Article Text

Abstract
Background Improving transitions in care is a major focus of healthcare planning. The objective of this study was to determine the improvement in transitions from an intervention identifying complex older adult patients in acute care and supporting their discharge into the community.
Methods This was a quality assurance study evaluating an intervention on high-risk patients admitted in an acute care hospital. In phase 1, the Length of Stay, Acuity of the Admission, Charlson Comorbidity Index Score, and Emergency Department Use (LACE Index) was selected to assess a patient’s risk for readmission and a standard discharge protocol was developed. In phase 2, the intervention was implemented: (1) all patients were screened for the risk of readmission using the LACE Index; and (2) the high-risk patients were provided care coordination including follow-up phone calls focused on medications, equipment and homecare services. Emergency department (ED) revisits and hospital readmissions were measured.
Results The LACE Index identified 433/1621 (27%) patients at high risk for readmission. Care coordination was achieved within 72 hours in 79% of patients. The 433 high-risk patients receiving the intervention, compared with a group without intervention (n=231), had lower lengths of stay (12.7 days vs 16.6 days); similar 7-day ED revisits (10.6% vs 10.8%) and 30-day ED revisits (30.5% vs 33.3%); lower 90-day readmissions (39.3% vs 44.6%); and lower 6-month readmissions (50.9% vs 58.4%). The 7-day and 30-day readmissions were similar in both groups.
Conclusions Identifying complex patients at high risk for readmission and supporting them during transitions from acute care to home potentially decreases lengths of hospital stay and prevents short-term ED revisits and long-term readmissions.
- geriatrics
- health services research
- patient discharge
- transitions in care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The complexity of navigating the healthcare system, especially for older adults, makes a compelling case for coordinated hospital discharge practices to be linked with key community services to provide seamless care.1 2 When a patient is in the hospital, there are many measures in place to ensure they receive quality care. However, when a patient is discharged, less attention has been paid to the continuity and subsequent quality of care, despite the fact that hospitals are still responsible for making sure patients stay on the path to wellness outside the hospital.3 Thus, discharge and transitional planning are significant for seniors where inadequate practices can be linked to adverse outcomes. Without a coordinated provider approach, patients are at an increased risk for morbidity, longer lengths of stay, emergency department visits, and rehospitalisation.1 4 Readmissions are often preventable and are very costly to the healthcare system.5 6 As many as 20% of hospitalisations are due to readmissions within 30 days of discharge, frequently the result of ineffective communication among the acute and primary healthcare team and with the patient.7
Effective discharge planning should focus on enhancing, not inhibiting, current workflows. When it comes to postdischarge planning, there are many possible strategies. Interventions that focus on postdischarge phone calls have been proven to help with continuity of care, patient satisfaction, give patients an opportunity to ask questions about care, encourage necessary outpatient follow-up and prevent adverse events and readmission.6 8–12 It is crucial that these postdischarge planning strategies evaluate and implement ways of performing the most effective outreach to their unique patient population. There are many potential benefits that arise from follow-up with patients following discharge from hospital. For example, posthospital discharge follow-up helps to identify patients who might be at risk for an adverse event.13 Posthospital discharge follow-up also increases patient satisfaction and decreases the likelihood a patient will be readmitted.6 13 It has been documented that the first 48 hours are the most crucial time periods posthospital discharge to support successful health maintenance in the community.13
Patients are often overwhelmed following posthospital discharge. They often feel unprepared to translate knowledge of safe health practices into daily living, and many lack the necessary supports to ensure restoration and recovery.14–16 The current evidence indicates that hospital discharge and transition initiatives, such as Path to Home, have been shown to lead to improvements in outcomes if interventions include family members and caregivers, focus on patient education, develop opportunities for communication between healthcare professionals and family, and provide interdisciplinary communication, care planning and ongoing support after discharge.17 18 As such, accreditation standards support patient-centred care planning in transitions of care including assessment for risk of readmission.19
Interventions focused on transitions in care need to bridge the gap between the care provided in hospital and the support services needed in the community.1 20 21 Transitions in care interventions should provide a coordinated health professional approach that includes clear and transparent dissemination of information as well as active support for patients and their family members. The purpose of this study was to support coordinated transitions from acute care to the community setting for complex patients (predominantly seniors) at risk for readmission.
