Article Text

Statistics from Altmetric.com
Problem
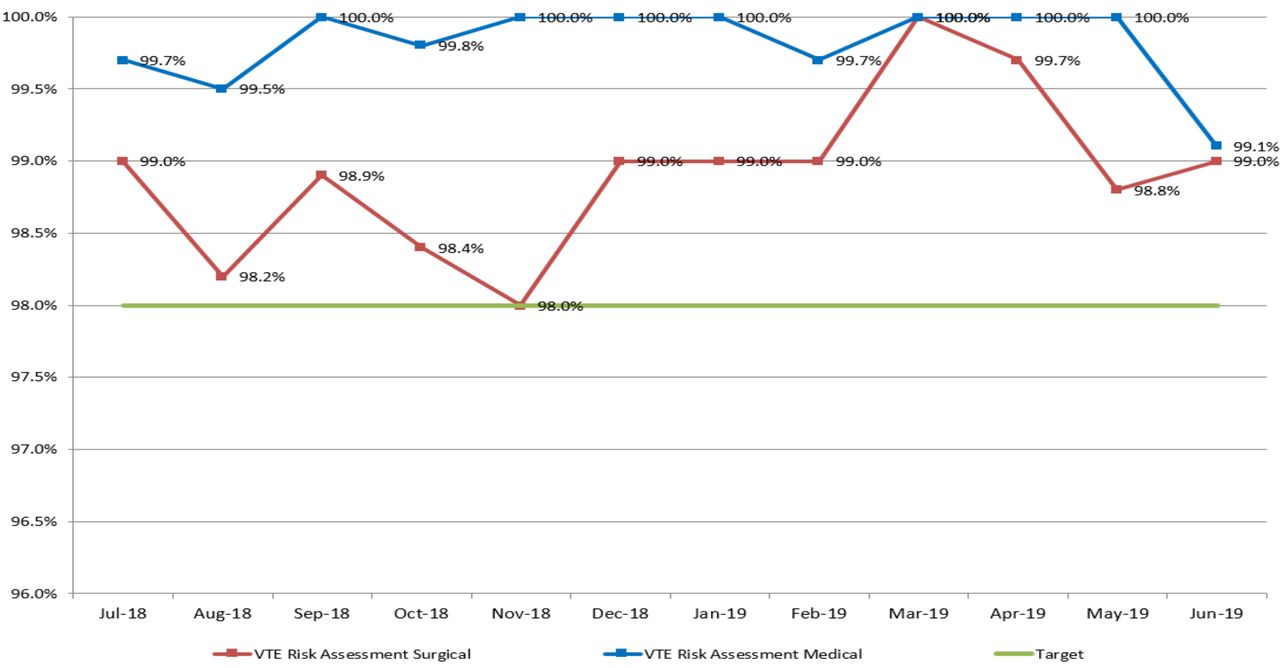
Venous thromboembolism (VTE) prevention is a critical patient safety measure. In a move towards safer practices, our governing body, Abu Dhabi Health Services SEHA, has raised the VTE prophylaxis KPI target from 85% to 95% for all admitted adult patients within 24 hours of admission. Our average VTE prophylaxis rate was 87% and achieving this new target was a challenge. Despite having a VTE risk assessment rate consistently above KPI target of 98% this was not reflected on the VTE prophylaxis rate (figure 1). A VTE prophylaxis improvement multidisciplinary taskforce was formed and included members from physicians, pharmacy, quality and health informatics, and through a collaborative effort led this quality improvement project. The aim of the project was to improve VTE prophylaxis rates from 87% to 95% (new VTE prophylaxis KPI target) through critical thinking and health informatics.
