Article Text

Abstract
We carried out a quality improvement (QI) project (QIP), aiming to improve the quality, safety and equity of healthcare provided for homeless patients attending the emergency department (ED). We used QI methodology to identify areas for improvement, and introduced and modified interventions over four Plan, Do, Study, Act cycles. We launched a departmental ‘Homeless Health Initiative’ (HHI), the chief intervention being the provision of ‘Homeless Health Boxes’ in the ED, which contained a ‘Safe Discharge Checklist for Homeless Patients’, maps to specialist homeless general practitioner surgeries and homeless day centres, information on other inclusion health services, copies of a local rough sleepers’ magazine and oral hygiene supplies. Voluntary Homeless Link Nurses and a number of informal ‘Homeless Health Champions’ were appointed. The HHI was embedded in departmental awareness through regular presentations to staff and incorporation into the induction programme for new doctors. Staff satisfaction, in terms of how satisfied staff members were with the care they were able to provide for homeless patients in the ED on a 0–10 scale, improved modestly over the course of the QIP from median 6/10 to median 7/10. The number of staff who were severely dissatisfied with the care they were able to provide for homeless patients improved more markedly: first quartile staff satisfaction improved from 3.875/10 to 6.125/10. Staff compliance with the checklist was poor, with full compliance observed in only 15% of cases by the end of the QIP. An HHI is a cheap and worthwhile QI project, with the potential to significantly improve the quality, safety and equity of healthcare provided for homeless patients, while improving staff satisfaction concurrently. Similar initiatives should be considered in any ED which sees a significant number of homeless patients.
- patient discharge
- emergency department
- harm reduction
- healthcare quality improvement
- patient safety
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
‘Nothing is a better reminder of inequality and human suffering than a rough sleeper.’- Victor Adebowale, Chief Executive, Turning Point, 20181
St Thomas’ Hospital is a teaching hospital in central London, with over 175 000 emergency department (ED) attendances per year.2 Though located in the Borough of Lambeth, it is situated immediately across the River Thames from the Borough of Westminster, the local authority with the highest number of rough sleepers in England (a local authority is a unit of local government responsible for running the public services and facilities in a particular area).3
There were 142 people living on the streets in Westminster in July to September 2019 (plus 355 intermittent rough sleepers); the corresponding figures for Lambeth were 19 and 78, respectively.4 The total estimated number of people sleeping rough in England on a single night in 2018 was 4677, of whom 1283 were in London.3 The total homeless population of London (including those in temporary accommodation, homeless hostels and rough sleepers) was estimated at 168 000 in 2018, accounting for more than half of Great Britain’s total estimated homeless population of 320 000.5
In comparison to previous years, the above figures represent a general upward trend in terms of the numbers of homeless people. For example, Great Britain’s total homeless population increased by 13 000 between 2017 and 2018, with London seeing an increase of 3488. For rough sleepers, the increase was from 4447 to 5096 Great Britain-wide, and from 964 to 1137 in London.5 6 At local authority level, the number of people living on the streets in Westminster increased by 27 (from 115 to 142) between 2017/18 Q2 and 2018/19 Q2, with the number of intermittent rough sleepers falling by 78 (from 433 to 355). The corresponding figures for Lambeth showed no change in the number of people living on the streets, with the number of intermittent rough sleepers increasing by 12 (from 66 to 78).4 Annual rough sleeper ED attendances to St Thomas’ are estimated to have been 753 in 2018, and 648—up until 17th December—in 2019.7
People experiencing homelessness and other forms of social exclusion experience extreme inequity, premature morbidity and mortality.8 Due to barriers in accessing preventative and scheduled healthcare,9 homeless people have some of the poorest health outcomes in society.10
The primary aim of this quality improvement (QI) project was to improve the quality, safety and equity of healthcare delivered to homeless patients in the ED through the use of Homeless Health Boxes, which contained our Safe Discharge Checklist for Homeless Patients (SDCfHP) and other resources. The secondary aim of the project was to improve ED staff satisfaction with their ability to care for homeless patients in the ED. A time limit of 12 months was set.