The study focused on promoting patient-centric, targeted discharge planning with intentional connections to community supports including primary care physicians and medical monitoring post discharge. This was accomplished through the development of an intervention for early identification of complex patients at risk for readmission through the introduction of a validated standardised assessment tool with the intention to reduce the potential for hospital readmissions or emergency department visits. The intervention provided mechanisms to improve the coordination of health services among providers across multiple sectors through targeted communications. The objective of this study was to determine the improvement in transitions from an intervention identifying complex older adult patients in acute care and supporting their discharge into the community. We hypothesised that addressing the gaps in transitions in care would result in reductions in length of stay (LOS) and readmissions. The uniqueness of our study is that many studies have concentrated on readmissions but not the impact on LOS.6 8 13 Our study addresses this need.
Methods
Study design and setting
This was a quality assurance study evaluating the outcomes of an intervention to improve transitions from acute care to home. The study was implemented in the Medicine Program at the Grey Nuns Hospital, an acute care hospital in Edmonton, Alberta, Canada. A multisector Transitions Steering Committee was tasked to improve on the transitions of patients at discharge. This Transitions Steering Committee consisted of stakeholders from acute care medicine and geriatrics, data and decision support, home living, transition services, supportive living, continuing care, and the primary care network (PCN). Phase 1 focused on the selection of the Length of Stay, Acuity of the Admission, Charlson Comorbidity Index Score, Emergency Department Use (LACE Index) to identify patients at risk for hospital readmission and to develop a discharge protocol (see online supplementary appendix 1 and 2).22 This selection was informed by literature review, steering committee