Article Text

Abstract
Patients admitted to the hospital and requiring a subsequent transfer to a higher level of care have increased morbidity, mortality and length of stay compared with patients who do not require a transfer during their hospital stay. We identified that a high number of patients admitted to our intermediate care (IMC) unit required a rapid response team (RRT) call and an early (<24 hours) transfer to the intensive care unit (ICU). A quality improvement project was initiated with the goal to reduce subsequent early transfers to the ICU and RRT calls. We started by focusing on IMC patients, implementing acuity-based nursing assignments and standardised daily nursing rounds in the IMC aiming to reduce early patient transfers to the ICU. Then, we expanded to all patients admitted to a hospital medical unit from the emergency department (ED), targeting patients with gastrointestinal (GI) bleed and sepsis who were at a higher risk for early transfer to the ICU. We then created an ED intake huddle process that over time was refined to target patients with SIRS criteria with an elevated serum lactic acid level greater than 2.0 mmol/L or a GI bleed with a haematocrit value less than 24%. These interventions resulted in an 10.8 percentage points (31.7% (225/710) to 20.9% (369/1764)) decrease in the early transfers to the ICU for all hospital medicine patients admitted to the hospital from the ED. Mean RRT calls/day decreased by 17%, from 3.0 mean calls/day preintervention to 2.5 mean calls/day postintervention. These quality improvement initiatives have sustained successful outcomes for over 6 years due to integrating enhanced team communication as organisational cultural norm that has become the standard.
- healthcare quality improvement
- emergency department
- critical care
- continuous quality improvement
- quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- healthcare quality improvement
- emergency department
- critical care
- continuous quality improvement
- quality improvement
Problem
In 2011, we identified that an unusually high rate of patients admitted from the emergency department (ED) to the intermediate care unit (IMC) required subsequent early transfer (within 24 hours of admission) to a higher level of care in the intensive care unit (ICU). Essentially, sick patients were going to a floor that was unable to care for them, leading to a stressful rapid response team (RRT) call and a quick transfer of an unstable patient to the ICU. In addition to the patient risks, we identified this inappropriate placement of patients as contributing to burnout and turnover among staff nurses. Accordingly, we undertook a quality improvement intervention directed at placement of patients to units most appropriate for their care needs. During this quality improvement initiative, we identified additional problems along the way. First, early transfers were a bigger issue that occurred throughout the hospital, not just in the IMC; second, patients with a sepsis or gastrointestinal (GI) bleed diagnosis where most at risk for early transfers.
The aim of this project is to reduce early transfers and RRT calls by ensuring patients are admitted to the most appropriate unit from the start. We hypothesised that an intake huddle between the treating ED team and the receiving admitting team would address these goals.
This quality improvement project was conducted at Virginia Mason Medical Center (VMMC), a multidisciplinary healthcare institution in the Pacific Northwest that includes a central urban campus with a 336-bed hospital and a network of suburban regional outpatient medical centres. This investigation was performed as part of a quality improvement project and therefore was determined by the International Review Board to be exempt from formal oversight.
Background
ED clinicians are often tasked the challenge of triaging the ‘borderline’ patients, whose needs are higher than a general floor but do not clearly need ICU care.1 The process of identifying patients at risk for deterioration can be difficult and determining where to admit a patient from the ED can be complex and multifactorial. Different clinical scores have been developed to prevent delays in treatment or transfers of critically ill patients, and can help clinicians better triage patients, such as the Modified Early Warning Score (MEWS) for surgical patients and the quickSOFA for sepsis.2 3 However, the clinician’s decision to admit to the ICU is largely dependent on the clinician’s individual preference, judgement and experience.4 Transfers to the ICU after hospital admission are associated with higher mortality and length of stay (LOS).5–9 At our institution, the IMC provides a middle ground between the ICU and general floor; however, some patients decline clinically and subsequently require transfer to the ICU. Appropriate placement of low-risk patients in IMCs has shown to reduce mortality by providing greater access to the ICU for critically ill patients.10
Poor communication during the transition from ED to inpatient care has been identified as a key source of error in diagnosis, treatment and disposition.11 12 A standard process for a conversation between the ED and admitting team when admitting a patient to have consensus on the plan of care has previously been shown to reduce improper assignments that result in early transfer to a different floor and LOS.13
Measurement
To identify inappropriate placement of patients, we measured the number of both early transfers to the ICU and RRT calls. These metrics were chosen because they indicate there is mismatch between a patients’ need and nursing staff resources; ultimately, indicating that the patient is in the wrong place.
