Article Text

Abstract
Introduction A toxic organisational culture (OC) is a major contributing factor to serious failings in healthcare delivery. Poor OC with its consequences of unprofessional behaviour, unsafe attitudes of professionals and its impact on patient care still need to be addressed. Although various tools have been developed to determine OC and improve patient safety, it remains a challenge to decide on the suitability of tools for uncovering the underlying factors which truly impact OC, such as behavioural norms, or the unwritten rules. A better understanding of the underlying dimensions that these tools do and do not unravel is required.
Objectives The aim of this study is to provide an overview of existing tools to assess OC and the tangible and intangible OC dimensions these tools address.
Methods An interpretive umbrella review was conducted. Literature reviews were considered for inclusion if they described multiple tools and their dimensional characteristics in the context of OC, organisational climate, patient safety culture or climate. OC tools and the underlying dimensions were extracted from the reviews. A qualitative data analysis software program (MAX.QDA 2007) was used for coding the dimensions, which resulted in tangible and intangible themes.
Results Fifteen reviews met our inclusion criteria. A total of 127 tools were identified, which were mainly quantitative questionnaires covering tangible key dimensions. Qualitative analyses distinguished nine intangible themes (commitment, trust, psychological safety, power, support, communication openness, blame and shame, morals and valuing ethics, and cohesion) and seven tangible themes (leadership, communication system, teamwork, training and development, organisational structures and processes, employee and job attributes, and patient orientation).
Conclusion This umbrella review identifies the essential tangible and intangible themes of OC tools. OC tools in healthcare do not seem to be designed to determine deeper underlying dimensions of culture. We suggest approaching complex underlying OC problems by focusing on the intangible dimensions, rather than putting the tangible dimensions up front.
- patient safety
- leadership
- organisational culture
- communication
- health policy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Recently a Dutch Academic Medical Centre was the subject of a news-making scandal where a culture of underlying fear in one of their departments contributed to inadequate team performance and decreased patient safety.1 The medical professionals involved were anxious to speak up about complications since they were graded on performance by the department head. Fatal incidents occurred, yet they were not reported. An independent investigation by the Dutch Health Inspectorate confirmed that it remained difficult to understand the underlying reasons to the behaviours and attitudes of medical professionals in this apparent culture of fear. Despite the various available tools to determine organisational culture (OC), and the different attempts to review the available tools, a complete overarching overview of potential tools to use and the criteria for choosing one in such specific cases was lacking. In this case, due to the limitations of the OC tool they were not able to address the problem. Better insight in OC tools and in the key dimensions that these OC tools do and do not determine is necessary to decide on their suitability for each situation and organisation. This is especially important as this is an incident which does not stand alone as a result of a widespread toxic OC, both nationally and internationally. In recent years, multiple Dutch but also international healthcare organisations, such as the National Health Service (NHS), were subject to news-making OC scandals2–4; not to mention cases that are not made public.
In the past 40 years the interest in OC has increased. The importance of OC is emphasised by research that links OC with adverse events, patient safety, professional well-being, competitive advantage and organisational performance.5–8 In 2000, the Institute of Medicine (IoM) also emphasised the importance of safe OC in order to prevent adverse events due to human errors.9 Healthcare organisations were advised to develop a ‘culture of safety’ so that the workforce and processes focus on improving the reliability and safety of the care for patients.9 This advice resulted in a growing trend of developing tools to determine OC. Consequently, many healthcare organisations use OC tools to get insight in their strengths and weaknesses.