input and presentations from outside sites using the LACE tool. In phase 2, all patients in the Medicine Program between September 2016 and June 2017 were included in the study, excluding those from facility living (long-term care), designated supportive living and those patients living outside of the region. Patients were not involved in the conception, design or review of the study. They were, however, part of the implementation.
Supplemental material
Supplemental material
Intervention
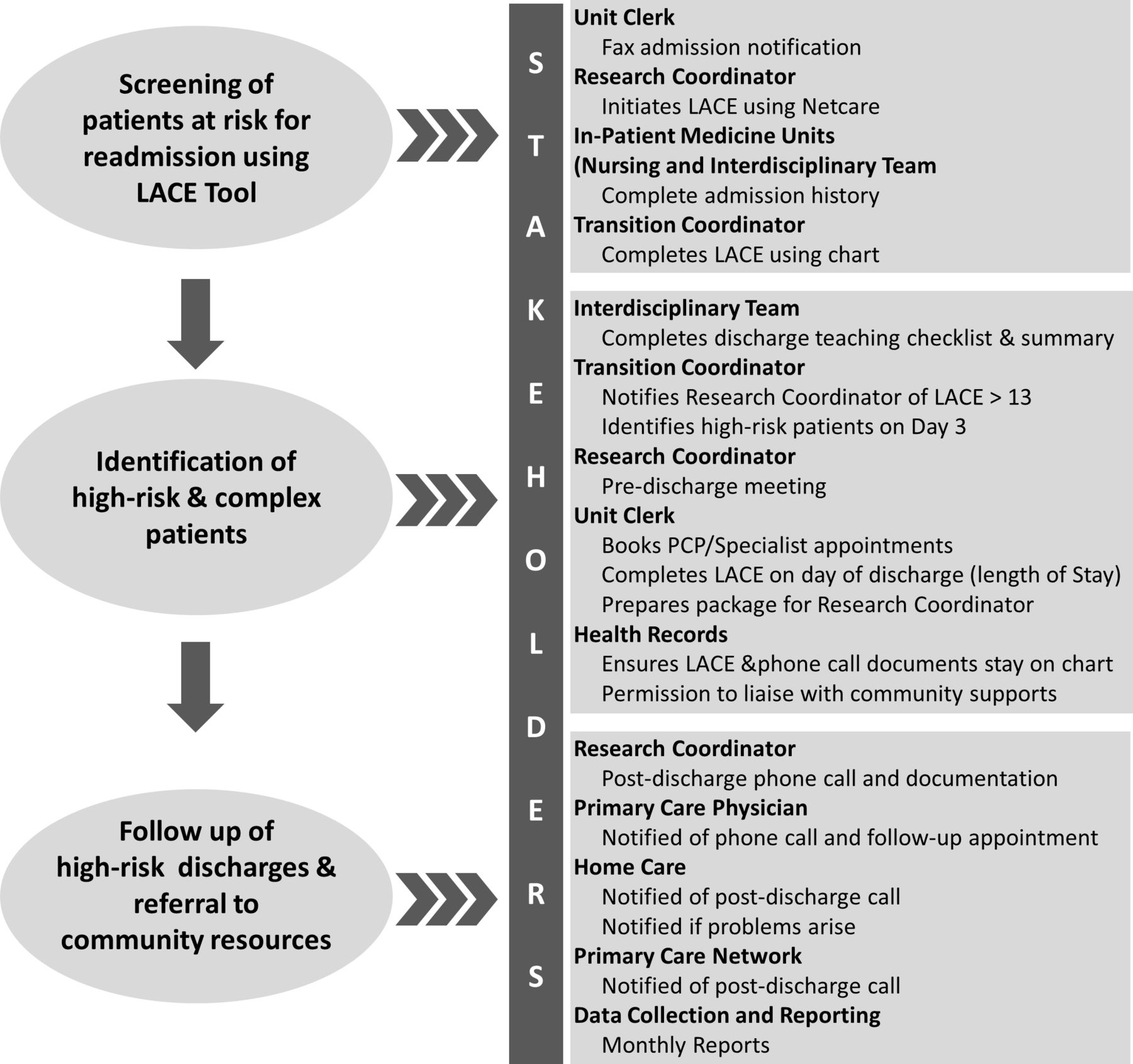
The intervention consisted of identifying patients at risk for readmission and providing these patients with care coordination after discharge. Each patient’s LACE Index was derived on the third admission day to identify potentially high-risk patients at discharge, omitting one variable (LOS). Patients with indexes of 10 or greater were classified as high risk. This score was documented on the chart and thereby alerted the team that the patient was at high risk for readmission. Again, on discharge, the LACE Index was obtained (now including LOS). Scores of 13 and greater were considered as being high risk for readmission. This is a validated tool to predict readmission.23 The high-risk patients were then provided with care coordination consisting of: (1) booking a follow-up appointment with the primary care physician (PCP) within a week of discharge and a (2) follow-up phone call (from the research coordinator) supporting the patient’s access or compliance to discharge instructions, medications, homecare, meals, equipment, follow-up appointments and satisfaction with discharge process. The research coordinator was a transition coordinator with a registered nursing degree and experience in discharge planning. She was trained on the LACE tool by a geriatrician and was part of the working group who developed the telephone call script. This script was also informed by literature review, steering committee input and a collation of scripts used by home living and outside sites. The research coordinator acted as a liaison between the patient and hospital, assuring the success of the transition. See figure 1 for a summary of the interventions and corresponding stakeholders.