We initially measured early transfers by monitoring the number of patients admitted from the ED to the IMC, and then transferred to the ICU in less than 24 hours, during the first quality improvement event from December 2011 to March 2012. During this event, we did quick Plan-Do-Study-Act (PDSA) cycles measuring outcomes at the 30-day, 60-day, 90-day intervals.14 We used the lessons learnt from this first quality improvement event to scale up our efforts to reduce even more early transfers to the ICU with a second quality improvement event. For the second quality improvement event, we redefined and measured the early transfer population as any hospital medicine patient admitted from the ED, who subsequently transferred to the ICU in less than 24 hours. The second event took place from July 2012 to October 2012. During the second quality improvement event, we also included quick PDSA cycles at 30, 60 and 90 days that measured LOS (days) for VM hospitalist medicine patients; time (in full-time employment (FTE)) hospitalist spent transferring patients to the ICU; and set-up reduction: time spent determining the level of care for an admission during initial hand-off conference call. The number of huddles was also recorded in a huddle log from August 2010 to September 2014.
Study methods and outcome
To assess the sustainability of these quality improvement efforts over time, we conducted a retrospective, observational study evaluating the preintervention (January 2009–November 2011), during intervention (December 2011–October 2012), and postintervention (November 2012–December 2018) periods. Primary outcomes included the number of ED patients admitted to a hospital medicine floor and then required an early transfer to the ICU, the number of RRT calls and the mean number of RRT calls/day from March 2011 to December 2018. Preintervention, during intervention and postintervention patient demographics and outcomes were summarised. Analysis of patient demographics and early transfers does not include data from the year 2016, since an inpatient hospital unit changed names and we were unable to correctly track patient placement. Patients or the public were not involved in the design, or conduct, or reporting or dissemination plans of our project.
Statistics
Preintervention and postintervention measures were compared using Student’s t-test for continuous variables, except for median LOS which is Wilcoxon rank-sum test. χ2 tests were used for dichotomous variables. Data were also explored graphically using run charts. We used Stata MP V.15 for all analysis (StataCorp, College Station, Texas, USA). The most frequent primary discharge diagnose was also described determined by International Classification of Diseases (ICD)9 and ICD10 codes: Sepsis 038, A40, A41; Stroke 431, 434, I61, I63; Respiratory failure 518.8, J96.
Design
Our institution’s cultural foundation is strongly rooted in the Virginia Mason Production System (VMPS) that uses Lean management and continuous quality improvement methodologies. This quality improvement initiative used on the VMPS model which functions by empowering front-line workers to impact change through multidisciplinary quality improvement events lasting 2–5 days. These events are highly organised and involve a diverse team with clear roles and responsibilities, collection of baseline data to ensure informed and objective understanding of the problem, developing innovative improvement interventions and trial of the interventions through PDSA cycles.15
This collaborative project between the ED and hospital medicine teams extended from November 2011 to October 2012 through two quality improvement events and a series of PDSAs. Based on our data and prior research that identified the ED as an intervention point, we sought to optimise triage and placement of patients with the goal that patients receive the right care at the right time, without waits or delays.
Strategy
Our improvement process was iterative; the intervention phase included a series of two quality improvement events that involved multiple PDSA cycles.
