Article Text

Abstract
Background Patients with nasogastric/nasoenteric tube (NGT/NET) are at increased risk of adverse outcomes due to errors occurring during oral medication preparation and administration.
Aim To implement a quality improvement programme to reduce the proportion of errors in oral medication preparation and administration through NGT/NET in adult patients.
Methods An observational study was carried out, comparing outcome measures before and after implementation of the integrated quality programme to improve oral medication preparation and administration through NGT/NET. A collaborative approach based on Plan-Do-Study-Act (PDSA) cycle was used and feedback was given during multidisciplinary meetings.
Interventions Good practice guidance for oral medication preparation and administration through NGT/NET was developed and implemented at the hospital sites; nurses were given formal training to use the good practice guidance; a printed list of oral medications that should never be crushed was provided to all members of the multidisciplinary team, and a printed table containing therapeutic alternatives for drugs that should never be crushed was provided to prescribers at the prescribing room.
Results Improvement was observed in the following measures: crushing enteric-coated tablets and mixing drugs during medication preparation (from 54.9% in phase I to 26.2% in phase II; p 0.0010) and triturating pharmaceutical form of modified action or dragee (from 32.8 in phase I to 19.7 in phase II; p 0.0010). Worsening was observed though in the following measures: crush compressed to a fine and homogeneous powder (from 7.4%% in phase I to 95% phase II; p 0.0010) and feeding tube obstruction (from 41.8% in phase I to 52.5% phase II; p 0.0950).
Conclusion Our results highlight how a collaborative quality improvement approach based on PDSA cycles can meet the challenge of reducing the proportion of errors in oral medication preparation and administration through NGT/NET in adult patients. Some changes may lead to unintended consequences though. Thus, continuous monitoring for these consequences will help caregivers to prevent poor patient outcomes.
- medication safety
- PDSA
- quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Medication administration through the oral route is a common practice in hospital settings and it is considered fast, safe and with low costs. Some patients are incapable of swallowing medications though. In these cases, nasogastric or nasoenteric tubes (NGT/NET) are valid alternatives.1 2
Not all pharmaceutical forms are safe for administration through an NGT/NET.3 Frequently, more than one oral medication is prescribed and scheduled for the same administration time, as well as modified-release drug forms are often prescribed for patients using an NGT/NET.4 5 Such actions bring potential risk to patients and contribute to patient safety incidents, including drug interactions, toxicity or tube obstruction.4 6
A research study conducted in three Brazilian hospitals verified that incidents with NGT/NET were related to incorrect oral medication preparation and administration techniques. From those incidents, tube obstruction was identified in 36.5% of all doses administered.7
Correct medication administration is a nurse responsibility and it represents an important target of quality and safety improvement interventions. Nurses need technical and scientific support to carry out safe and effective practices in the administration of pharmacotherapy via NGT/NET.8 9 This support may include multidisciplinary actions involving nurses, physicians, pharmacists and dieticians to ensure safe and effective nutritional therapy and pharmacotherapy in patients with these tubes.10 In this context, a quality programme aimed at preparing and administering oral medications through NGT/NET can result in improved quality of care and patient safety.11 12 Also, following the model for improvement, front-line practitioners and organisational leaders can quickly identify strategies that make a positive difference and result in a greater degree of success. By focusing on small tests to create and measure change, improvement is seen faster within an organisation, compared with the use of a typical research measurement, with minimal interruption in workflow.13
The quality improvement (QI) proposed by the Institute for Healthcare Improvement (IHI) was adopted in this study.5 14 This methodology is widely used in many countries, including the USA,15 the UK16 and Australia,17 but has not been explored in Brazilian research. It is a simple but powerful tool that accelerates the QI process. In addition to this process, three fundamental questions addressing aims, measures and changes are answered. These questions are intended to help practitioners identify their areas of concern.14 Furthermore, the Plan-Do-Study-Act (PDSA) cycle, also known as the Deming cycle, is used to test changes in the actual work environment and determine if the changes resulted in the intended improvement.5
The study objective was to implement a QI programme to reduce the proportion of errors in oral medication preparation and administration through NGT/NET in adult patients.
Methods
Study design
An observational study was carried out. We compared outcome measures before (phase I) and after (phase II) the implementation of the integrated QI programme, aiming to improve oral drug preparation and administration through NGT/NET in adult patients.