Background
We completed a detailed evidence review using search terms including ‘discharge checklist AND homeless’, ‘checklist AND homeless’, ‘discharge AND homeless’, ‘“emergency room” AND homeless”, and ‘“emergency department” AND homeless’. We also reviewed the grey literature because the evidence in this field is disparate and often recorded in reports and non-peer-reviewed publications.
Discharging homeless patients: general considerations
Hospital discharge is a high-risk area in the management of homeless patients.11 Critical social needs often go unaddressed in the healthcare setting, leading to a vicious cycle of poverty and illness.12 Most emergency physicians have little knowledge of available resources for homeless patients,13 despite the requirement for a holistic approach.14
National policy
Although the UK Department of Health have repeatedly highlighted the importance of acute hospitals and local authorities having admission and discharge protocols for people experiencing homelessness,15 16 a 2010 report found that only 39% of areas had such a protocol in place.17 Accessing housing as a homeless person in England involves a process of demonstrating a local connection to a particular area and priority need.18 The moral imperative to refer homeless patients to a local authority for housing support is now supported by a legal imperative; the Homelessness Reduction Act (2017) places a legal duty on specified public authorities in England to refer service users who they think may be homeless or threatened with homelessness to local authority homelessness/housing options teams. Such public authorities in the NHS include EDs, urgent treatment centres and hospitals (in their function of providing inpatient care).19 A generic referral form is available on the UK government website.20
Service interventions and UK EDs
Research has shown how specialist hospital homeless teams can in-reach to improve care of admitted patients,21 but there has been little research on how to improve care in ED settings.
A recent national inclusion health clinical audit of EDs identified that homeless people received little advice and signposting to access primary care and other services suggesting a missed opportunity.22 Other common omissions included failure to take a drug and alcohol history, failure to refer patients in whom drug or alcohol use was the direct cause for presentation to specialist services, and failure to refer patients with an acute mental health problem to liaison psychiatry.23
ED-relevant service interventions trialled at UK hospitals include: the provision of information resources for staff via the intranet, ward manuals and posters; attendance at ED frequent attender meetings by homeless link workers to provide advice to staff and support to patients identified as frequent attenders; provision of ‘comfort bags’ to homeless patients, containing, for example, clothing, hygiene supplies, information about local services and cards containing empowering messages24; formalising of a hospital admission and discharge protocol for homeless patients, attending to processes within the ED, on hospital wards and for patients who self-discharge25; and a peer advocacy scheme based in the ED, training formerly homeless people to mentor patients who are currently homeless, encouraging them to keep appointments.26
Recommendations for ED practitioners, following a pilot project which delivered intermediate care for homeless people in Lambeth, were as follows:
Place known frequent attendees on an alert system that includes details of who to contact for information about them.
Establish whether the person is a rough sleeper, attends a day centre or lives in a hostel and, if possible, contact the outreach workers or day centre or hostel workers for client histories.
Quickly establish a regimen to reduce alcohol and drug withdrawal symptoms, helping to reduce self-discharge, inappropriate management and challenging behaviour.
Recognise that homeless patients may have literacy, linguistic or cognitive problems.
Remember that homeless people can take time to trust others and can have poor impulse control.
Build links with local GP practices that specialise or are interested in treating homeless people.
Refer clients to local homeless services, if appropriate.
Develop resource packs for new staff.
Address mental distress appropriately.
Refer patients to the local homeless health team on discharge.27
While not specific to emergency medicine, Groundswell’s peer research evidence has made an important contribution to the evidence base relating to the health of homeless people. For example, the Healthy Mouths peer-led audit on the oral health of people experiencing homelessness recruited 262 currently homeless subjects, providing data on the prevalence of oral health problems among this population.28 Guy’s and St Thomas’ NHS Foundation Trust is fortunate to have a peer advocate from Groundswell.