Quality improvement event 1 (December 2011–March 2012): mistake proofing IMC flow
We held a 2-day quality improvement event to address which patients are admitted to the IMC and whether the appropriate nursing resources and coordination were available. Prior to this event, there was no standard process for anticipating nursing needs based on patients’ clinical condition. Problems stemming from this lack of standard process included: (1) patients can decompensate quickly and need to transfer to the ICU within a short time of arriving to the IMC; (2) nursing ratios, staffing and assignment making was challenging; (3) great difference in the acuity of the IMC patients could exist.
This event sought to create a process to ensure the IMC was prepared to meet patient needs by developing a safe assignment acuity tool (table 1) to help make nursing assignments and standardised daily nursing rounds. This process involved the charge nurse rounding with each IMC nurse on their patients at the start of each shift. During these rounds, they used the acuity tool to assign a color-coded status to each patient using red, yellow or green stickers on piece of paper that hung visibly at the nursing station to make visual the acuity status. Acuity status was determined by multiple variables, such as frequency of medication and assessments, blood transfusion need and if the patient was improving or declining. At the start of each shift, the charge nurses from the IMC, ED and ICU met to review each units’ census, patients’ acuity statuses and nursing needs. This meeting helped these three units that patients commonly transferred between develop a shared understanding, so the units were less isolated and could be better prepared to match nurse staffing to meet patients’ needs.
Safe assignment acuity tool
Quick PDSA cycles of this process showed a 49% (35–18 patients) decrease in the number of total transfers from the IMC to the ICU; however, the proportion of early transfers from the IMC to the ICU increased from 54% (9/35) at baseline and 77% (14/18) at 60 days, despite three revisions of the acuity assignment tool.
We learnt there was work to be done on reducing early transfers before patient arrive to the IMC, which meant looking at patients in the ED. We also identified that transfers to the ICU was a complex issue throughout the hospital and not a unique to the IMC. Accordingly, this led us to look at all patients being admitted from the ED, not only just those going to the IMC.
Quality improvement event 2: (July 2012–October 2012): intake huddle
A 5-day quality improvement event was the organisation’s second event focused on reducing early transfers in the hospital. The scope of this project was larger and included all hospital medicine admissions. The goal of this event was to further reduce the waste associated with early transfers and assign the patient to the correct level of care on arrival.
A root cause analysis with a convenience sample of 24 patient who had early transfers showed that 36% of these patients were admitted from the ED. The greatest reason for early transfer to the ICU was haemodynamic instability with 47% of patients meeting criteria for systemic immune response syndrome (SIRS), a non-specific set of clinical criteria typically used in defining sepsis (SIRS+infection). We envisioned employing SIRS to screen for patients at high risk of requiring an early unit transfer to a higher level of care.
With this information, an intake huddle process was formed, bringing a face-to-face meeting between the ED and admitting teams at the time of admission to the hospital with the goal of determining appropriate placement of patients. We created the ‘Intake Huddle Criteria’ (box 1) used by the Hospital Admission Centre (HAC) nurse to identify which patients needed an intake huddle prior to admission. If the intake huddle criteria were met, the HAC nurse coordinated an intake huddle between the flow supervisor, accepting inpatient provider, hospital unit charge nurse and primary ED nurse to determine next steps for patient care as well as unit placement in the hospital. The intake huddle criteria is not a validated tool perfect at estimating need for ICU admission, but rather a simple method that we devised to guide determination of unit placement. This tool was developed ad hoc during our quality improvement event with input from our physician and nurses.
Intake huddle criteria
Always admit to ICU if possible sepsis and lactate is greater than or equal to 4
Possible sepsis with current heart rate greater than 100, systolic blood pressure less than 100 or lactate greater than or equal to 2.5
Gastrointestinal bleed with heart rate greater then 100, systolic blood pressure less than 100 or haematocrit value less than or equal to 24%.
ICU, intensive care unit.
