Article Text

Abstract
Aim Intrahospital transportation (IHT) of patients under mechanical ventilation (MV) significantly increases the risk of patient harm. A structured process performed by a well-prepared team with adequate communication among team members plays a vital role in enhancing patient safety during transportation.
Design and implementation We conducted this quality improvement programme at the intensive care units of a university-affiliated medical centre, focusing on the care of patients under MV who received IHT for CT or MRI examinations. With the interventions based on the analysis finding of the IHT process by healthcare failure mode and effects analysis, we developed and implemented strategies to improve this process, including standardisation of the transportation process, enhancing equipment maintenance and strengthening the teamwork among the transportation teammates. In a subsequent cycle, we developed and implemented a new process with the practice of reminder-assisted briefing. The reminders were printed on cards with mnemonics including ‘VITAL’ (Vital signs, Infusions, Tubes, Alarms and Leave) attached to the transportation monitors for the intensive care unit nurses, ‘STOP’ (Secretions, Tubes, Oxygen and Power) attached to the transportation ventilators for the respiratory therapists and ‘STOP’ (Speak-out, Tubes, Others and Position) attached to the examination equipment for the radiology technicians. We compared the incidence of adverse events and completeness and correctness of the tasks deemed to be essential for effective teamwork before and after implementing the programme.
Results The implementation of the programme significantly reduced the number and incidence of adverse events (1.08% vs 0.23%, p=0.01). Audits also showed improved teamwork during transportation as the team members showed increased completeness and correctness of the essential IHT tasks (80.8% vs 96.5%, p<0.001).
Conclusion The implementation of reminder-assisted briefings significantly enhanced patient safety and teamwork behaviours during the IHT of mechanically ventilated patients with critical illness.
- critical care
- patient safety
- respite care
- team training
- transportation of patients
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
The National Taiwan University Hospital is a university-affiliated medical centre in Taiwan consisting of 2300 beds, including 161 adult intensive care unit (ICU) beds. An emerging issue was the safety during the intrahospital transportations (IHT) of patients with critical illness performed approximately 1000 annually. In 2015, it was brought to our attention that various types of adverse events occurred during IHT, including two cases of cardiopulmonary arrest requiring emergent resuscitation, and other cases of unstable vital signs requiring emergent care (online supplementary table 1S), demonstrating the high impact on the patients. Multiple potential weaknesses of the IHT process required a detailed examination, as the proximate cause of these events may have involved various personnel such as physicians, nurses, respiratory therapists, technicians and administrative staff. To better address these issues, we decided to implement an improvement programme with a proactive approach using healthcare failure mode and effects analysis (HFMEA),1 which explores the whole process and identifies weak points and opportunities for improving the safety of the process.
Supplemental material
The Centre for Quality Improvement of the hospital called for the establishment of a team to conduct an improvement programme. The team gathered, discussed and decided to apply HFMEA to generate interventions because IHT has several features, including multiple departments involving in transportation, concerns of unexplored processes, face-to-face communication and collaboration, and mechanically ventilated patients with high risk for serious adverse events (table 1).
Steps of HFMEA and persons selected to participate in this programme*
Our specific aims were to analyse the process of IHT by applying HFMEA to generate improvement strategies for IHT for mechanically ventilated patients.
The following Specific, Measurable, Attainable, Relevant, Time-based objectives were then conceived:
To increase the completeness and correctness of the essential IHT tasks to higher than 95% through an actionable reminder-based briefing process during the IHT process for mechanically ventilated patients with critical illness.
To reduce the incidence of adverse events with patient harm to lower than 0.5% during IHT.