International interventions
Researchers in Seattle, Washington, USA described a framework for the care of the homeless inpatient, by means of a mnemonic checklist, ‘A SAFE DC’:
A=assessing housing status.
S=screening and prevention.
A=address primary care issues.
F=follow up care.
E=end-of-life discussions.
D=discharge instructions.
C=communication method after discharge.29
ED patients at a Chicago, Illinois, USA hospital were provided with a booklet giving information on alcohol and mental health services, clothing, meals, medical services, shelters, youth services and important numbers.13 In Toronto, Ontario, Canada, a trial of ‘compassionate contact’ with homeless ED patients by trained volunteers significantly reduced subsequent ED attendances in the intervention group.30 Finally, clinicians in Paris, France, were able to provide transfer to shelters and clothing for homeless patients through employing social workers in their ED.31
Public health and the ED
The potential for EDs to support broader public health outcomes, rather than simply emergency treatment of illness and injuries, is increasingly recognised.32 Initiatives to combat, for example, smoking,33 alcohol misuse34 and intimate partner violence35 are well established. The comparative lack of studies concerning ED-specific public health interventions aimed at tackling homelessness is therefore incongruous.
Measurement
We measured:
Staff compliance with a'safe discharge checlist for homeless patients' (SDCfHP), as follows:
SDCfHP in patient’s notes?
If in notes, SDCfHP fully completed? Partially completed? Not completed at all?
Homelessness-specific satisfaction score in surveys administered to ED staff (advanced clinical practitioners, doctors, nurses, physician associates), as follows:
‘On a scale of 0–10, how satisfied are you with the care you are able to provide for homeless patients at St Thomas’ Hospital ED?’
We were fortunate that this was the only quality improvement project (QIP) targeting healthcare for homeless patients active in our ED during the study period, meaning that any observed improvement in the above measures could reasonably be attributed to our QIP.
Measures: specifics and rationale
1) Staff compliance with an SDCfHP
We asked all ED staff treating homeless patients to complete the SDCfHP and file it in their patient’s notes, whether the patient was being admitted to hospital or discharged from the ED.
To measure staff compliance with the SDCfHP, we analysed the notes of 20 homeless patients attending the ED over a 2-week period bimonthly, as part of four Plan, Do, Study, Act (PDSA) cycles. We included the first 20 homeless patients in each 2-week period, and excluded reattenders who had already had a previous attendance within this 2-week period analysed.
At baseline, no patients had an SDCfHP in their notes (we introduced this checklist during the first PDSA cycle).
To minimise sampling errors when measuring compliance with the SDCfHP, we scrutinised the notes to ensure that only genuinely homeless patients were included in the analysis.
We identified homeless patients using the Symphony e-audit tool by postcode: patients without an address are given the postcode ‘ZZ99 3VZ’ by ED reception staff on booking in, making identification of homeless patients straightforward.
Using this method of identifying homeless patients does, however, miss many homeless hostel residents and homeless people in temporary accommodation, and those who are sofa-surfing. This was acceptable to us as rough sleepers were the subgroup of homeless patients for whom we were most keen to improve care: rough sleeping is the most dangerous form of homelessness,36 with the highest death rate37 and ED attendance rate.38
We chose to measure compliance with the SDCfHP because we felt that the process of completing the SDCfHP was central to improving the quality of care provided to homeless patients in the ED. Furthermore, as the SDCfHP was a paper form designed to be placed in the patient’s ED notes, which were subsequently scanned and uploaded to the departmental IT system (Symphony), staff compliance with this checklist was easy to measure.
2) Homelessness-specific satisfaction score in surveys administered to ED staff
We surveyed a convenience sample of ED staff on the ‘shop floor’ on three different occasions, as part of the first, between the second and third, and as part of the fourth PDSA cycle. All surveys were carried out by the corresponding author (CA), optimising consistency of administration. Median staff satisfaction at baseline was 6/10, and first quartile staff satisfaction at baseline was 3.875/10. We chose to measure staff satisfaction with the care they were able to provide for homeless patients because this was straightforward to measure, is a worthy goal in itself, and can also be seen as a proxy for the quality of care provision.