Setting
The study was conducted at Ribeirão Preto State Hospital, São Paulo, Brazil. This general medium teaching hospital has a 50-bed medical ward, 10 outpatient beds and 4 operating rooms. The medical ward was chosen because, at this site, adult patients receive care in various non-surgical, non-obstetric and non-gynaecological medical specialties.
Sample
The unit of analysis was defined in a previous research18 as oral medication preparation and administration through NGT/NET, measured by the proportion of wrong techniques in both processes. The sample consisted of 244 doses prepared and administered (122 doses before and 122 doses after the QI programme), which was a proportion associated with the research site.18 The sample size calculation was described elsewhere.19
Definitions
Wrong oral medication preparation was defined as a medicine that was incorrectly handled before administration through an NGT/NET. This included incorrect reconstitution (crushing enteric-coated medications); incorrect dilution (incorrect choice or volume of diluent); physicochemical incompatibility of medicines mixed in the same container and others.20
Wrong medication administration was defined as an inappropriate procedure or improper technique used in medication administration through an NGT/NET. This included mixing two or more drugs; improper flushing of the tube before, during and after each drug administration; mixing medications with feeding formulas; fail to test the correct placement of the NGT/NET before medication administration and others.20 21
An intervention was defined as a general notion or approach that is useful in developing specific ideas for changes that lead to improvement.22
Before the QI programme
From February 2014 to April 2015, we conducted a multicentre study to analyse nurse practices related to oral medication preparation and administration through NGT/NET. We ascertained the proportion of wrong medication preparation and administration techniques.18 At that time, we observed 374 doses of medications prepared and administered at three general medium teaching hospitals located in metropolitan areas (two hospitals in São Paulo state and one hospital in Minas Gerais State, Brazil). Wrong techniques were identified in both processes and the results were presented elsewhere.18
In all hospitals included in that study, nurses were not trained in drug administration through NGT/NET and formal training programmes did not exist for the handling of an NGT/NET. Nurses had little knowledge of controlled release and enteric coated dosage forms or of risks when mixing solid medications in the same crushing container during medication preparation. Furthermore, the hospital pharmacies were not systematically asked for advice concerning the preparation and administration of oral drugs to patients through feeding tubes.
Given the importance of pilot testing innovations before implementing them widely, the Ribeirão Preto State Hospital, São Paulo, Brazil, was selected as the implementation site for the QI programme. The choice was due to the existing partnership between the members of the research team and the Risk Management Commission, and the interest of hospital managers in the research project. Thus, preintervention data (phase I) included the observation of 122 doses of oral medications administered to 16 adult patients with an NGT/NET.
After baseline assessment, further PDSA cycles gathered feedback and assessed the impact of QI interventions.23
Improvement strategy
The step-by-step approach based on the model for improvement was put in practice as recommended by IHI24:
To analyse nurse practices related to medication preparation and administration through NGT/NET, ascertaining the rates of wrong medication preparation and administration, data collected from February 2014 to May 2014 at Ribeirão Preto State Hospital were used (phase I—baseline measurement). The following results were obtained:
Medication preparation
No hand washing before medication preparation (40.8%).
Crushing enteric-coated tablets (5.6%).
Mixing drugs during medication preparation (43.5%).
Liquid medications with a high osmolality incorrectly dilute or not dilute (9.6%).
Prepared medication not labelled (60.4%).
Medication administration
No hand washing before medication administration (48.1%).
Testing feeding tube placement before medication administration, not done (67.6%).
Flushing of the tube before medication administration, not done (62.5%).
Administering medications together (65.6%).
Flushing of the tube between medications, not done (86.5%).
Administering medication that adsorbs or interacts with enteral nutrition, without observing the minimum recommended interval between ingestion (30.5%).
All QI methods rely on measurements. Thus, data were collected through direct observation of oral medication preparation and administration through NGT/NET. The observer recorded exactly what the nurses did with the medication and witnessed the medication’s administration to the patient. Data recorded included related procedures, such as giving medications with food.