Background
IHT, defined as the movement of a patient from one physical location within the hospital to another,2 is one of the most frequently performed tasks for caring hospitalised patients.3 It is particularly challenging as the patients move to an environment with changed care setting,4 5 which carries the potential risk of adverse events,6 7 such as deterioration of physiological parameters,8 malfunctioning of equipment and facilities, and displacement and malfunctioning of tubes and lines.9 The contributing human failures might include incorrect operation of instruments and equipment or failing to comply with standards.10 11 Patients under mechanical ventilation (MV) are among the high-risk population for IHT,12 with reported worsening of respiratory and other essential organ functions.13 The MV requires additional staff such as respiratory therapists; however, their specialty care and operation of the ventilator are not part of the routine work of the staff at the bedside. Preventing adverse events related to IHT is challenging,14 and researches have focused on elucidating the underlying causes.15
In a typical IHT session for mechanically ventilated patients in this hospital, the healthcare workers confirm the transportation need for an examination or intervention. The workers then assemble personnel and prepare equipment, including a portable ventilator, oxygen, monitors, medications and additional helpers to form a transportation team. After arrival at the destination, there is a handoff process with documentation of the patient’s condition on the transportation sheet and the transfer of the patient to the examination table. The examination room staff perform the planned task, carefully monitoring and providing treatment as required. After the examination, the staff members are summoned, and the transportation team is reassembled to return the patient to the primary venue.
According to the studies referenced above, IHT may be an essential priority for a proactive improvement project in terms of patient safety and adverse events. However, publications providing experience from peers, and especially those involved in detailed examinations of the transportation process to reduce patient risk, are lacking. Therefore, we decided to explore the safety issues related to IHT.
Measurement
The whole span of process and outcome measurements included the preimplementation phase from January to December 2015, the implementation phase from January to December 2016 and the postimplementation phase from January to December 2017.
The process measurements were performed by randomly assigned respiratory therapists who participated in the IHT session from 12 ICUs for CT and MRI examinations. Shortly after completion of IHT session, the respiratory therapist was provided with a checklist-type assessment worksheet, which consisted of 16 items regarding the completeness and correctness of IHT tasks (table 2), to assess the observable practice during IHT. These participating respiratory therapists had all received education and training to assess the completeness and behaviour of the transportation team members. Selection of the cases for auditing was the convenient sampling approach when the investigators knew when the transportations took place and were able to provide the worksheet for auditing immediately after the transportation. The audits were performed from October 2015 to March 2017 and consisted of 14, 72 and 33 sessions in the preimplementation, implementation and postimplementation phases, respectively.
Mnemonics and descriptions applied for the reminder-assisted briefing during the intrahospital transportation process
For the outcome measures, the team calculated the adverse events reported to the incident reporting system of the hospital from January 2015 to December 2017. Data collected also included the IHT sessions and clinical data of patients. Based on the literature, a patient safety event was defined as an unexpected or unintended event, which could have led to or did result in harm to the involved patient. An adverse event was defined as an injury caused during the healthcare process rather than by the underlying disease or condition of the patient.16–19 Furthermore, for a control chart for IHT-related adverse events, we used a g-chart in statistical process control analysis, as the incidence of reported events regarding this process was rare20; baseline preimplementation of this programme showed an incidence of 1.08%.
For statistical analysis, quantitative variables are expressed as count (percentage) for categorical variables and mean with SD for continuous variables. The statistical significance of comparisons of proportions was assessed using the χ2 test or Fisher’s exact test for crosstabs. A p value <0.05 was considered to be statistically significant.
Design
The interventions were based on HFMEA to explore weak points in the process of IHT and to develop actionable strategies because the subprocesses of IHT in this setting were linked as the patients moved between locations. The HFMEA had never been applied to IHT process before this improvement programme. Still, conventional analysis and improvement process in the institutional incident reporting system was considered not enough to reinforce the weakness.
In the first part of HFMEA, analysis of the process was conducted, and table 1 summarises the steps, descriptions and the persons selected to participate in the steps according to the literature.1 HFMEA was modified from traditional FMEA,21 22 with main changes being eliminating the likelihood of detection, and calculating risk priority number only by severity times probability, with the application of decision tree analysis.1 HFMEA is a useful tool23 and has been increasingly applied to risk management in healthcare settings24–29; an expanded version has also been suggested.30 However, few studies have applied HFMEA to the transportation of patients with critical illness. On the other hand, the use of a checklist to enhance safety in patient transportation has been suggested,31–33 but no studies reported the use of HFMEA to generate such a checklist. Therefore, the team decided that HFMEA should be the first part of the analysis, while the checklist serves as the output of strategy backed up by HFMEA results.