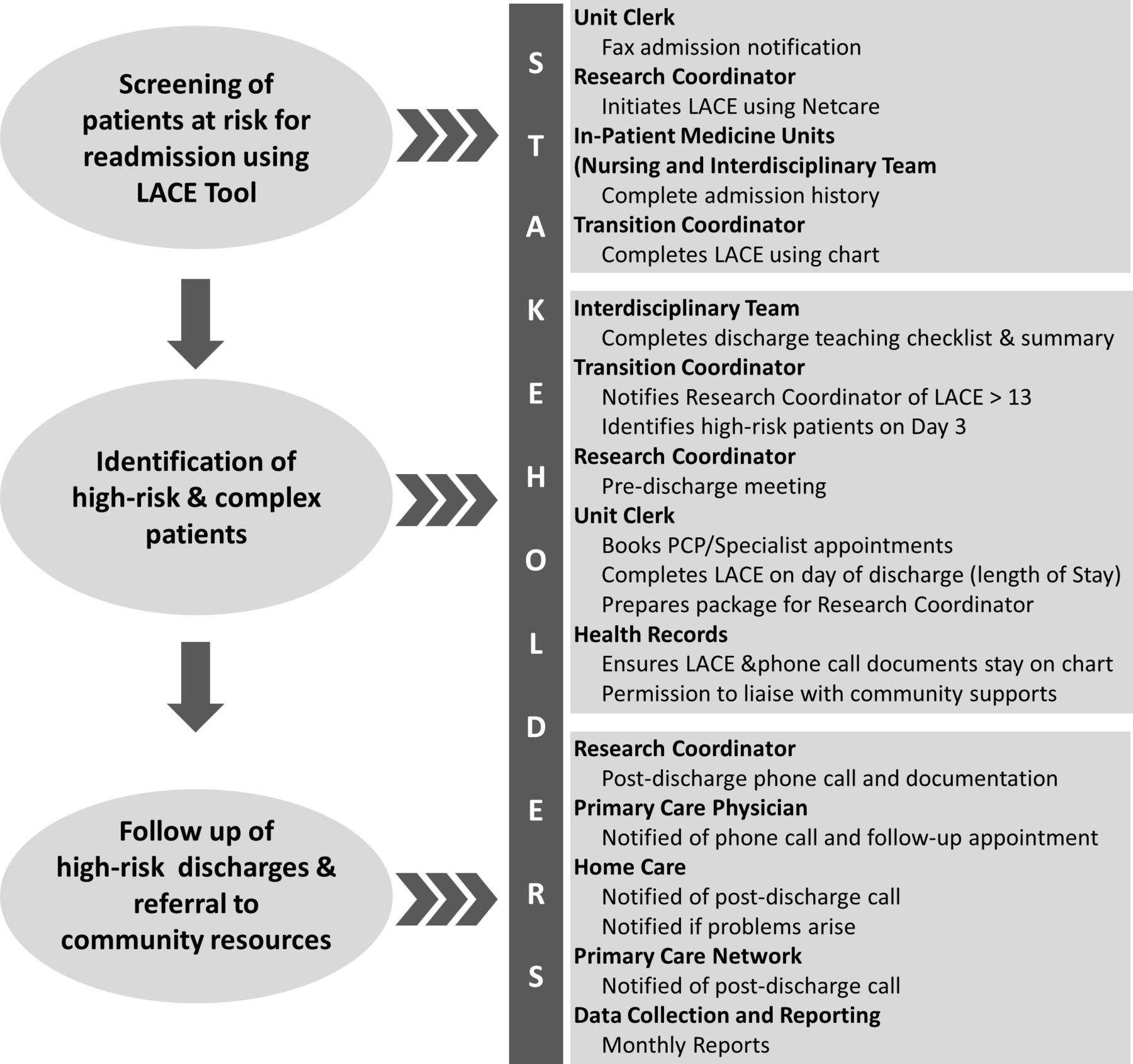
Interventions and stakeholders in the study. LACE, Length of Stay, Acuity of the Admission, Charlson Comorbidity Index Score, Emergency Department Use.
Outcome measures and analysis
An evaluation framework was developed to capture the following elements: improvements in the patient and family experience in care transitions from hospital to home; LOS in hospital; reduction in ED revisits at 7 and 30 days; reduction in hospital readmissions 7, 30, 90 days and 6 months; and improvements in coordination of health services among providers across multiple sectors through targeted communication. During the phone call, data were collected on whether or not the patient understood the discharge instructions, picked up their medications, attended a follow-up appointment with the primary care physician, and if applicable, if they received their equipment and/or connected with home care. Patients and their caregivers also were asked about their satisfaction with the intervention. Provincial databases were used to determine outcomes for the specific patient population receiving phone calls. Data were retrieved from information gathered during the phone call and from provincial databases (aggregate data only).
Data from a comparable group of high-risk patients (n=231), admitted from June 2017 to September 2017 but who did not receive the intervention, were collected. LACE scores were completed retrospectively after discharge. This group was from the same medicine units at the same hospital and acted as a control.
We used descriptive statistics to analyse the results. To compare the proportions between the two groups, we used z tests (Stata V.15.1).
Results
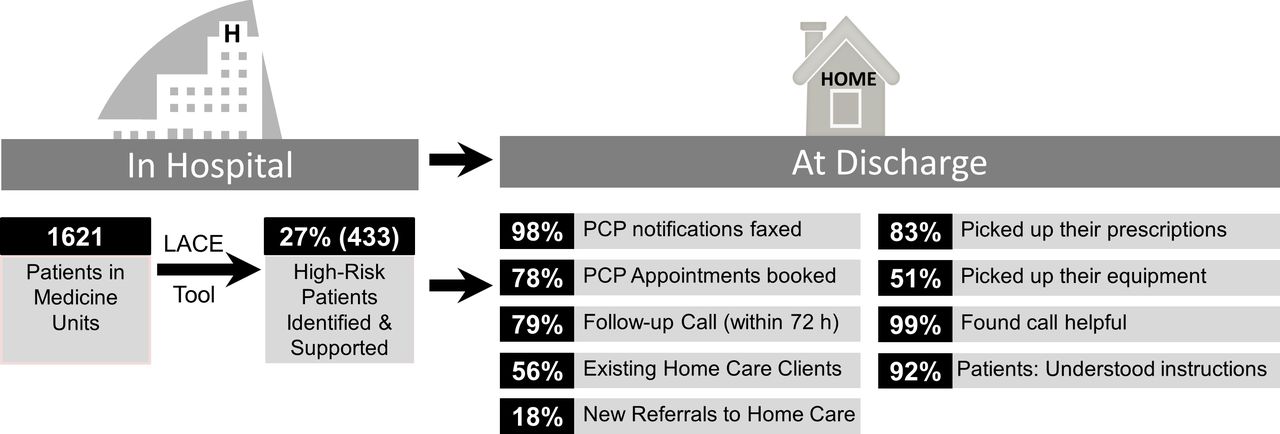
One thousand six hundred and twenty-one patients were discharged from medicine units in the hospital with a discharge disposition of home between September 2016 and June 2017. Four hundred and thirty-three patients (27%) were identified as high risk for readmission as assessed by a LACE score of ≥13.