OC has been defined in different ways.10–14 A commonly used definition is by Edgar Schein: ‘OC is the pattern of shared basic assumptions—invented, discovered, or developed by a given group as it learns to cope with its problems of external adaptation and internal integration—that has worked well enough to be considered valid and, therefore, to be taught to new members as the correct way to perceive, think, and feel in relation to those problems.’11 Schein describes three levels of OC: (1) artefacts, which are the visual organisational structures and processes, (2) espoused values, which are the organisations’ strategies, goals and philosophies, and (3) basic underlying assumptions, which are the unconscious, taken-for-granted beliefs, perceptions, thoughts and feelings. While the upper levels 1 and 2 can be perceived as the tangible dimensions of OC, the deeper level 3 can be perceived as the intangible dimensions of OC.15
In the literature, ‘OC’ is used interchangeably with ‘organisational climate’. Although OC and organisational climate are both acknowledged to be similar and strongly related concepts, organisational climate is often referred to as the tangible dimensions of culture.16 Tangible dimensions, such as policies, procedures and reward systems, are relatively easy to determine in contrary to determining the intangible dimensions of culture, such as an organisation’s values and beliefs.16 Although OC tools often aim to combine tangible and intangible dimensions in order to display a complete picture,10–12 it is not clear to what extent OC tools achieve this aim and thus measure the deeper underlying assumptions of medical professionals’ functional or dysfunctional behaviour. Thereby, there is no consensus about the dimensions that OC tools should measure.
Since a toxic OC has a considerable impact on healthcare professionals who are already under tremendous pressure due to the increasing complexity of care and personnel shortages, knowledge on how OC tools address the deeper underlying assumptions may help healthcare authorities to purposefully address OC. This study therefore aims to provide an overview of available OC tools and to provide insights in the tangible and intangible dimensions of these tools.
Methods
An interpretive umbrella review was conducted to integrate and synthesise theory from multiple literature reviews17–21 that addressed OC tools. Our methodology was based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.22 For this paper, no approval of the institutional review board was required.
Search strategy
Systematic searches were conducted in collaboration with a medical information specialist. Four electronic databases were searched (ie, PubMed.com, PsycINFO/EBSCO, Business Source Elite/EBSCO, CINAHL/EBSCO) from inception up to March 2019. The following index terms and free-text words were used to search literature reviews (including synonyms and closely related words such as climate): ‘organisational culture’, ‘culture of safety’, in combination with the terms ‘tool’, ‘measure’, ‘questionnaire’ and ‘review’. We combined these terms using Boolean operators and adapted the search strategy to the appropriate syntax of each database.
In addition, an internet search using scholar.google.com was conducted on 13 April 2017 with the term ‘assessing OC in healthcare’ and sorted in the order of highest to lowest relevance. The first 100 records were reviewed and reviews describing tools that measure culture were obtained. Duplicate articles were excluded. The full search strategies for all databases are available from the corresponding author on request.
Eligibility criteria
With the increasing knowledge regarding the benefits of improving the OC, healthcare organisations were advised by the IoM to develop a culture of safety. Therefore, literature reviews were considered for inclusion if they described tools that determined OC or patient safety culture with their dimensional characteristics. In this context, ‘tool’ was defined as ‘a method by which one can collect information on dimensions of OC and which can help determine the OC on its own or as a part of a process’. The search was limited to English articles published after the year 2000. This period was selected as most of the empirical work on OC has been published since 2000 after the published report ‘To err is human’ by the IoM.9 Reviews that did not describe tools in a healthcare setting or did not mention dimensions were excluded. Scientific quality and bias of the reviews was assessed according to the following: whether there was a clear and systematic description of the aim of the study, systematic data collection and analysis methods, results of the study, context and setting of the study, strengths and weaknesses, and implications of the study. Eligibility assessment of the retrieved articles was performed by two authors (RFM and NA) independently (not blinded). In case of doubt or disagreement regarding inclusion or exclusion, a third author (FS) was consulted to establish consensus.
Data extraction
Data extraction was performed by RFM and NA. Each included review was reviewed for the following: year, author, number of tools, focus and purpose of the tool, qualitative or quantitative nature of the tool and the reported (key) dimensions of OC.