Team participators included three respiratory therapists, an ICU nursing supervisor, an ICU head nurse, a nurse from surgical ICU, a supervisor of radiology technicians, a staff member and a supervisor from Centre for Quality Management and a critical care physician. The director of the Centre for Quality Management approved this programme. Anticipated problems encountered included the variation of IHT process across different ICUs, need for time to practise standardised tasks and policies not supporting further documentation of the routine checking about safety tasks. The team planned to implement strategies considered likely to be sustainable, such as repeated staff education with training videos available online, random audits and reminding mechanisms visually available in the environment related to IHT.
Strategy
The team applied HFMEA methodology as previously described,1 with pertinent spreadsheets, scoring instructions and algorithms adopted from sources all publicly available on the internet. The table shows the adopted template1 used in this programme (see online supplementary file 2). The IHT included five main processes, and the spreadsheet shows main processes, subprocesses, failure modes, causes of failure, effects, risk assessment, the decision on correction, actions and reassessment of risk for the process of IHT during the HFMEA process of this programme (see online supplementary file 2).
Supplemental material
A total of 64 failure modes were found in the whole process, including 25 in the preparation of transportation, 10 in care and monitoring during transportation, 13 in arrival at the examination unit, 10 in transportation back to ICU and 6 in arrival at ICU bed. These failures had 112 failure causes and 132 effects, and the sum of risk priority number was 939. The team determined that 71 of the effects require corrective actions, including 35 actions to ‘eliminate’ the failure modes and 36 to ‘control’ failures, with none to ‘mitigate’ failures. Hazard analysis iterated 26 modes with potential causes meeting the criteria for taking actions. A summary of the worksheet for this HFMEA is provided in online supplementary table 2S. Aiming to limit the HFMEA to a more manageable scope, three strategies were addressed by consensus on the priority of the strategies: development and implementation of a reminder-assisted briefing method, standardisation of IHT process and establishment of routine checking process for equipment and facilities related to IHT. Detailed descriptions of the three strategies are summarised in online supplementary table 3S.
During preimplementation phase, the team held eight meetings, spending 66.0±6.2 min and eight persons per meeting. Eight meetings were conducted in implementation phase, spending 66.3±24.1 min and 13 persons per session, whereas the seven meetings spent 43.6±5.8 min and seven persons per session in postimplementation phase. Overall, 14 nurses, 6 physicians, 8 respiratory therapists, 3 radiology technicians, 4 members of staff from the quality centre and 7 from other units participated in meetings. After the provision of improvement strategies, the risk priority number was calculated again, showing a reduction from 939 to 411 points, with a reduction of more than 50% indicating the feasibility of the planned corrective actions.
The team reviewed and revised IHT processes during the first improvement cycle from January to March 2016. A description of role and position of members of transportation team was provided to ensure the workers in right positions and fulfilled designated roles during transportation. The maintenance department discussed the documentation and actively checked for potential malfunctioning of the transportation equipment. The members collaborated to generate educational materials to enhance the knowledge, skills and attitude of the workers. The team found the main barrier in adhering to standardised IHT process was the lack of time for desired subprocesses and difficulty in memorising tasks. Our discussion then focused mainly on the need for a briefing process.
Agreements in the modification of IHT process prompted the establishment of three reminder-assisted briefings regarded as ‘time-out’ mechanisms. Emphases put on interactions among IHT team leader, respiratory therapist and ICU nurse at the ICU were discussed, as well as the interaction among IHT team leader, radiology technician and IHT team members. The ‘time-out’ sessions were assigned the mnemonics of ‘STOP’ (Secretions, Tubes, Oxygen and Power), ‘VITAL’ (Vital signs, Infusions, Tubes, Alarms and Leave) and ‘STOP’ (Speak-out, Tubes, Others and Position), respectively. Table 2 summarises the mnemonics of the reminders for structured briefings, content of essential tasks and persons required to conduct the tasks. Patients were always transported on ICU bed, displaced to examination table and then replaced to ICU bed after examination, and transported back to ICU. The reminder-assisted briefing used a printed card attached to the equipment or chart displaying essential tasks needed to be completed correctly during IHT.