Postdischarge phone calls
Eighty-three per cent (n=359) of the high-risk patients and/or their caregivers were successfully contacted through the follow-up call. Fifty-two per cent (52%; n=186) of these follow-up phone calls were made with the patient and 48% (n=172) were made with the patients’ caregivers. Ninety-seven per cent (97%; n=420) of these patients received a first call within the first 3 days of discharge, of which successful contact was made with 79% (n=342). In addition, 99% (n=355) of patients and caregivers indicated they found the follow-up phone call helpful.
When asked whether or not they understood the discharge instructions, 93% (n=173) of patients and 92% (n=158) of caregivers indicated they had a good understanding of the discharge instructions (see figure 2). Eighty-three per cent (83%; n=298) of patients and their caregivers had filled their prescriptions and 51% (n=183) of patients and their caregivers picked up equipment. The notification of discharge was faxed to 98% (n=424) of primary care providers. Seventy-seven per cent (77%; n=333) of the patients identified as high-risk for readmission belonged to a PCN. The unit clerk was able to book appointments for patients with their primary care providers for 45% (n=195) of patients prior to discharge from hospital. A total of 78% (n=338) of patients had booked follow-up appointments with their primary care provider or a specialist, with these appointments made either by the unit clerk or independently by patients or their caregivers. Of the 433 patients called, 74% (n=320) of patient had home care involvement, 18% (n=78) were new home care clients and 56% (n=242) were existing home care clients. The remaining 26% (n=113) of patients had no home care involvement. In addition, 6% (n=24) of the patients had a systems case manager involved in their discharge care.
{kind=link}
{kind=link}
Infographic of outcomes at discharge. LACE, Length of Stay, Acuity of the Admission, Charlson Comorbidity Index Score, Emergency Department Use.
ED visits and readmissions
The average LOS was shorter in the intervention group (12.7 days) than the comparison group (16.6 days). In terms of ED revisits, the proportions were similar between the two groups at 7 days (10.6% vs 10.8%; see table 1) as well as at 30 days (30.5% vs 33.3%). The intervention group had lower readmissions at 90 days (39.3% vs 44.6%) and 6 months (50.9% vs 58.4%). The 7-day and 30-day readmissions were similar in both groups though were slightly lower in the control group. None of the differences reached statistical significance.