During the processes of preparing and administering medications, nurses were observed by the principal investigator, who received a day of training with a total workload of 4 hours. For this purpose, the research team developed a data collection tool. The tool was then submitted to a panel of experts for face and content validity, followed by three consecutive testing days.18
Observations took place on different days of the week (including weekends and holidays) and at different times of the day and night. Nurses were observed for a maximum number of four times to include as many different nurses as possible.25
The observer was present during a preset series of shifts, to represent the variation of working hours in nursing practice. When a potentially harmful error was identified (dose omission), the observer did not only register the error but also intervened by talking to the nurse about the case. Prescriptions were also analysed to identify the presence of enteric-coated tablets prescribed to be administered through an NGT/NET.
We identified the use of wrong techniques in both processes (medication preparation and administration). According to Langley et al,26 before implementing a QI project, it is necessary to work with the people involved in the process, because of the importance of all team members recognising that problems exist and that they need to be addressed. With this goal in mind, the results were presented to a multidisciplinary team that included nurses, physicians, pharmacists, hospital dietician, service managers and an administrative assistant.
An improvement team was formed to implement the planned changes, using low-cost QI interventions. The project team consisted of a nurse manager, a (head) nurse of the infection control committee, a pharmacist end a hospital dietician. The members of the QI project signed a verbal contract to improve the techniques nurses use during oral medication preparation and administration through NGT/NET.
The following objectives were agreed on: (1) to reduce the proportion of wrong techniques in oral medication preparation by 80% in a period of 3 months and (2) to reduce the proportion of wrong techniques in oral medication administration through NGT/NET by 80% in a period of 3 months.
We should make sure that all measures have been maintained over time. Therefore, Langley colleagues26 recommend a list of up to six manageable measures. Thus, the measures selected for this study were:
Medication preparation measures
Hand washing before medication preparation.
Crush compressed to a fine and homogeneous powder.
Crushing enteric-coated tablets and mixing drugs during medication preparation.
Triturated pharmaceutical form of modified action or dragee.
Medication administration measures
Flushing of the tube before medication administration.
Flushing of the tube between medications.
Flushing of the tube after medications.
Feeding tube obstruction.
Three PDSA cycles (Phase II) were needed to achieve our objectives; from April to November 2015, two consecutive cycles were performed. From June to July 2017, the third cycle was held and a total of 122 doses were observed, administered to 16 patients as shown in figure 1. Data from 2015 to 2017 are still applicable in 2019 because the changes remained in place over time, as observed in processes monitoring during 2018 and 2019.

Quality improvement program phase II diagram. Cycles 1 and 2: two consecutive cycles were performed. The first served to elaborate the good practice guide for the preparation and administration of oral medication via NGT/ NET. The second was to offer training to the nursing staff. Cycle 3: the goal was to evaluate drug preparation and administration via NGT/ NET and compare the data with the baseline result. NGT/NET, nasogastric/nasoenteric tube; PDSA, Plan-Do-Study-Act.
Cycle 1 (from April to August 2015)
Good practice guidance for oral medication preparation and administration through NGT/NET was tested. This guidance was developed by the project researchers based on an integrative literature review and the entire process was published elsewhere.27 The guidance was presented to the improvement programme team. Four meetings were held from April 2015 to August 2015 to adapt the medication guide according to the hospital. The meetings were held at the study hospital site so that the researchers could assist the team in action planning, and they had a maximum duration of 60 min each.
The good practice guidance was made available in hospital computers and a hard copy was made available to the hospital pharmacy and nursing stations. Members of the QI team exchanged experiences and knowledge to solve the task. The QI team decided that the next cycle would be to train the hospital nursing staff about the changes made. The following changes were tested: to provide a printed list of oral medications that should never be crushed to all members of the multidisciplinary team and to provide to prescribers a printed table at the prescribing room containing therapeutic alternatives for drugs that should never be crushed.
Cycle 2 (November 2015)
Formal theoretical and practical training sessions were provided by the principal investigator for nurses to use the good practice guidance. Also, a video was developed by the research team to enhance oral medication preparation and administration through NGT/NET and it was used during training sessions. Nine training sessions were conducted in 2 days and each session lasted 60 min each. Eighty-one per cent of nurses were trained; the remaining 20% were vacationers or absenteeism professionals. Nurses’ knowledge was assessed before and after the training sessions through multiple-choice questions.