Besides the above-mentioned aggregation of data we did an interpretive analysis to synthesise theory. The dimensions of OC tools that were mentioned in the included articles were coded through qualitative data analysis (using software programme MAX.QDA 2007). An overview was created of all OC dimensions, which resulted in a categorisation of dimensions around themes. This process consisted of two phases: first phase, data were categorised with open and axial coding by two researchers (RFM and NA). During open coding, dimensions were coded with a label that summarised the meaning of that dimension; this resulted in a large number of labels. Subsequently, axial coding reduced the number of labels by clustering the content of closely related labels into categories. Finally, connections were made between the categories identified in the axial coding process, also called selective coding. This phase was an iterative process, in which the research team repeatedly discussed until consensus was reached about the key dimensions. The multidisciplinary nature of our review team allowed to incorporate different perspectives into this process. Within the second phase, the key dimensions were categorised according to the three pillars of the conceptual framework of Schein: to achieve a clear distinction between dimensions; artefacts and espoused values were seen as tangible dimensions; and basic underlying assumptions (dimensions that partly concerned perceptions, beliefs, feelings and thoughts) were seen as intangible dimensions.
Results
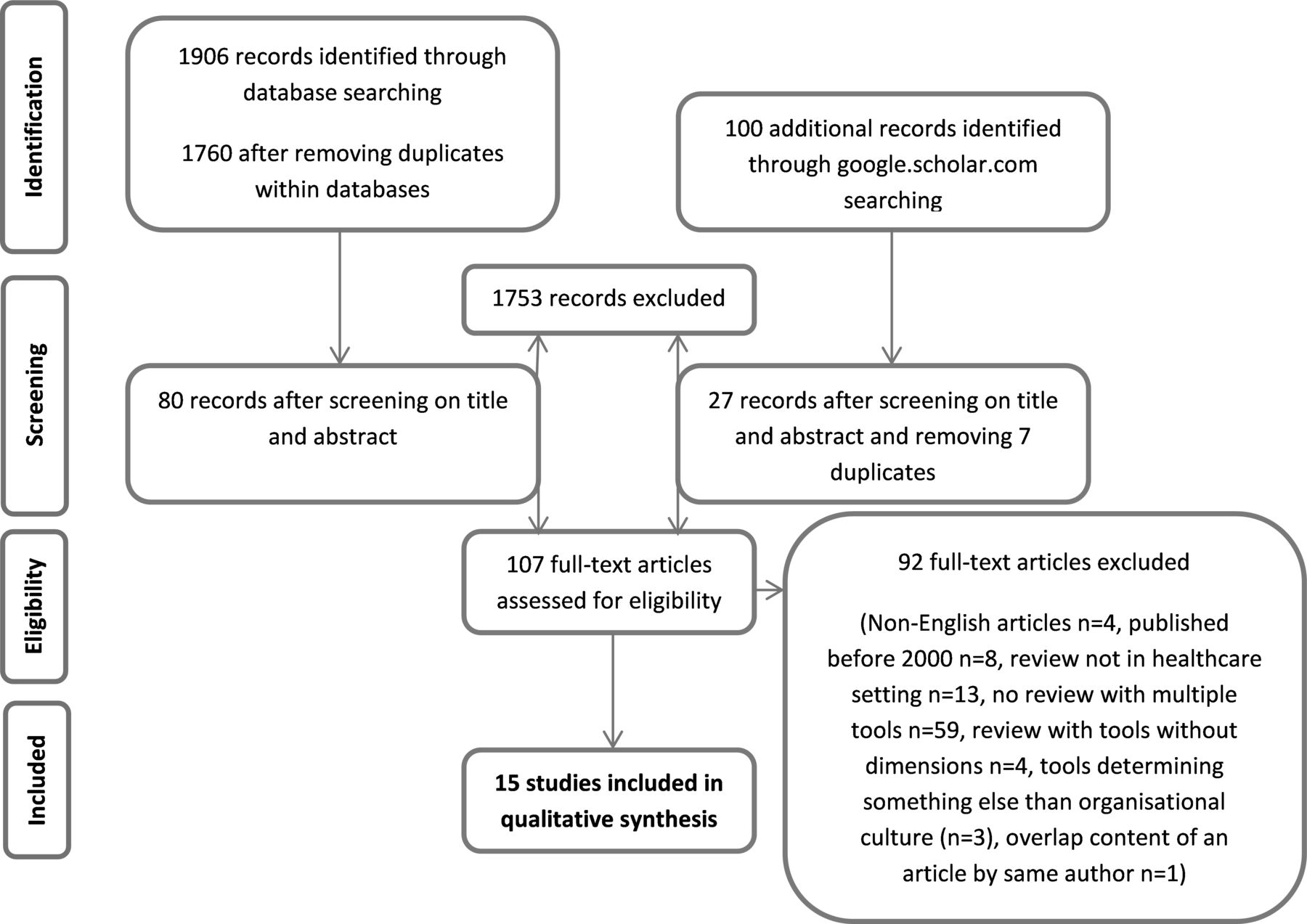