One of the themes we identified early on in the project was that ED staff often felt troubled by their encounters with homeless patients, and felt limited in terms of their ability to help them. Evidence recognises the occupational trauma and emotional impact of managing complex and overlapping needs in limited time in ED settings.39 Staff describe difficulty in managing complex consultations in limited time, and feeling disenabled to do more to help patients. Key challenges, therefore, include maintaining a holistic, patient-centred approach to the care of homeless patients in the ED in the face of conflicting demands such as departmental overcrowding and long waits to be seen.
We considered measuring the satisfaction of homeless patients themselves; however, this proved impractical, as surveys had to be carried out on the CA’s allocated non-clinical days, and it was not possible to collect an adequate dataset on these sporadic days.
Design
Interventions
‘Homeless Health Boxes’, placed at several locations within the ED. These contained (see online supplementary files 1–5):
The SDCfHP.
Maps to local specialist homeless and homeless-friendly general practitioner (GP) surgeries.
Maps to local homeless day centres.
Copies of The Pavement magazine (containing information on services for rough sleepers).
Following staff feedback, we subsequently included:
Information on services provided by the specialist Pathway Hospital Homeless Health Team (a charity, employing NHS staff, which provides integrated healthcare for homeless people), the Health Inclusion Team (a nurse-led community homelessness team), Trust and community alcohol services and local sexual health services.
Supplies of toothpaste, toothbrushes and denture paste.
Appointment of two Homeless Link Nurses and one Homeless Link Clinical Assistant Practitioner.
Appointment of a number of informal ‘Homeless Health Champions’ intradepartmentally to promote the project; these enthusiasts were given badges to wear to raise awareness of the project.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
In addition to the above, we:
Arranged for the Homeless Health Initiative (HHI) to be mentioned in the ED induction programme for new doctors.
Created a slideshow on the initiative so that it could be promoted regularly at departmental handover meetings.
Made the initiative’s core documents (the SDCfHP, maps to specialist homeless and homeless-friendly GP surgeries and maps to homeless day centres) available on the Trust intranet, enabling their use in non-ED contexts.
Publicised the initiative intradepartmentally, within the broader Acute Medicine directorate and among stakeholders from the wider inclusion health community.
We developed our chief intervention (the creation of Homeless Health Boxes) after consulting with local experts on how best to improve the care we provided for homeless patients, given the demands of a busy ED. The boxes provided a structured approach to the care of homeless patients (via the SDCfHP), and quick interventions to improve aftercare.
The main problem we anticipated with our project was the failure of colleagues to engage with it, due to the conflicting demands of ED work.
We tried to ensure sustainability of the project by embedding the initiative within the ED, as described above.
Project team and consultees
Our core team comprised an EM specialty trainee, an EM senior clinical fellow with a special interest in homeless healthcare, a specialist homeless GP who also works part-time in our ED’s Urgent Care Centre and an EM consultant with a special interest in inclusion health. We were assisted by two Homeless Link Nurses, a Homeless Link Clinical Assistant Practitioner and a number of informal ‘Homeless Health Champions’.
We consulted widely, including our ED’s Clinical Lead and Matron, the Trust’s Alcohol Care Team, the Health Inclusion Team, our local specialist Pathway Hospital Homeless Health Team and managers at a local homeless day centre. This provided valuable insight into the services available for homeless patients, into which interventions were likely to be feasible/useful and helped promote our project.
Strategy
Strategy for improvement
We based our methods on a combination of evidence, stakeholder engagement and practicalities of time and resource. Having identified a target for improvement—the standard of healthcare provided to homeless patients in the ED—we used a ‘fishbone’ cause and effect diagram to examine the causes of suboptimal healthcare provision, and help identify areas for improvement.40 We used PDSA QI methodology throughout our QIP,41 and have plotted our interventions against time on a Gantt chart (see online supplementary files 1–5).