The improvement team gradually implemented the changes over 2 months (after a 7-month baseline period). We anticipated that empowering nurses would be more effective than providing education alone. Thus, a short version of the good practice guidance was made available at the nursing station and a table containing therapeutic alternatives for oral medications that should never be crushed was available for physicians and nurses.
Cycle 3 (from June to July 2017)
We compared the proportion of wrong techniques the nurses used during oral medication preparation and administration through NGT/NET, before and after the interventions. The same researcher observed the nurses, using the same data collection tool that was used during phase I. The researchers decided to present the results of every cycle during an improvement team meeting with the main stakeholders to gather feedback and decide on the actions to be taken.
Data analysis
Data were entered in EpiData V.3.1 and were subsequently transferred to R software. Data analysis was performed using a weekly statistical process control chart to monitor the process and identify problems if observed. Common variation cause follows a normal distribution and it means that the process is stable, within the limit of control. Special variation cause occurs by errors that must be eliminated. The limits are out of control by changing the SD and average values.25
The Pearson χ2 test or Fisher’s exact test were used to analyse the following variables: hand washing before medication preparation; crush compressed to a fine and homogeneous powder; crushing enteric-coated tablets and mixing drugs during medication preparation; triturated pharmaceutical form of modified action or dragee; flushing of the tube before medication administration; flushing of the tube between medications; flushing of the tube after medications and; feeding tube obstruction. All analyses were carried out with a significance level of 5% (α=0.05).
Ethics
Nurses and patients were informed of the project and asked to voluntarily sign the consent form before enrolment in the study. They were informed of possible risks which were: nurses were intercepted by the observer if a wrong technique occurred during medication preparation and/or administration and the fact that the observer’s intervention could be vexing. The situation was treated respectfully though and nurses were asked to review their conduct. Lack of patient privacy during medication administration may have occurred. Also, participants were informed that the results will be used for possible publications. We guaranteed their confidentiality and anonymity.
Results
Our primary outcomes were the improvement in the proportion of oral medications correctly prepared and administered after the QI programme.