From the systematic searches of the literature, 1760 records were obtained in the four electronic databases and 100 of 227.000 records were obtained in Google Scholar. After screening on title and abstract, respectively, 80 and 27 records were subjected to full review. The flow diagram of the systematic literature search is shown in figure 1. Eventually 15 studies met our inclusion criteria.15 16 23–35
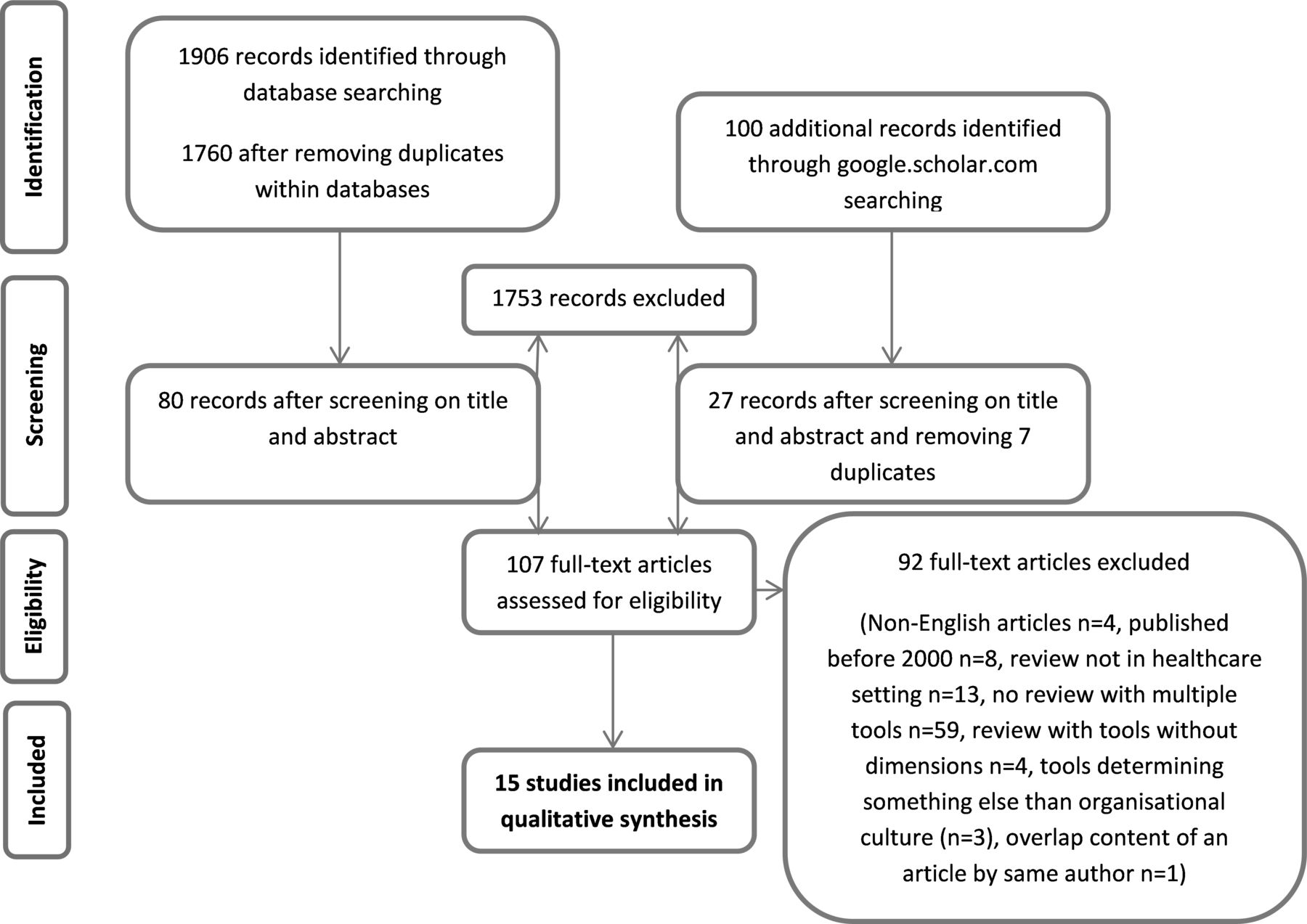
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Online supplementary appendix I lists the 15 studies that met the inclusion criteria and summarises their design and results. Two articles did not specifically aim to review instruments and its dimensions, however they were still included as the presented data gave an overview of instruments and dimensions that fitted our inclusion criteria.15 31 All articles were published between 2002 and 2019. The main findings from reviewing these papers are as follows: 10 of the 15 reviews focused on patient safety climate or culture and the remaining five reviews focused on OC. Although all reviews provided an overview of the available OC tools in healthcare, they varied in the setting and their focus; for example, hospital versus primary care, English NHS versus German-speaking countries, quantitative versus a combination of quantitative and qualitative tools. The majority of the instruments that were included focused on hospital care, some were used in rehabilitation settings and long-term care.
Supplemental material
The 15 reviews presented 209 tools. After deduplication 127 tools were identified, of which the majority were quantitative tools determining a predefined set of dimensions in the form of questionnaires. Seventeen of these tools were qualitative tools or