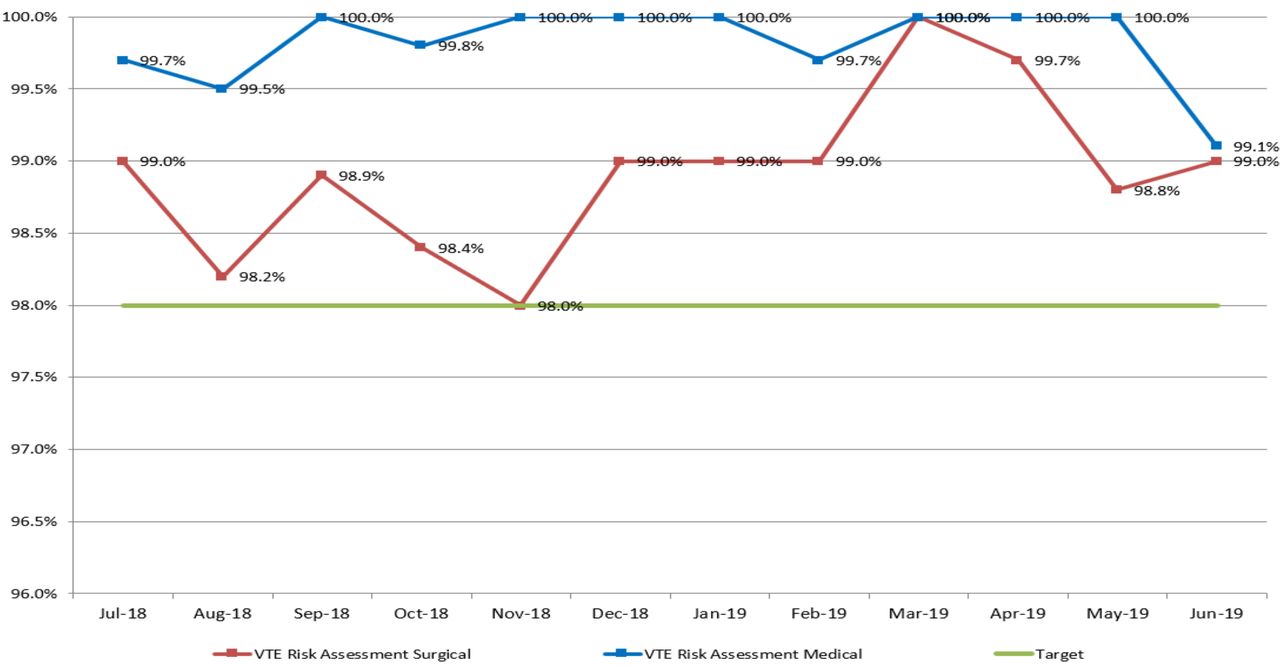
Medical and surgical VTE risk assessment within 24 hours. VTE, venous thromboembolism.
Background
VTE is a leading cause of morbidity and mortality in hospitalised medical and surgical patients.1 The Joint Commission International has identified VTE prevention as a critical patient safety measure.2 3 Mafraq Hospital VTE prevention policy states that all admitted adult patients 18 years and above should receive a VTE risk assessment and all patients identified at risk of VTE with no contraindications receive appropriate VTE prophylaxis within 24 hours of admission in order to reduce the occurrence of VTE in hospitalised patients.
Measurement
The VTE prophylaxis KPI target set by our governing body Abu Dhabi Health Services SEHA is 95%. The average VTE prophylaxis rate preimplementation of interventions was 87%. We used the Caprini model4 5 electronic VTE risk assessment computerised decision support tool6 to help identify VTE risk (figure 2). VTE prophylaxis rate is the percentage of medical and surgical patients at moderate or high risk (VTE risk assessment score of 3 or more) for whom VTE prophylaxis was administered within 24 hours of admission unless contraindicated. The numerator is the number of adult medical and surgical inpatients at moderate or high VTE risk and no contraindication for whom VTE prophylaxis was administered within 24 hours of admission. The denominator is the total number of adult medical and surgical inpatients with moderate or high VTE risk and no contraindication. Exclusion criteria are patients less than 18 years of age, those with low VTE risk (VTE risk assessment score of 2 or less) and those with contraindications to VTE prophylaxis. We also looked at the VTE risk assessment rate (figure 1). The numerator is the number of adult medical and surgical inpatients for whom VTE risk assessment was completed within 24 hours of admission. The denominator is the total number of adult medical and surgical inpatients. Exclusion criteria are patients less than 18 years of age. In the 12-month study period from July 2018 until June 2019 a total of 5475 medical and surgical inpatients were evaluated.

VTE risk assessment for medical/surgical patients. AMI, Acute myocardial infarction; BMI, body mass index; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; DVT, Deep vein thrombosis; FHx, Family history; HIT, Heparin Induced Thrombocytopenia; HRT, Hormone replacement therapy; HTN, Hypertension; LMWH, low molecular weight heparin; PE, Pulmonary embolism; PLT, Platelet; VTE, venous thromboembolism.