To implement improvement strategies, we produced materials for training courses, including videos describing new processes for standardised IHT process, the use of reminder-assisted checklist briefing based on mnemonics and emphasis on teamwork culture. Educational materials were developed by participating members from ICUs, respiratory therapy and radiology department. The team organised education and training sessions, recruiting participants from ICUs, respiratory therapy unit and radiology, to teach and practise the reminder-assisted checklist briefing. The participants also provided feedback to training team. Titles of the videos included ‘Safety in the intra-hospital transportation of patients under mechanical ventilation’, ‘Scenarios of intra-hospital transportation with patient safety issues’ and ‘Introduction of team resource management and measures to improve teamwork’. These videos, 1 hour for each session, were provided to 13 ICUs, the radiology department and the respiratory therapy between 1 December and 31 December 2015. A total of 507 healthcare workers participated in 16 educational sessions, with 88.0% considering beneficial to their practice, and 88.7% satisfied with the course.
The patients or the public were not involved in the design, conduct, reporting or dissemination plans of our research.
Results
The analysis period spanned from January 2015 to December 2017, with 8014 annual admissions to the ICU and 55 239 patient-days. The average number of IHT sessions for MV was 1153 annually. Table 3 summarises the audit results of IHT sessions in the three phases, showing marked improvement of completeness of reminder-assisted briefings after the briefing implemented. Audits for IHT sessions by convenient sampling from participating ICUs also showed markedly improved compliance rate (p<0.001).
Process and outcome measurements for intrahospital transportation
During the implementation phase, there were three cases of adverse events with patient harm, including one with cardiopulmonary arrest, one with incorrect operation of an infusion pump resulting in unstable vital signs and one with incomplete preparation tasks resulting in delayed transportation. During the postimplementation phase, two events with patient harm were reported, including one with insufficient oxygen during transportation, and another with inadvertent removal of central line (online supplementary table 1S). Table 3 summarises the comparisons of adverse events with patient harm in the three phases, showing reduced incidence in the implementation phase compared with preimplementation in terms of either event per IHT session (0.23% vs 10.8%, p=0.010) or event per ICU admission (0.04% vs 0.14%, p=0.027). Further decreases in event rate were also noted in the postimplementation phase (table 3).
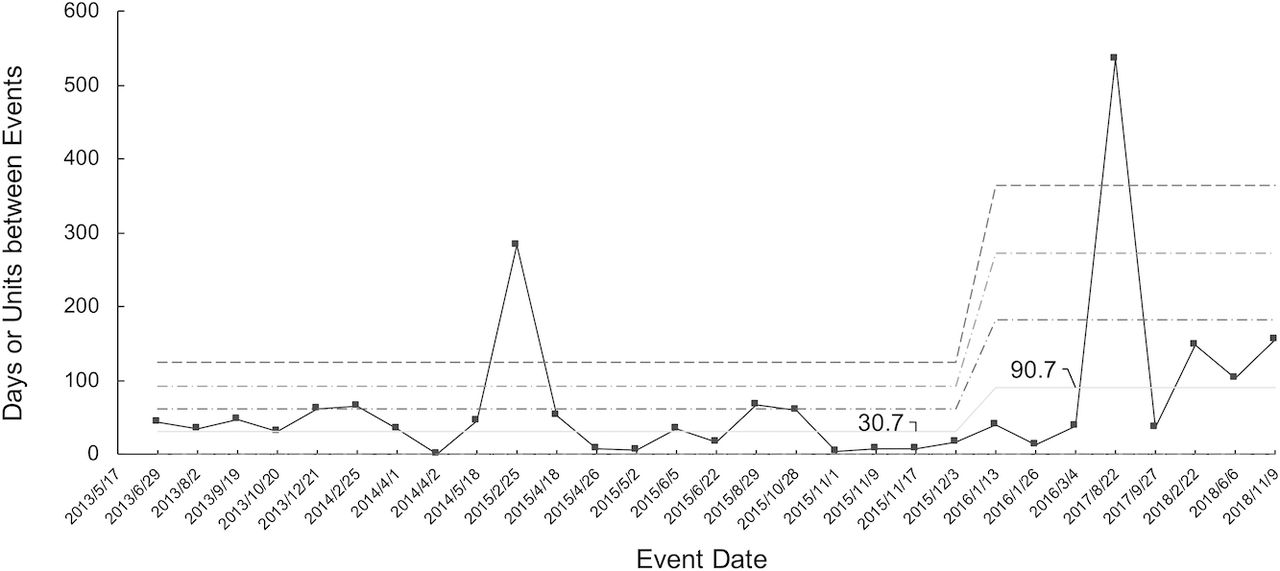
Figure 1 illustrates the g-chart in statistical process control, showing the programme tended to improve for the incidence of reported adverse events from January 2013 to December 2018, with 1 January 2016 as the interruption point. The figure shows significant prolongation of the interval between each reported event, from 30.7 days on average before implementation to 90.7 days after implementation.