approaches and five of these tools were unclassified due to a lack of information. The qualitative approaches, such as observation, ethnography and interviews, are mentioned in maximum of three articles (online supplementary appendix 1). Other qualitative approaches, such as story-telling and the critical incident technique, are mentioned in one article and are not widely used in healthcare.26 Tools that are widely used and mentioned by multiple reviews include (variations on) the Hospital Survey on Patient Safety Culture in 13 reviews, the Safety Climate Scale (although various variations) in 13 reviews, the Safety Attitudes Questionnaire in 11 reviews, the Patient Safety Climate in Healthcare Organizations Questionnaire in nine reviews and the Organisational Culture Inventory in five reviews. The Nursing Unit Cultural Assessment Tool, the Quality Improvement Implementation Survey, the Operating Room Management Attitudes Questionnaire-modified and the Manchester Patient Safety Framework (MaPSaF) are mentioned in four reviews. All above-mentioned tools use a quantitative approach except for the MaPSaF, which uses a qualitative approach. MaPSaF evaluates the perceptions of safety culture within healthcare organisations by a process of reflection and discussion. The number of tools mentioned per review ranged from 3 to 70, with a median of 11. The majority of tools use a single method regarding the collection of data and determining OC. Eight of the 15 reviews gave an overview of key dimensions of these tools. From the remaining seven reviews, the key dimensions were extracted per tool. The maximum number of key dimensions mentioned in these reviews was 26.