After implementation, we recognised that the intake huddle process was being used too frequently to be sustainable, with up to 60 huddles in 1 week. We went back to the data and realised that of the patients with SIRS, the patients at high risk for requiring ICU care also met clinical criteria for sepsis with an elevated serum lactic acid level (greater than 2.0 mmol/L). We modified the intake huddle criteria to include a lactic acid threshold and had a prompt, significant reduction in the number of weekly intake huddles, now restricted to a population largely with sepsis as the primary diagnosis.
The data also identified a second population of patients with a high risk of early transfer to the ICU: patients with GI bleeding and a low haematocrit. These patients had a complaint of GI bleeding and a haematocrit value less than 24%, indicating anaemia without the SIRS seen in the septic patient population. Rather than using the huddle process for this population, we created messaging to the ED and hospitalist teams that these patients were high risk for requiring ICU care and to consider that in admitting placement.
We measured convenience samples in the context of quick PDSA cycles of the intake huddle process and identified a 17% (92/743 at baseline, 15/152 at 90 days) decrease in the proportion of early transfers to the ICU for all hospital medicine patients admitted from the ED; a 2% (4.37 days at baseline, 4.46 days at 90 days) increase in the average LOS (in days) for a VM hospitalist medicine patient; 41% (0.081 FTE at baseline, 0.047 FTE at 90 days) decrease in the time (in FTE) hospitalists spent on early transfer to the ICU; and a 41% (8 min and 33 s at baseline, 5 min at 90 days) reduction in the time spent determining the level of care for an admission during the initial hand-off conference call. The number of ED huddles was also logged from August 2012 to September 2014; this showed the average number of huddles a month to be: 39 (195/5) from August to December 2012; 49 (586/12) from January to December of 2013; 44 (396/9) from January to September 2014.