{kind=link}
The g-chart of adverse events related to intrahospital transportation of mechanically ventilated patients.
For time-out sessions, the time spent by respiratory therapists (for ‘STOP’) was 28.1±6.3 s (n=14), 20.1±4.4 s (n=20) and 13.4±3.1 s (n=20) during the three phases, respectively, with a shorter time in the postimplementation phase compared with the preimplementation phase (p<0.001). The time spent by ICU nurses (for ‘VITAL’) was 41.6±10.9 s (n=14), 34.5±10.8 s (n=20) and 27.1±9.9 s (n=20), respectively, shorter in postimplementation (p<0.001). The time spent by radiology technicians at examination room (for ‘STOP’) was 39.3±12.7 s (n=14), 36.7±10.7 s (n=20) and 25.8±10.3 s (n=20), respectively, also shorter in postimplementation phase (p=0.002). No unintended consequence was identified, such as increased turnover rate of healthcare workers in the units, increased internal complaints or opinions, increased cancellation of CT or MRI examinations or increase of complaints from patients or families.
Lessons and limitations
In this report, we provided the processes and results of HFMEA for IHT of mechanically ventilated patients who underwent CT or MRI examinations, and improvement in process and outcome measurements. We evaluated possible systematic errors and showed that regular team reminder-assisted briefing was feasible, with positively perceived effects on patient safety. The strength of this programme was the application of HFMEA method combined with implementation of a reminder-assisted briefing as the principal improvement strategy.
During this programme spanning several years, we found the IHT process carries a high risk for compromising patient safety; this was compatible with previous findings.6 7 The failure modes we identified highlighted potential effects consistent with previously reported adverse events.8 9 13 As IHT is a high-volume process with more than 5000 sessions for ICU patients and more than 1000 for ventilated patients, our methods of analysis and strategies might provide useful information for hospitals with similar need for IHT.
HFMEA in healthcare domain has recently been advocated,1 and the use of checklist has become popularly implemented worldwide to improve patient safety, such as surgical operations,34 35 specifically to improve the process of IHT.31 32 Few studies have investigated HFMEA to enhance safety in the IHT of patients under MV, despite preventive programmes reported.36 The application of HFMEA also highlighted additional risks by identifying more failure modes in the process, in addition to a variety of reported unexpected incidents.3 Therefore, we recommend that healthcare institutions adopt HFMEA or similar proactive techniques to examine related processes.
The orally performed reminder-assisted briefings in this programme deserve emphasis. While checklists have been advocated for surgical operations37 and transportation of patients with critical illness,32 to the best of our knowledge, few studies have combined a checklist and oral briefing into a reminder-assisted briefing within a transportation team. Reports suggested the use of briefing checklist technique for emergency medicine handoffs38 and resuscitation during interhospital transportation39; well-prepared transportations using briefing strategies,40 however, rely on memorised and independent tasks of the individuals participating in transportation. Our findings suggest that a pause in IHT process with team briefing based on a structured checklist as reminder can promote communication skills and create commitment to improving communication among healthcare workers while limiting resource expenditure and loss during transportation. Waiving the need to complete a written checklist form also reduces the workload and time.