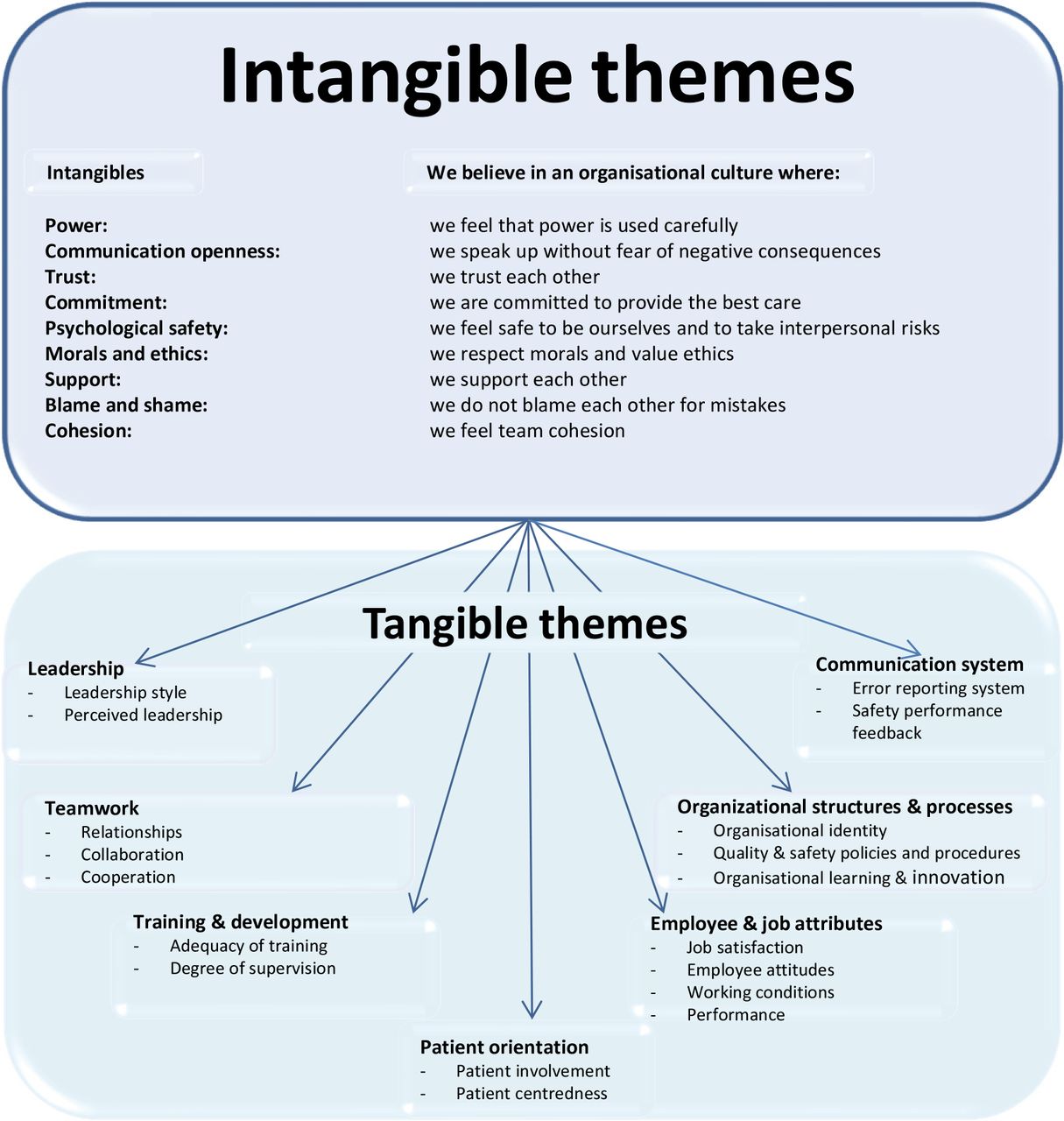
The iterative coding process, as described above as the first phase, resulted in eight themes that covered the key dimensions of OC tools: (1) leadership, (2) communication (could be differentiated in communication system and communication openness), (3) teamwork, (4) training and development, (5) organisational structures and processes, (6) employee and job attributes, (7) patient orientation, and (8) blame and shame (online supplementary appendix 2). Notably, most of the themes (with their subthemes) seemed to be mainly tangible; only the communication openness and blame and shame themes, which mainly focus on a non-punitive response to error, were potentially intangible. There seems to be consensus on the importance of the first five above-mentioned themes as they are virtually covered by all tools. Moreover, leadership and communication system were presented as the most important tangible elements across the tools while patient orientation was scarcely represented as key dimension. The additional coding process according to the concepts of Schein, as described above as phase 2, resulted in nine intangible themes: commitment, trust, psychological safety, power, support, communication openness, blame and shame, morals and valuing ethics, and cohesion. Both intangible and tangible themes are nested at different levels within the organisation: organisation, management, team, individual and the patient level. At least four of the nine intangible dimensions were directly related to the management level: power, trust, commitment and support (figure 2).