Results
Over the course of the 10-year evaluation period, there were a total of 2765 hospital medicine patients admitted from the ED to a hospital floor that required early transfer to the ICU or were directly admitted to the ICU from the ED. The mean patient age decreased from 65 to 64 years (p=0.04). There was an increased proportion of patients with sepsis in the ICU postintervention. Mean LOS and discharge status were unchanged when comparing preintervention and postintervention time periods. Patients who had an expired discharge status was statistically unchanged from 11% (76/710) preintervention to 13% (369/1764, p=0.19) postintervention (table 2).
Demographics and outcomes of hospital medicine patients admitted from the ED to a hospital floor that required early transfer to ICU, 2009–2018 (analysis does not include patients in year 2016 unless indicated otherwise)
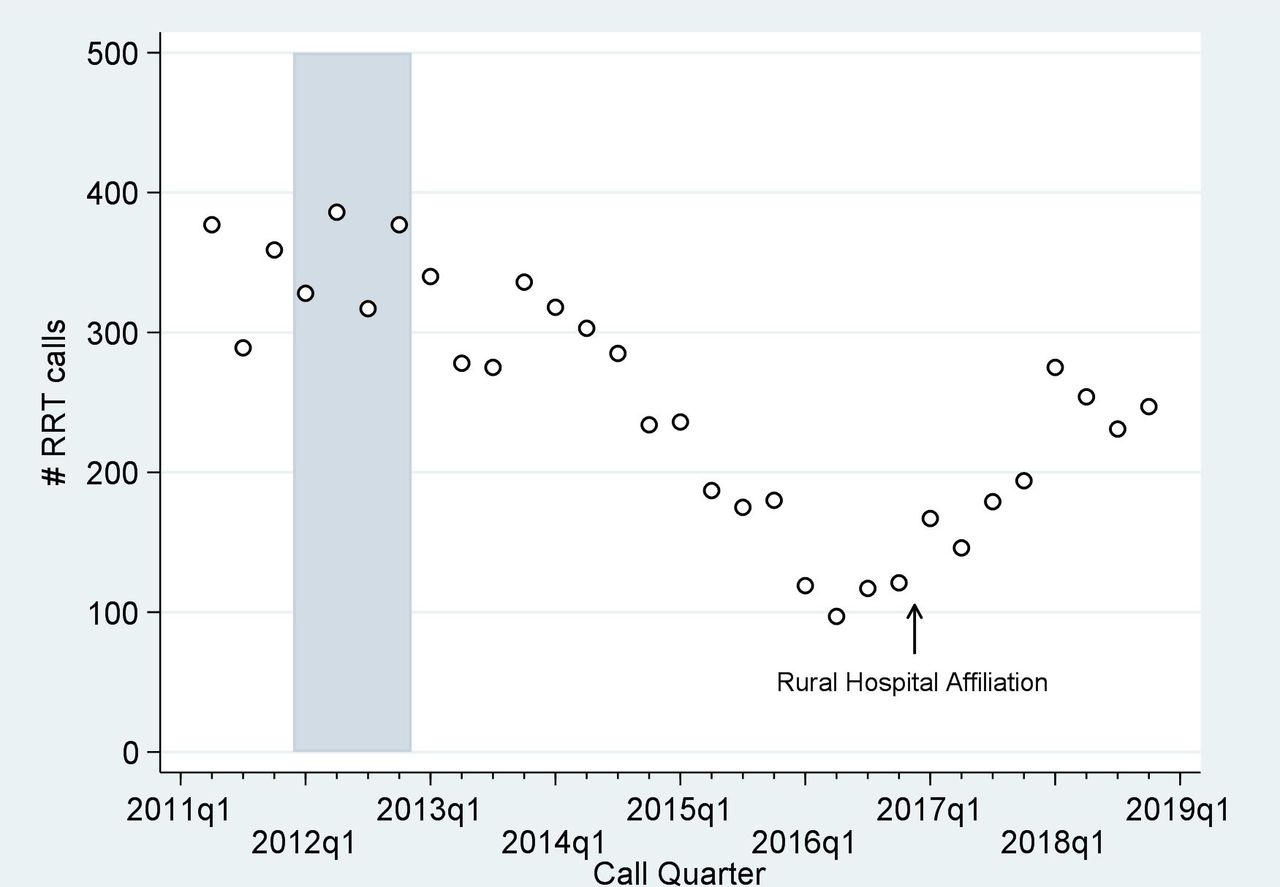
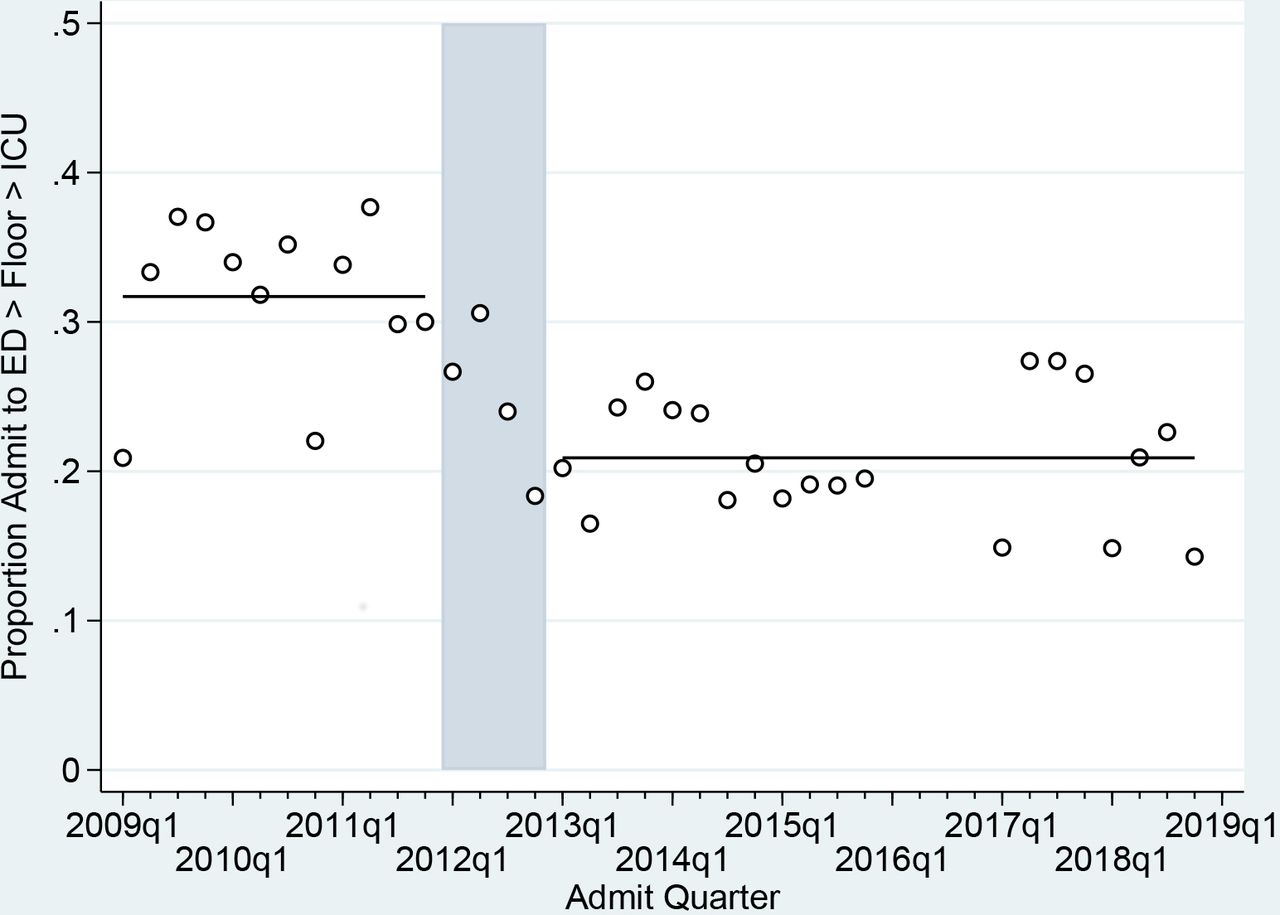
Following these two quality improvement events, there was improvement in both early transfers and number of RRTs sustained over 6 years postintervention. Early transfers to the ICU decreased by 10.8 percentage points (31% (225/710) to 20.9% (369/1764), relative reduction 34% (p<0.001)) (figure 1). The number of RRT calls/day decreased from 3.0 preintervention to 2.5 postintervention (p<0.001) (table 2). Figure 2 shows that the absolute number of RRT calls per quarter also decreased through 2017. This decrease corresponded temporally with the intervention in 2012.

Time series showing the proportion of patients admitted to the floor from the emergency department (ED) who are transferred early to the intensive care unit (ICU), before, during and after the intervention. The shaded grey area indicates the intervention time.