Equity, justice and the inverse care law
In an age where healthcare systems are increasingly focused on efficiency and cost-effectiveness, this QI project provided an opportunity for staff to stand alongside the patient at a time when they were amenable to thinking about their health. Its justification was as much about healthcare ethics as it was about outcomes. The inverse care law dictates that the poorest and most in need receive the least care, and so it is with homeless patients, who are often discharged to a dangerous environment with limited recourse to follow-up, despite a high prevalence of morbidity. We hoped that our QI project, in aiming to improve the healthcare of homeless patients, may have served as a starting point to achieving more equitable and just care for this population.
Results
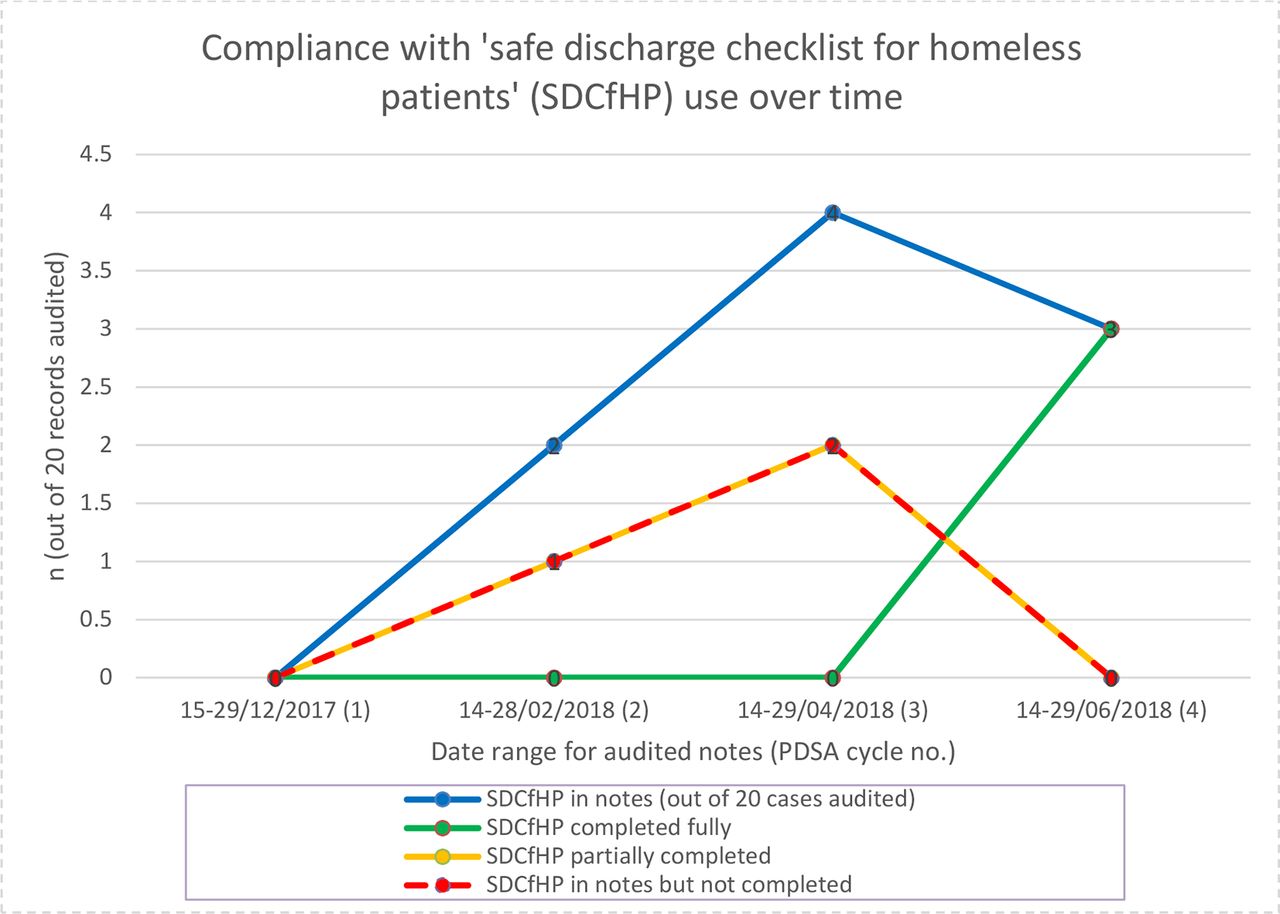
Staff compliance with the SDCfHP is displayed in the following line chart (figure 1):

Compliance with 'safe discharge checklist for homeless patients' (SDCfHP) use over time
Each date on the x-axis corresponds to a PDSA cycle.