Design
The methodology used was a prospective study of VTE prophylaxis compliance in all admitted adult medical and surgical patients 18 years and above admitted to Mafraq Hospital in the study period July 2018–June 2019. A total of 5475 patients were evaluated during the study period. The information was extracted from the electronic medical record by using a specific segmented electronic form that contained all required information, including the medical service, patient name, medical record number, time of admission and time of VTE prophylaxis order. The average VTE prophylaxis rate preimplementation was 87%. Our goal was to improve VTE prophylaxis rates, aiming to achieve the new KPI target of 95% set by our governing body, Abu Dhabi Health Services SEHA. Achieving this newly set target was a challenge. The VTE prophylaxis improvement multidisciplinary taskforce was formed and included members from physicians, pharmacy, quality and health informatics and, through a collaborative effort and a number of interventions, was able to improve VTE prophylaxis rates exceeding the new KPI target.
Strategy
The average VTE prophylaxis rate until the implementation of changes in July 2018 was 87%. VTE prophylaxis improvement multidisciplinary taskforce was formed and included members from physicians, pharmacy, quality and health informatics. Brainstorming sessions were held and root cause analysis was conducted, which identified the areas for improvement placed on the cause and effect diagram (figure 3):

VTE prophylaxis cause and effect diagram. VTE, venous thromboembolism.
Inconsistency in physician documentation in the electronic VTE risk assessment tool.
Inconsistency in physician documentation of VTE prophylaxis contraindications: VTE contraindications were documented in the progress notes and not in the VTE risk assessment tool.
Use of VTE tool-generated risk score rather than the physician-entered risk level as the trigger for VTE prophylaxis.
VTE risk assessment tool not linked to VTE prophylaxis order.
VTE risk assessment tool not updated: new evidence-based medicine American Heart Association/American Stroke Association 2018 guidelines7 favouring the use of mechanical rather than chemical VTE prophylaxis in acute ischaemic stroke not reflected.
Through a collaborative effort, an action plan was developed, and the below key interventions were tested and their impact on improving VTE prophylaxis was measured (figure 4):
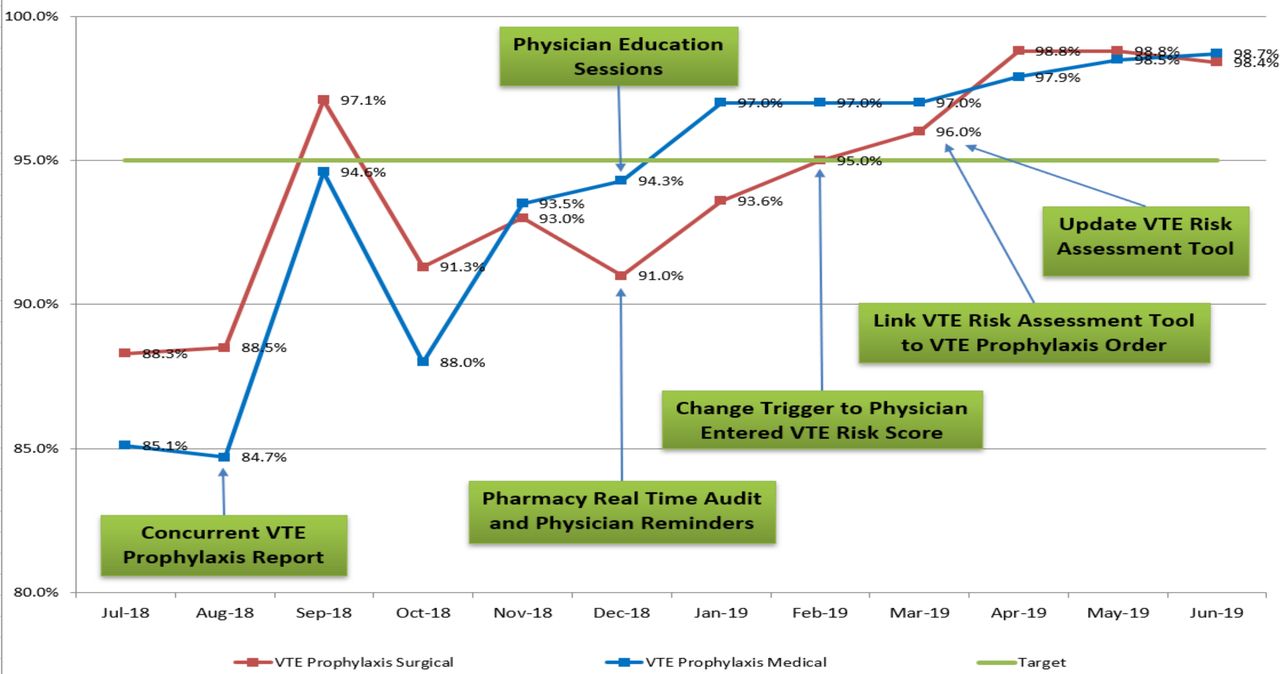
Medical and surgical VTE prophylaxis within 24 hours. VTE, venous thromboembolism.