During the implementation of the process changes, 81% of the nurses were formally trained regarding the use of the best practice for oral medication preparation and administration through NGT/NET.
There was an increase in the proportion of hand washing before medication preparation (from 22.1% in phase I to 54.1% in phase II; p 0.0010). Improvement was also identified in the following measures ‘crushing enteric-coated tablets and mixing drugs during medication preparation’ (from 54.9% in phase I to 26.2% in phase II; p 0.0010) and ‘triturated pharmaceutical form of modified action or dragee’ (from 32.8 in phase I to 19.7 in phase II; p 0.0010). The following measures also improved: ‘flushing of the tube before medications administration’ (from 13.1% in phase I to 29.5% in phase II; p 0.0020), ‘flushing of the tube between medications’ (from 8.2% in phase I to 66.3% in phase II) and ‘flushing of the tube after medications’ (from 86.8% in phase I to 92.6% phase II; p 0.1340) (table 1).
Techniques used by nurses during oral medication preparation and administration through NGT/NET
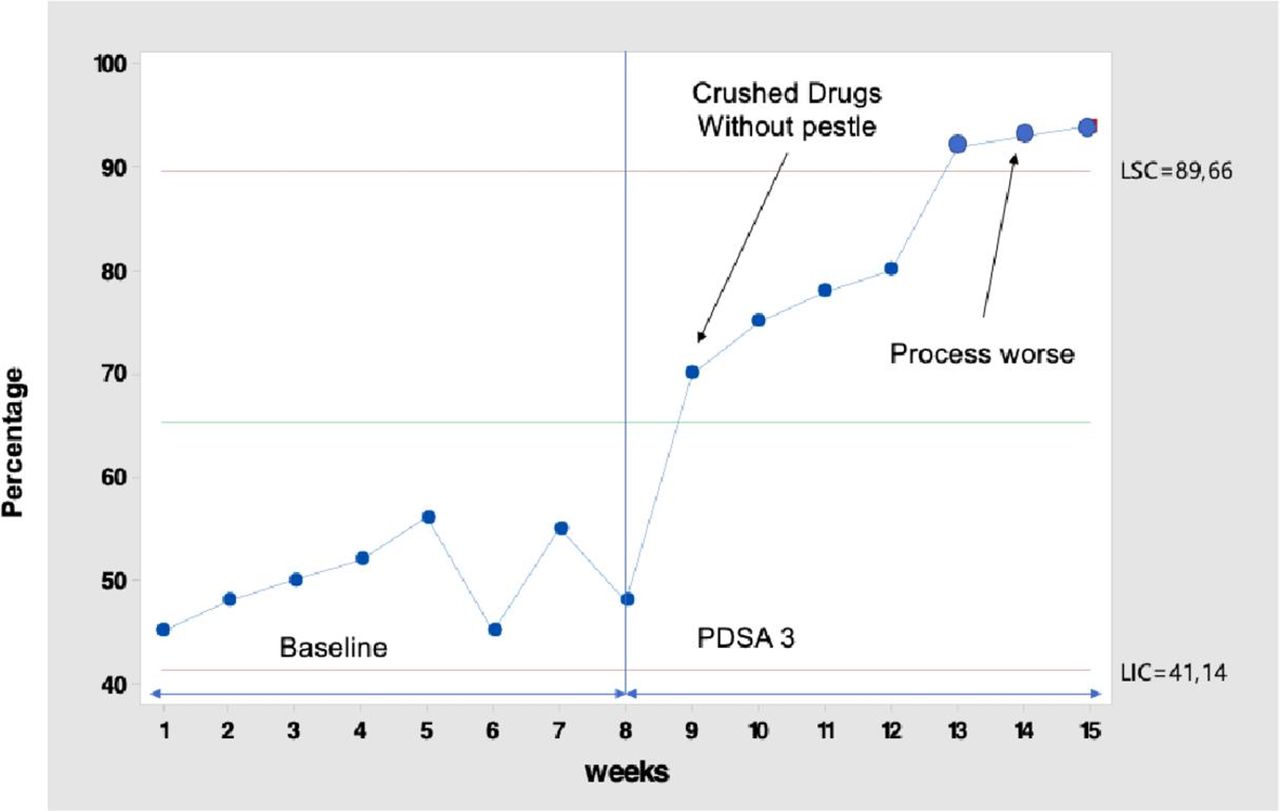
Worsening in the following measures were also observed: ‘crush compressed to a fine and homogeneous powder’ (from 7.4%% in phase I to 95% phase II; p 0.0010) and ‘feeding tube obstruction’ (from 41.8% in phase I to 52.5% phase II; p 0.0950) (table 1). During the observations, however, we identified that in the hospital there was no mortar with a pestle to crush the solid forms (figure 2).

{kind=link}
{kind=link}
Weekly statistical process control chart showing the percentage of crush compressed to a fine and homogeneous powder. Control chart showing the percentage of crush compressed to a fine and homogeneous powder. Administered to 16 patients reporting continuous observation and follow-up periods. Hospital elected to the improvement programme made changes to improve oral medication preparation and administration techniques via NGT/ NET. PDSA 3: We found that in the hospital there was no pestle mortar to crush the solid forms, it is clear that the process worsened. NGT/NET, nasogastric/nasoenteric tube; PDSA, Plan-Do-Study-Act.
It could be observed that oral medications were not crushed with the aid of a mortar and pestle, as such devices were not available on the hospital throughout the data collection period. Oral medications were, therefore, triturated in the most varied ways: crushed on their very own packages, employing the help of scissors or a syrup bottle; reconstituted in plastic disposable cups; among others.
In November and December 2017, the QI project team met at the hospital with the researchers. The results were presented and the need for a new change was discussed. The team decided to purchase a porcelain mortar with a pestle to reduce errors in oral medication preparation through NGT/NET.