The SDCfHP was introduced prior to the second PDSA cycle.
Only 15% of patients (3 of 20, green line) had an SDCfHP fully completed by the final PDSA cycle.
At best, 20% of patients (4 of 20, blue line) had an SDCfHP in their notes (this was achieved during the third PDSA cycle).
If an SDCfHP was present in the notes, it was completed only partially half of the time during PDSA cycles 2 and 3 (dashed yellow line); none were partially completed during the final PDSA cycle. A similar number of patients had a blank SDCfHP left in their notes (dashed red line).
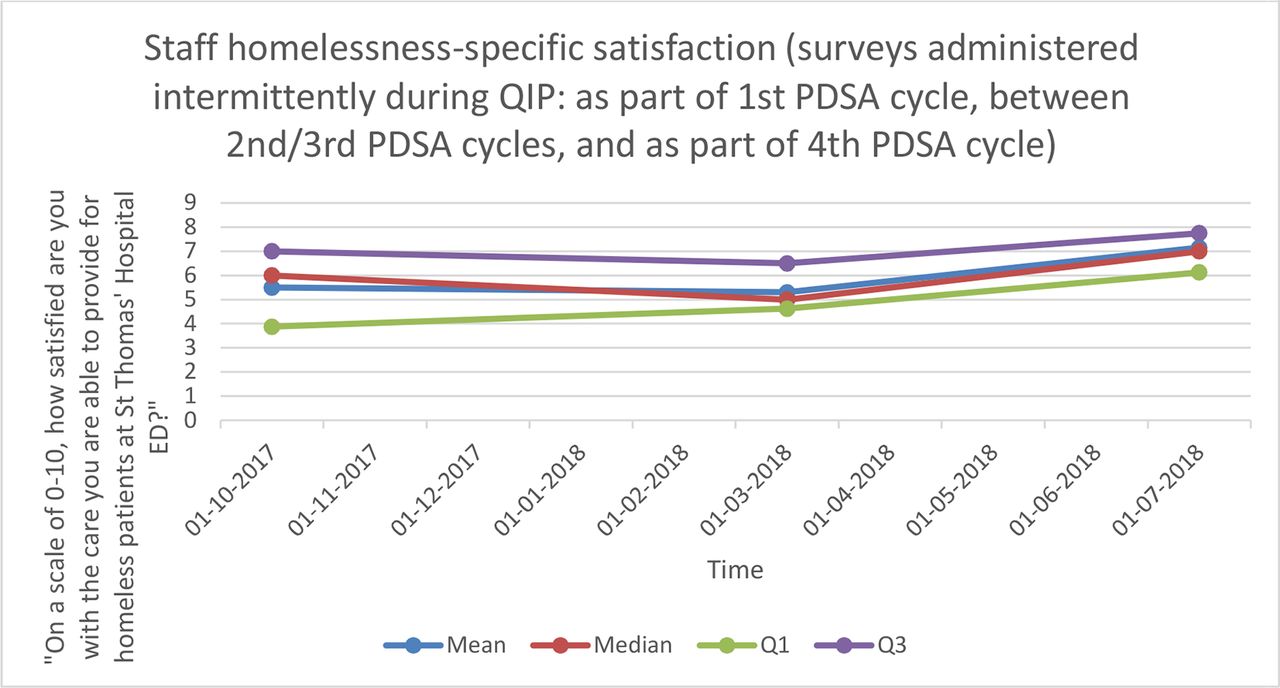
Staff homelessness-specific satisfaction is displayed in the following line chart (figure 2):
{kind=link}
{kind=link}
Staff homelessness-specific satisfaction
Staff homelessness-specific satisfaction, on a scale of 0–10, is displayed on the y-axis; mean and median scores, as well as first and third quartile scores, are displayed.