Quality department in August 2018 started running a concurrent VTE prophylaxis report and shared the data with physicians in order to raise awareness and address concerns. This improved VTE prophylaxis rate from 84% to 93%.
Pharmacy in December 2018 conducted a real-time audit with phone call physician reminders to place VTE prophylaxis order within 24 hours.
VTE Prophylaxis Physician Champions in December 2018 conducted physician-targeted training sessions. The physician champions went to the different departments’ morning meetings and provided educational presentations on the proper completion of the VTE risk assessment tool and documentation of VTE prophylaxis contraindications within the VTE risk assessment tool in addition to the physician progress notes. Post-training sessions, a multiple-choice test was conducted to ensure knowledge retention with a success pass rate of 80%.
Physician education sessions and pharmacy real-time audit with physician reminders improved VTE prophylaxis rate from 93% to 95%.
Quality department changed the VTE prophylaxis trigger to physician-entered risk level instead of the previous tool-generated risk score (figure 5). This improved VTE prophylaxis from 95% to 96%.
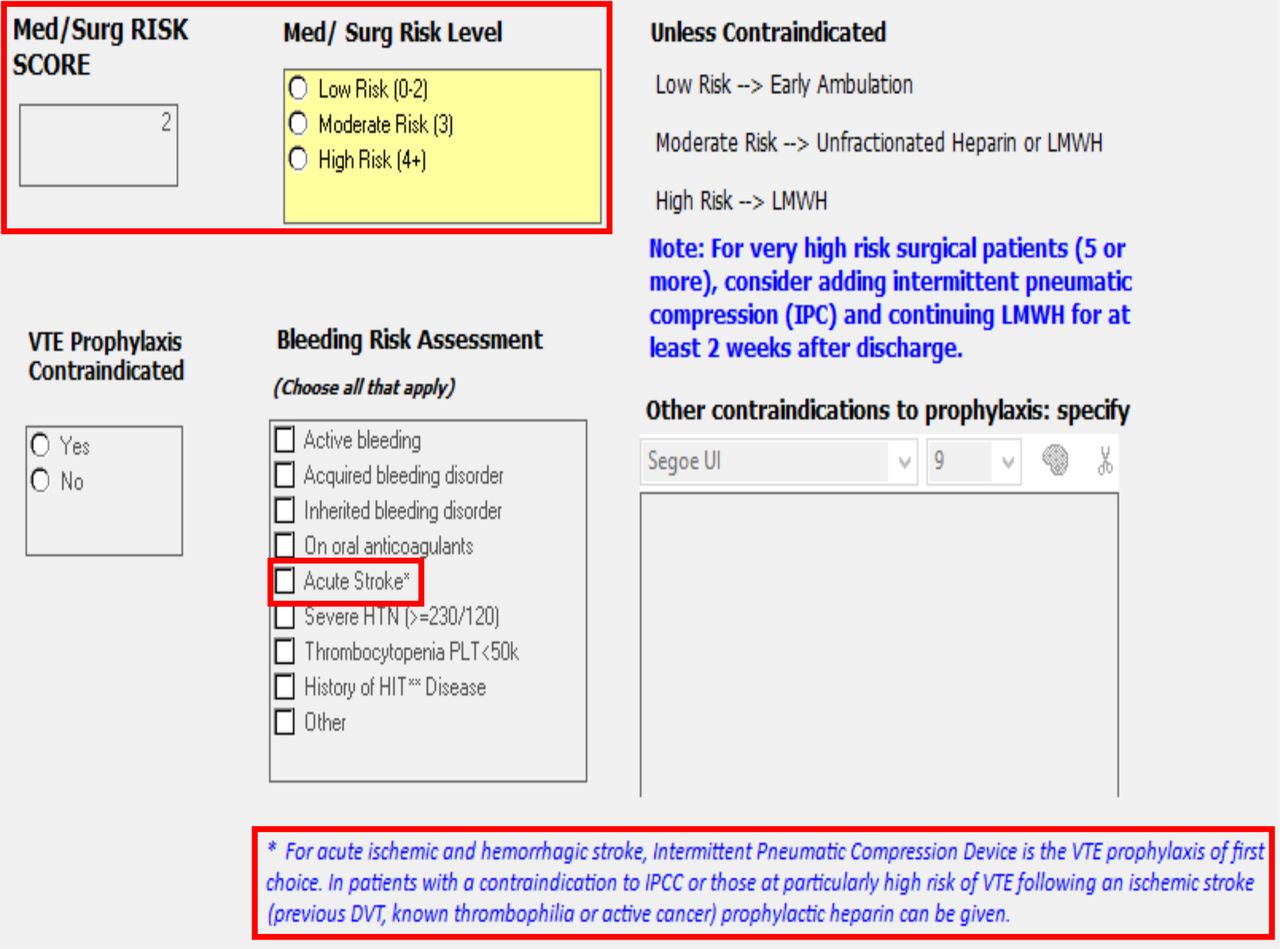
Health Informatics linked the VTE risk assessment tool to the VTE prophylaxis order (figure 6) and updated the VTE risk assessment tool to reflect new evidence-based medicine American Heart Association/American Stroke Association 2018 guidelines for VTE prophylaxis in acute ischaemic stroke7; in the VTE contraindication list, ‘acute haemorrhagic stroke’ was replaced with ‘acute stroke’ to include acute ischaemic stroke as well (figure 5). Those health informatics interventions improved VTE prophylaxis from 96% to 98%.

VTE Risk Assessment Score. DVT, Deep vein thrombosis; HIT, Heparin induced thrombocytopenia; HTN, Hypertension; LMWH, Low molecular weight heparin; PLT, Platelet; VTE venous thromboembolism.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Venous thromboembolism orders.
Results
With the implemented performance improvement interventions, there was remarkable improvement in the medical and surgical VTE prophylaxis rates from an average of 87% in July 2018 to above 98% in April 2019, and this improvement was sustained over the last 3 months of the study period April through June 2019.
Lessons and limitations
Health informatics and automation can play a key role in performance improvement projects. A limitation of this project is that it focused on the process measure VTE prophylaxis rate and did not include the outcome measure VTE rate.
Conclusion