Discussions
By implementing a QI programme to reduce errors in oral medication preparation and administration through NGT/NET in adult patients, the following measure improved: ‘triturated pharmaceutical form of modified action or dragee’. It is known that modified action pills cannot be crushed, as this will diminish their action.28 29 Another important variable that may affect pharmacological actions on organisms is the way the healthcare professional prepares and administers medications through NGT/NET. It was observed that solid forms of modified action pharmaceuticals forms were crushed and that high osmolarity medications were diluted incorrectly and this error may result in adverse reactions such as vomiting and diarrhoea.30 31
Additionally, we verified that, when there was more than one oral medication prescribed and scheduled for the same administration time, nursing teams crushed them together to enable the administration through an NGT/NET. In another study performed in a Brazilian hospital, 39.2% of oral medications were crushed simultaneously and administered with the aid of NGT/NET.19 Preparing and administering more than one drug simultaneously may cause physicochemical interactions capable of making drug therapy unfeasible, eventually causing complications for patients, such as possible adverse reactions: diarrhoea, nausea and tube obstruction.8 32
Another error observed in this study was the fact that nursing teams did not wash the tubes before medication administration, between medications and after the procedures are completed. In an investigation conducted in an intensive care unit of a private Brazilian hospital, 80% of nursing technicians and 100% of all nurses affirmed that tube obstruction was related to errors in oral medication preparation and administration.33 These errors result in unnecessary increases in expenses and costs to healthcare systems.34 In a study, researchers compared costs related to errors occurred during oral medication preparation and administration in three Dutch hospitals. After QI interventions, savings reached US$342 million each year.35 QI programmes in health-related processes are indicated for upgrading such systems and reducing unnecessary costs.
This study implemented a good practice guidance to support nurses during oral medication preparation and administration through NGT/NET. As a result, some measures improved, such as: ‘flushing of the tube before medication administration’, ‘flushing of the tube between medications’, ‘flushing of the tube after medications’. These actions have the potential to prevent potential adverse reactions and tube obstructions. A previous study conducted in a Brazilian hospital reports the significance of care protocols always being available for nursing teams, as these guarantee the effectiveness and standardisation of care techniques in nursing.36 37
Another problem identified during oral medication preparation was not ‘crushing and compressing to fine and homogeneous powder’, due to a lack of equipment. This error on the technique may result in tube obstruction because the granules may adhere to the tube’s lumen.38 39 It is essential to train nurses and provide adequate quality equipment, for the technique to be executed correctly, therefore, ensuring the patient’s safety while using tubes for gavage.
Interventions on QI demand dedication and time to make the processes safe and efficient. Small PDSA cycles are recommended for testing interventions and, starting on the learning process (PDSA cycle), implementing and spreading changes in health environments. These must start at a local level, then regional, then national, to achieve our social compromise of providing safe and efficient care.40 41 An interactive learning cycle is established, for comparisons of collected data and building a knowledge which will serve as an entry point for the next cycles.42
Lessons learnt
The good practice guidance for oral medication preparation and administration through NGT/NET and a printed table containing therapeutic alternatives for drugs that should never be crushed provided to prescribers at the prescribing room was pointed by the QI team as an important barrier for safe medication through NGT/NET. Before preparing and administering medications via NGT / NET, the nursing staff consults the chart to identify whether or not prescribed medications can be administered via NGT/NET. The lack of adequate equipment to crush the tablets to fine, homogeneous powder made the process worse, but the team itself recognised the need for the equipment and will be provided by the institution. Future PDSA cycles will be required to implement and test this change.
Limitations
The observation method for studying medication preparation and administration errors can influence the results because the presence of an observer may affect the nurse’s behaviour at the beginning of the observations. The long-term approach helped to overcome the Hawthorne effect though, because nurses got used to being observed.
The results may not be generalisable to other departments or other hospitals because the study involved the medical ward of a general medium-sized hospital, thus the incidence of oral medication preparation and administration may be lower when compared with an intensive care unit or the medical ward of a large university hospital. Another aspect to be considered was the non-inclusion of patients and caregivers in the meetings, as they could have contributed to their perceptions about the process of drug administration by NGT/NET. Their concerns were addressed during the study period and they received information about safe medication administration.
Conclusions
Our results highlight how a collaborative quality improvement approach based on PDSA cycles can meet the challenge of reducing the proportion of errors in oral medication preparation and administration through NGT/NET in adult patients. However, some changes may lead to unintended consequences, thus, continuous monitoring for these consequences will help caregivers to prevent poor patient outcomes.
Acknowledgments
We thank the nursing staff and pharmacists at the study hospital.
References
Footnotes
Contributors RAP contributed to the study concept and design, acquisition of data, analysis of data, drafting of the manuscript. FBdS contributed to drafting of the manuscript and critical revision of the manuscript. MCGR contributed to drafting of the manuscript and critical revision of the manuscript. JRP contributed to drafting of the manuscript and critical revision of the manuscript. LRMdC contributed to drafting of the manuscript and critical revision of the manuscript. FREG contributed to the study concept and design, drafting of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.