Supplemental material

{kind=link}
{kind=link}
Tangible and intangible themes of organisational culture (OC) tools.
Discussion
We performed an umbrella review and identified the intangible and tangible key themes of OC tools. Although OC can be analysed at several different levels,11 the tools which are aimed to determine OC in healthcare do not seem to be designed to explore the deeper underlying dimensions of culture. The mainly quantitative nature of tools, mostly self-reported questionnaires, does elucidate the superficial meanings of culture (ie, tangible themes), yet does not allow to explore the underlying assumptions of culture in depth (ie, intangible themes).36 The focus on a predetermined set of dimensions in these questionnaires and the lack of reasoning behind the answers might reinforce the belief that culture is static and given. This may explain why the Dutch Healthcare Inspectorate had difficulties in understanding the problems that originated in the lack of an open culture. Prior studies have already noticed that there is little agreement about how OC should best be observed or determined and which dimensions should be taken into account.23 The tools that determine OC vary in scope, dimensions and context,16 23 24 which makes it difficult to understand the contextual relevance of tools, but also makes it difficult to know whether fundamental underlying problems in OC are determined. Moreover, a majority of tools focus on tangible dimensions while intangible dimensions are scarcely represented as key dimensions. We would like to discuss a different approach to uncover complex underlying problems by focusing on the intangible dimensions that assess the emotional dimensions, rather than putting the tangible dimensions that elicit the rational responses up front.
In the search to uncover this deeper level, or the intangible dimensions of OC, it is often observed how values govern behaviour.11 Since it is difficult to observe values directly and add meaning to it, Schein emphasises the importance of combining methods such as documents and charters with interviews of key members. However, these identified values usually only represent the manifest values of a culture accurately; they focus on what people say is the reason for their behaviour, what they ideally would like those reasons to be and often what their rationalisations are for their behaviour, while the underlying reasons for their behaviour remain unclear.11 If certain motivational processes are repeated and continue to work in a certain way, the assumption drops out of awareness and is increasingly taken for granted. These taken-for-granted assumptions are powerful as they are less debatable and confrontable compared with espoused values. Schein emphasises that delving into these underlying assumptions is imperative to really understand OC and ascertain the group’s values and overt behaviour. These assumptions reflect the actual perceptions, thoughts and emotions of group members. Moreover, Schein reasons that these assumptions can only be brought back to our consciousness by doing a focused inquiry that requires the efforts of both an insider and an outsider, respectively, someone who has the unconscious assumptions and someone who helps to uncover the assumptions by asking the right kind of questions.11
As the deeper underlying assumptions within culture are most difficult to grasp yet enormously set the mood, we believe that the identified intangible dimensions should be the primary base for a focused inquiry. These intangible dimensions encourage us to focus on connecting the thoughts and feelings to underlying needs and values within an organisation. However, a focused inquiry requires knowledge about the right topics to base the questions on and framing questions requires skills and practice.37 38 On the one hand, questions must explore the interviewer’s topic and be sufficiently general to cover a wide range of experiences, while on the other hand they should be narrow enough to fit, elicit and elaborate the participant’s specific experience.37 The data can be forced by interviewers by asking the wrong questions, but also by how they pose, emphasise and pace their questions. The wrong questions fail to explore pivotal issues or to elicit participants’ experiences in their own language.37 In addition, power dynamics, gender, age and race should be taken into account as they may affect the direction and content of interviews. Although intensive interviewing, observations and questionnaires are often used as a single method as was confirmed by this research,37 38 single approaches do not seem to sufficiently uncover the deeper underlying dimensions.11 13 26 27 36 A complex subject as OC requires a focused approach with the use of different methodologies that complement each other. For example, concept mapping and pattern matching is a tool that combines qualitative and quantitative aspects.39 Such tools would be preferred over the single approaches. Although this tool has seen previous application in healthcare, it is not widely used; healthcare organisations remain conducting their usual yearly quantitative measurements to measure OC.