{kind=link}
{kind=link}
Time series showing the number of rapid response team (RRT) calls across all hospital medicine patients, before, during and after the intervention. The shaded grey area indicates the intervention time.
Lessons and limitations
Through these quality improvement initiatives, we demonstrated that using the ED as an intervention point to facilitate communication for hospital admissions can successfully reduce early transfers to the ICU and the number of RRT calls. In the first quality improvement event, the IMC attributed their success to the acuity-based assignment algorithm tool that gave nurses clinical parameters and empowered them to say ‘no’ to inappropriate transfers. This work catalysed a larger organisation effort to address early transfers for all hospital medicine patients. With our second quality improvement event, PDSA cycles showed that the implementation of the intake huddle effectively reduced early transfers of patients to the ICU and the number of RRT calls. This work helped break down the medical specialty silos between the ED and inpatient teams to enhance communication and shared knowledge that contributed to placement of patients on units appropriate for their needs. Previous studies have also shown the ED as a successful intervention point, where improved communication during patient admission can reduce inappropriate patient assignments and early transfers.13 16
Over time we demonstrated sustained success of our outcome measures even though the number of intake huddles declined. We believe this decline occurred because our efforts to ensure patients receive appropriate care and enhanced team communication became so engrained into our organisation culture that despite the number of intake huddles declining, the work became our standard way of doing things.