The programme suggested significant implications for hospital personnel and systems, including proactive analysis and reducing risks, and teamwork-based reminders with briefings. Potential difficulties, however, can be encountered, such as reluctance to change workflow and unwillingness for face-to-face briefings. Compliance with a safety checklist can be suboptimal due to various human conditions,41 while meaningful compliance can also be a concern42 due to barriers.43 To address this issue, a team may need to emphasise implementing science44 and a culture of safety, such as teamwork45; several crucial success factors for the implementation of quality improvement strategies have been suggested.46
There are limitations to this programme. First, similar to most improvement programmes, ours implemented more than one strategy. To validate the effectiveness of reminder-based briefings, a programme testing a single intervention is necessary. Second, it was not feasible to audit the tasks conducted in all IHT sessions, especially those during off-hours because of limited human resources. Although the selection of the cases for auditing was the convenient sampling approach, the numbers of auditing were not the same during the three phases of the programme. This was because the timing of IHT was mostly determined by the examination rooms according to the real-time patient flow that investigators might not know the time transportations took place and thus might not provide the auditing worksheet to the respiratory therapist immediately after the transportation, especially during the hours the investigators were also not available. Long-term selected audits are warranted. Third, healthcare workers may not have reported, or even perceived, the occurrence of events during IHT, especially those deemed predictable physiological changes in patients with critical illness. Fourth, this programme focused on a small proportion of diagnostic and interventional procedures requiring IHT; therefore, hospital-wide generalisability requires further investigation. Fifth, the cost and burden of implementing strategies were not measured; for sustainability, further evaluation of the value of this implementation is needed. Sixth, the before-after design carried an inherited limitation related to non-randomisation, while comparisons including other factors require prospective data collection with a more significant number of cases. Finally, the HFMEA tool can be difficult for healthcare workers and managerial who are not familiar and inexperienced with the actual process of the analysis. While the validity and usability of HFMEA in the identification of potential risks and translation into enhanced safety are still under debate,47 48 recommendations for implementation49 and modifications of this tool have also been suggested.30 50
Conclusion
The application of HFMEA for the IHT of mechanically ventilated patients may identify and prioritise potential risks that may have compromised the safety of patients; implementing briefings may significantly reduce the number of adverse events. Reminder-based briefings help conduct essential tasks without excessive burden. We found optimal results in process and outcome measurements, and therefore we recommend the implementation of a comprehensive exploration of similar processes and the application of reminder-based briefings. Further understanding of the burden added to the workers and reduced attention of the person caring for other patients requires investigation.
Sustainability depends on the feasibility of the practice to complete safety tasks before and during IHT. The use of reminder-based briefings may provide a higher probability of sustained adherence to the structured process. Further development of electronic checklists containing the reminder items to alert the workers will be considered. We also hope to implement our strategy institution-wide to achieve a higher level of patient safety in similar settings.
Acknowledgments
The authors thank Pao-Yu Chuang, nursing supervisor, Department of Nursing, National Taiwan University Hospital, for her kind assistance in this study and the implementation. The authors also thank Mei-Yu Chen, Yen-Wen Yung, Shu-Mei Liu, Hsiu-O Kao, Wen-Hsia Lin, Chiung-Hua Cheng, Shih-Ting Liu, Hsiu-Hua Lin, Shin-Tsyr Hwang and Shiao-Pei Wang, head nurses of the ICUs of National Taiwan University Hospital, for their kind assistance with the implementation of the interventions. The authors thank Hsiao-Fang Huang, Centre for Quality Management, National Taiwan University Hospital, for her kind assistance with data management.
References
Footnotes
Twitter @joey
Contributors SJL, CYT, MYS, LCC and JSJ planned the study. SJL, CYT, MYS, CLW, LCC, HJH, WLH, JCC, YWK and JSJ participated in the generation of improvement strategies and methods. SJL, MYS, CLW, HJH, WLH and JCC directed the implementation of improvement strategies. SJL, CLW, HJH and WLH carried out the audits. SJL, CLW, LCC, HJH, WLH and JCC collected the data. SJL, LCC and JSJ analysed the data. CYT, JSJ, HDW and JSS supervised the improvement programme and study. SJL and YWK wrote the draft of the manuscript. JSJ and HDW revised and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval The Institutional Research Ethics Committee of our hospital approved the study and waived the need for informed consent from the patients and workers participating in the programme (201703095RINC).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.