If organisations really want to change their culture to benefit professionality and patient care, they should invest properly on a mixed method that suits their perspective and the aim of determining OC to elucidate its deeper level. In addition, an organisation should consider a practical approach that fits the setting to reduce potential negative impact on outcomes of the used method. Change requires big investment and considering the further complexities of OC and pinpointing the change needed through using the right set of tools, it therefore requires even greater investment. A focused inquiry with the intangible dimensions up front and collaboration between insiders and outsiders may help get a more realistic view of the OC.11 Although the context should be leading for the content of a focused inquiry and there are different ways to observe OC, we recommend healthcare organisations to use tangible core dimensions as subtopics within the intangible main topics; in particular the tangible element ‘Leadership’. Consistent with the literature, leadership behaviour determines OC to a large extent and is therefore essential to achieve a complete image of any OC.11 Another important theme that deserves continuous attention is ‘Communication system and openness’ with its tangible and intangible nature. Open communication or speaking up remains difficult for different professional groups. The hierarchical structure of healthcare organisations and the increasingly implemented strategy of ‘physicians in the lead’ do not seem to contribute to open communication.40–44 Moreover, important dimensions might not be identified by tools if participants consider them unimportant or conceal them on purpose to prevent potential negative consequences of speaking up.10 36 37 45 To effectively prevent such behaviour and realise a healthy OC, learners should feel they can challenge authority in practice and learn when and how to speak up and give adequate concrete feedback to their superiors, but also to their peers and subordinates.41 43 44 Moreover, in today’s competitive healthcare market, where healthcare organisations continuously have to determine and improve culture to recruit and retain qualified employees,16 healthcare organisations could continuously build on a healthy OC by structurally addressing and discussing the tangible and intangible OC dimensions. Leaders are key figures to realise the above-mentioned and to implement open conversations about OC as they serve as an example for the rest of the team. A third theme that deserves attention is patient orientation. Although it was not taken into account by the majority of tools as key dimension, we expect it to be increasingly important in the development of tools since the upcoming trends of patient involvement, participation and patient-centred care.
Using the umbrella review method allowed us to summarise the overall body of knowledge available on a topic with the goal of answering a specific question.19 This umbrella review was limited by the quality and comprehensiveness of the original systematic reviews. As a distillation of many systematic reviews, an umbrella review is two steps removed from the original studies that are included. Therefore, for some this type of knowledge synthesis may not yield the level of detail necessary for implementing findings into practice without needing to revisit the original studies or systematic reviews.
Although we gained insight in OC tools and the authors delved into the theoretical foundations behind the tools, we recommend to explore the following in future research: (1) how OC tools in healthcare resemble original culture theory and tools in other settings, and (2) whether the themes are applicable to other contexts than the Western context as the themes in this study are based on OC tools that were mainly developed in the Western setting.
Conclusion
With this umbrella review we have identified the essential (in)tangible themes of OC tools. OC tools in healthcare, which are mainly quantitative questionnaires for a hospital-based setting, do not seem to be designed to determine deeper underlying dimensions of OC. Tools mainly cover tangible key dimensions that elicit rational responses. An approach that combines different methodologies to determine the intangible key dimensions beneath the surface is required.
Acknowledgments
We thank Chantal den Haan, medical information specialist, for her contribution to the systematic search strategy.
References
Footnotes
Contributors RFM, MBS, NA, CH and FS contributed to the conception and development of the study, project management, reporting and publication. RFM and NA collected and extracted the data. RFM, MBS, NA and FS contributed to the interpretive analysis of the data. RFM prepared the first draft of the manuscript. RFM, MBS, NA, CH and FS were involved in drafting and revising the manuscript and have given final approval of the version to be published. RFM takes responsibility for the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.