To achieve this success and sustain it, required different types of changes from our teams that can be broken down into technical versus adaptive type change. First, technical changes represent changes that occur when there are clearly defined problems and known solutions that are delegated. For example, a technical change in this project was introducing the use of the intake huddle criteria. This tool sought to provide the nurses who used it with clear answers with how to navigate the defined challenge of if an intake huddle was needed or not. Second, there is adaptive change, this type of change occurs when there are poorly defined problems and solutions. Adaptive change requires learning and empowers front-line workers to reach solutions. An example of adaptive change in this project is when we sustained reduced early transfers and RRT calls despite doing fewer actual intake huddles. This demonstrates how the technical change of the intake huddle became less necessary over time as our culture integrated this work so deeply that it simply became a customary way of doing things.17
There are a number of limitations to this study. First, in terms of data limitations, this is a retrospective, observational study, without a control group. We are unable to exclude confounding variables due to other ED and unit changes that may have also occurred around the time of these interventions. Furthermore, we did not assess how these interventions may have affected higher level systems. For instance, we do not know if there was less ICU availability due to instituting a lower threshold for ICU admissions, or if the interventions caused the ICU to be less able to receive transfers from other hospitals that could have delayed or limited access to necessary care. Examining the factors that impact accepting ICU transfers would be valuable information added and a consideration for future work on this topic.
The temporal aspect in retrospective studies can make assessments difficult. For example, the acquisition of a rural hospital during our postintervention period changes our patient population and may have influenced the reported sustainability of RRT calls. Additionally, we were not able to locate some implementation metric data (ie, the number of intake huddles logged after 2014) that were reportedly kept. Some implementation metrics were never collected (ie, rate of huddle effectiveness, meaning the number of times bed assignment changed based on the huddle). If we were to undertake this project again, we would keep a better record of the timeline and include more implementation metrics. Another limitation, given that many of our outcome measures were collected during the PSDA cycles, is that team members could have altered their behaviour, consciously or subconsciously, knowing they were in a time observation. This is a known observer effect and can impact the integrity of results. There is the question of generalisability of these data given this was a single-centre study, deeply committed to quality improvement at the core of its culture. Lastly, there was no analysis on nursing turnover or morale which would be added valuable information and an area worth further investigating in the future.
Conclusion
A quality improvement framework was used to address the challenges of early transfers to the ICU and number of RRT calls through a series of quality improvement events and PDSA cycles. During this process, we analysed the cause of early transfers and identified patients with SIRS criteria with a positive lactate and patients with GI bleeds and a low haematocrit were responsible for a large portion of these cases. We created an inpatient huddle process to flag high-risk patients and bring together the ED and inpatient treatment teams to determine the most appropriate unit for admission. This effectively reduced the number of early and the number of RRT calls. These results have been sustained for years as these changes in communication have been incorporated into hospital culture.
Acknowledgments
The front-line staff, including patient care technicians, nurses and clinicians, who are passionately committed to providing the highest quality of care to our patients and willing to make changes to improve patient care. The Center for Health Care Improvement Science for their expert guidance and support in quality improvement methodology.
Footnotes
Contributors SH: planned and conducted the study, data analysis, manuscript author. SO: planned and conducted the study, authorship of manuscript. CG: planned and conducted the study, contributed to intellectual content of the manuscript. EC: planned and conducted the study, contributed to intellectual content of the manuscript. BW: planned and conducted the study, statistical analysis and interpretation of the data, revised the manuscript for quality improvement methodology. CB: planned and conducted the study, revised the manuscript for quality improvement methodology.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.