SD 5.2%) in those with the assessment form completed, and 80.7% (SD 17.9%) when the assessment form was not used.
We conducted a survey to seek users’ experience at the end of each 4-month term for doctors in training. Fifteen foundation and core trainees participated in the survey. Most participants felt that the assessment form was useful, accessible and easy to use. Time taken to complete the form ranged between 10 s and 1 min. The lists of risk factors and contraindications were helpful, and the flow diagram provided clarity to the decision-making process. Participants commented on the positive visual impact of printing the form on yellow sheets and some felt that the layout was better than similar tools previously encountered in other Trusts. An important theme that emerged was inconsistent use. Some participants reported that they were more likely to use the form when there was uncertainty in the decision-making process. In cases that were deemed to be straightforward, completing the assessment form was felt to be too time consuming, especially on busy night shifts.
Lessons and limitations
Lessons learnt
An important lesson learnt is that a thorough understanding of users’ experience is crucial. To this end, the continual feedback from users proved to be beneficial. The narratives provided experiential accounts of prescribing experience and highlighted the attitude and nuances unique to the environment. This feedback resulted in positive changes that enhanced the integration of the form into the workflow and maintained sustainability during changeover.
In our study, neither the educational sessions nor the electronic prescribing prompt made any significant impact to the rate of VTE prophylaxis implementation. The attendances for the educational sessions were variable due to the shift patterns. The electronic prompt was not directly linked to any assessment tool or coupled with the prescribing action. Similarly, passive distribution of guidelines, through strategically placed posters have not been successful. It was evident from the focus group sessions that doctors were unaware of these posters. It is possible that the perpetual visual display in a crowded wall leads to poster fatigue and diminishes its effect.
Limitations
There are limitations that need to be acknowledged. This project was focused on medical patients in a single centre. Our findings may not be generalisable to other specialties such as surgical admissions. Mechanical prophylaxis was underused in our study and was largely unchanged with the introduction of the assessment form. We did not address the proportion of patients with a contraindication to mechanical prophylaxis. However, our project reflects real-world challenges encountered with VTE prophylaxis in medical patients admitted to a large tertiary hospital with a wide variety of presentations.
Conclusion
In this study, we demonstrated the utility of an assessment tool to increase the appropriate use of VTE prophylaxis in medical patients. Through an iterative process, we developed a structured assessment form that could be used as a decision support at the point of prescribing. Our intervention was associated with a shift in the process of prophylaxis prescribing and the special cause variation clearly occurred in those instances where the form was completed. In contrast, there was no demonstrable change in the process when the form was not used despite other ongoing interventions implemented during this period.
Implementing VTE prophylaxis in acute medical care can be a cognitively demanding task. The presenting complaints are diverse and often complex. The numbers of medical admissions are rising, and clinical decisions are increasingly made under pressure. The potential impact is that VTE prophylaxis can be perceived to be less of a priority at the front door. In our study, these factors are compounded by lack of accessible-supporting mechanisms for rapid decision-making and an undefined responsibility for implementing VTE prophylaxis. Thus, the decision for VTE prophylaxis is often deferred to others, and sometimes subsequently missed. Decisions made at admission need to be reassessed as the patient’s condition may change; a clear process and reminder is needed for this to happen reliably.
The structured assessment form may have mitigated some of these issues. Enclosing the assessment form in the prescription chart enhances access to the current protocol. The process flow diagram increases the efficiency of decision-making and reduces the cognitive effort. Several previous studies using a similar intervention have shown improvement in VTE prophylaxis. For example, the standardised paper-based medication chart encompassing VTE risk stratification and prophylaxis guidance in Australian public hospitals has been associated with increased VTE prophylaxis prescription from 52.7% to 66.5% in medical patients.15 In our study, the overall rate of pharmacological prophylaxis use rose from 72% to 85% following the introduction of the assessment tool. The change was particularly significant where the form was used—98% of eligible cases had an appropriate prophylaxis decision.
The proportion of cases with a record of contraindication to pharmacological prophylaxis has also risen significantly with the introduction of the form. It is possible that the checklist reduces the cognitive load, thus allowing user to focus on the decision-making. Interestingly, there is an increase in the proportion of cases with a record of contraindication to pharmacological prophylaxis even when the form was not used. Indeed, some of the survey participants reported that they were less likely to complete the form when there is an obvious contraindication.
The inconsistency in the use of the assessment form remains a challenge. The difficulty is that the form was sometimes discarded without any documentation of an assessment, or more importantly, reasons for omission. In part, it is considered as optional and only necessary when there is an ambiguity. A more challenging issue is that the form is viewed as time consuming and represents a paperwork burden, especially when prophylaxis provision is perceived to be less of a priority. One potential reason is that the assessment form reinforces analytical reasoning process. In a demanding environment, such a reasoning process can be difficult, and the associated cognitive demand can potentially influence the perception of time thus making the assessment tool seems less useful. Overcoming these perceptions is key to a successful implementation. The emphasis for any future intervention should focus on education, presenting the rationale and evidence to promote engagement and safe decision-making. These findings also support the potential role of electronic prescribing with a mandatory support for VTE risk stratification.
In conclusion, we have shown that a paper-based VTE risk assessment tool placed within the prescription chart could substantially improve the rate of appropriate assessment and VTE prophylaxis implementation. However, such a decision-making aid is only effective if it is used and completed properly. Thus, managing human factors is important to its viability. In a high-workload environment, emphasising to clinicians that VTE prophylaxis is an important part of direct clinical care is crucial. A risk assessment tool made available at the time of initial prescribing can be very effective if it is integrated into the usual work of prescribers and presents the information in a way that suits the target audience.
References
Footnotes
Correction notice This article has been corrected since it was published. Author name has been changed from Veiraiah Aravindan to Aravindan Veiraiah.
Contributors HP planned, collected data, drafted and revised, submitted the study. AL planned, collected data and drafted the study. IS planned and collected data. VA analysed the data and designed the statistical analysis, reviewed and revised the study. LD and SD collated data and reviewed the study. YYB collated data.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval This was deemed as a quality improvement project by a governance committee in our institution, hence no formal ethical approval was sought.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relavant to the study are included in the study article.