The multidisciplinary VTE prophylaxis improvement taskforce managed to implement quality improvement interventions that resulted in significant improvement in VTE prophylaxis rate for admitted medical and surgical patients. Those interventions resulted in a remarkable improvement in medical and surgical VTE prophylaxis rates from an average of 87% in July 2018 to above 98% in April 2019, and this improvement was sustained over the last 3 months of the study period from April to June 2019. This performance improvement project shows that critical thinking and multidisciplinary team approach using information technology and collaboration between physicians, pharmacy, quality and health informatics can result in significant sustained performance improvement. The outcomes of the project and lessons learnt were shared throughout the organisation. Implemented interventions are generalisable and can be replicated in other wards and organisations.
Acknowledgments
Many thanks to SEHA Health Informatics and Quality team and Mafraq Hospital Quality Department, Pharmacy and Medicine and Surgical teams for their engagement and dedication.
Footnotes
Contributors HT participated in the brainstorming sessions and root cause analysis; provided education and training to physicians on proper VTE risk assessment tool documentation; planned the study, and prepared and submitted the study manuscript; was responsible for the overall content. EG participated in brainstorming sessions and root cause analysis, ran concurrent VTE prophylaxis report and shared the data with physicians in order to raise awareness, provided the VTE risk assessment and VTE prophylaxis run charts. FJ participated in brainstorming sessions and root cause analysis, ran concurrent VTE prophylaxis report and shared the data with physicians in order to raise awareness. GS participated in brainstorming sessions and root cause analysis, conducted a real-time audit with phone call physician reminders to place VTE prophylaxis order within 24 hours. BK participated in the brainstorming sessions and root cause analysis, changed the VTE prophylaxis trigger to physician-entered risk level instead of the previous tool-generated risk score. SK participated in the brainstorming sessions and root cause analysis, and linked the VTE risk assessment tool to the VTE prophylaxis order and updated the VTE risk assessment tool. WKH participated in brainstorming sessions and root cause analysis, provided education and training to physicians on proper VTE risk assessment tool documentation and participated in preparing the study manuscript.
Funding This study was funded by Mafraq hospital.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.