Outcomes with and without the intervention
Discussion
With an increasing population, longer life expectancy, an increase in chronic conditions and advancing medical care, the healthcare system is becoming increasingly difficult to navigate, especially for seniors. This is because seniors often have more complex medical problems, longer LOS and higher acute care use which may result in readmission if the discharge is not well supported.24 These characteristics dictate that the majority of patients identified as complex and high risk will be seniors. Enabling seniors to remain at home as long as possible, while maintaining their safety and independence, is of great importance, both to maintain the patient’s quality of life and to exercise allocation of stretched hospital resources.25 The goal is that seniors will continue to remain healthy at home for longer, with less acute care utilisation. This study aimed to achieve this goal by connecting patients at high risk for hospital readmission to existing community supports. This process is especially important for isolated seniors that do not know what resources are available and how to access them. The hospital admission and discharge processes are usually busy, rushed and emotional. By providing follow-up shortly after discharge, once the patient is settled at home, the patient and caregiver have a better perspective on gaps in their care needs.20
Our research indicates that the use of a follow-up phone call as part of the intervention identifies that there is a problem with patients picking up equipment. Ongoing liaison with equipment suppliers within the community is helping to mitigate this. Despite this challenge, patients overall were satisfied with the intervention and it was clear that patients understood their discharge instructions and that discharge from hospital was well coordinated in large part due to the implementation of the Path to Home model.17 Our research study has demonstrated that having LACE Index scores on the chart highlights the complexity of patients to the interdisciplinary team and has decreased LOS by an average of 4 days, which is clinically significant. It appears that the care team being alerted on day 3 to a complex patient may have led to this reduction through focused care planning and communication. Despite the decreased LOS in our study, short-term ED revisits and readmissions were not increased. With respect to the impact of phone calls, in the short term, the phone call did not seem to have an impact on reductions in readmission, but in the long term may have. There may be many factors that contribute to a lack of positive impact on readmission in the short term including the multifactorial nature of readmission risk factors such as medical complexities with multiple diagnoses, the need for higher level of care for a number of these patients but not being able to support this level of care in the home, and/or patients being readmitted for a different medical problem. In our study, a deep dive into the short-term ED visits revealed mainly cancer diagnoses or attendance for a separate medical issue to the first visit. Other studies have shown better discharge support but not decreased LOS.6 8 13
Key learnings from the study are that patients found the intervention helpful, understood their discharge instructions, and despite shorter LOS, had no increased readmissions. Overall, the feasibility and sustainability of the intervention over time appear promising. Most of the aspects of this innovation are sustainable in that many of the resources and modifications are currently in practice. However, there are opportunities in the system to automate and integrate the LACE Index. The LACE Index that we have adopted is relatively quick and easy to complete by members of the care team, and its results can be used in a number of ways. The study used the LACE Index score to identify patients as complex and at high risk for readmission, which alerted the care team on day 3 to start complex discharge planning. The LACE Index score also alerted the unit clerk to book a follow-up appointment with the primary care physician. However, the Care Team, either in acute care or in the community, needs to take over the research coordinator’s role to make the follow-up phone call. There are further opportunities for cohesive discharge planning to occur for these patients with the local PCNs and homecare as partners in this innovation and work is already underway to spread this concept. One common theme, for example, there is a lack of understanding of medications immediately after discharge, and incomplete processes in sharing information with primary care providers and community pharmacies. A potential area of continuation and further development is around medications. A high LACE score could be used to alert the Care Team to provide more comprehensive discharge planning and explanations of medications prior to discharge. This would require the involvement of a nurse or pharmacist with the discharge phone call.
Limitations
This study was done to improve transitions in the patients admitted to the medicine programme. Budgetary limitations precluded the study’s spread to other departments. Also, for ethical reasons, the study could not create a comparison group (ie, withholding the intervention) from the group of medicine patients. Barring logistical limitations, a more robust comparison group could have been established from other departments. Use of the LACE Index had the most impact in reducing LOS, with little impact on ED visits/readmissions. Performing the LACE Index is sustainable and ongoing since the results of the difference in LOS were available. Going forward, the transitions steering committee has liaised with the PCNs to continue the follow-up phone call.
Conclusion
Identifying complex patients at high risk for readmission and supporting these patients during transitions from acute care to home potentially decrease lengths of hospital stay and prevent long-term readmissions. However, the use of the LACE Index had little effect on ED visits 7 days and 30 days after discharge, and 7-day and 30-day inpatient readmissions despite the decreased LOS. The intervention also brought various stakeholders together to solve a complex problem. This created a better understanding of system challenges and key roles that each play in supporting the patient’s health journey. Patient transitions are a well-known area of health systems improvement and remain a rich area for further research.
References
Footnotes
Contributors LC and LJ contributed substantially to the conception and design, acquisition of data, analysis, interpretation of data, review/revision of the manuscript and provided final approval of the version to be published. They are the responsible for the overall content as guarantors. JMIT drafted and revised the manuscript and provided final approval of the version to be published. JP contributed to the conception and design of the study, interpretation of data, review/revision of the manuscript and provided final approval of the version to be published. BD and PGJT contributed to the interpretation of data, reviewed/revised the manuscript and provided final approval of the version to be published.
Funding This study received an Innovation Grant ($200 000) from the Covenant Health–Network of Excellence in Seniors Health and Wellness, Edmonton, Alberta.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval This study was deemed to be outside the mandate of the Health Research Ethics Board of the University of Alberta (Study ID # Pro00062100) and did not require ethics review.
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement Data are available upon reasonable request. Data may be requested from Covenant Health.