The x-axis displays time, with the dots coinciding with (1) the first PDSA cycle, (2) the cross-over period between the second and third PDSA cycles and (3) the fourth (and final) PDSA cycle.
The graph shows that median satisfaction was 6/10 at the start of the QIP, and 7/10 towards the end of the QIP.
The more marked rise in satisfaction at the Q1 (first quartile) level, from 3.875/10 to 6.125/10, is likely to represent a substantial reduction in the proportion of staff who were markedly dissatisfied with the care they were able to provide for homeless patients by the end of the QIP.
Data collection was complete and accurate for both measures (electronic notes were scrutinised systematically, and staff surveys were undertaken in a reproducible and consistent manner).
Lessons and limitations
Strengths
This QIP aimed to improve the healthcare provided to arguably our most disadvantaged local population. As a tool in the struggle against health inequity, therefore, we considered even minor successes worthwhile.
The QIP drew much-needed attention to a patient group that is frequently neglected.
The interventions carried out were cost-effective. The CA was allocated two non-clinical days every 9 weeks to work on the QIP. Material costs were low and consisted solely of stationery, printing and the cost of plastic storage boxes.
The Homeless Link Nurse roles and Homeless Link CAP role were voluntary positions taken on by substantive staff—this helped to embed the HHI as an integral part of the service offered by the ED.
While compliance with the SDCfHP was poor, sustained staff engagement with other aspects of the QIP have been much better. One year on from the end of the QIP, for example, the number of maps (to specialist homeless GP surgeries and day centres) distributed to patients remains high.
The authors are fortunate to have a number of colleagues from across the Trust, community services for people experiencing homelessness and the specialist Pathway Hospital Homeless Health Team, who are enthusiastic supporters of the HHI.
Limitations and reflection
The introduction of the Homelessness Reduction Act in April 2018, part-way through the QIP, rendered the SDCfHP out-of-date with regard to the statutory duty to refer.
The SDCfHP does not include a mechanism for contacting street outreach providers in the area in which a rough-sleeping patient is to be found (as recommended in the 2006 joint Department for Communities and Local Government and DH report);16 this could be considered in future checklists.
While we took steps to promote the HHI at induction when new doctors rotated into the ED, we did not target the inductions of non-medical ED staff. Furthermore, after the CA left the Trust, the HHI was no longer reliably included in the induction programme for doctors, but instead was promoted on an ad hoc basis by enthusiasts.
The authors intended to create an automated prompt on Symphony (the St Thomas’ ED patient management computer system), reminding clinicians to complete the SDCfHP when they ‘click on’ a patient who is homeless, and again when they come to discharge the patient off Symphony. Implementation of this intervention had to be postponed for technical reasons.
The importance of improving healthcare delivery for homeless patients is likely to be generalisable to other hospitals which serve large homeless populations. For hospitals which see few homeless patients, the opportunity cost of launching an HHI may be outweighed by other demands.
The use of convenience sampling when administering surveys may have introduced bias.
Compliance with the SDCfHP may have been adversely affected by its length; the ideal SDCfHP would be brief and integrated into the casualty notes. The use of a separate, remotely located form may also have been a barrier to compliance.
Conclusion
Staff satisfaction was positively associated with the launch of the HHI. Staff compliance with the SDCfHP, however, was poor. To the authors’ knowledge, no prior studies looking at our outcome/process measures exist.
The impact of the QIP on the ED has been positive—staff surveys point to improved staff knowledge with respect to the management of homeless patients, and diminished feelings of powerlessness when confronted with homeless patients.
Poor compliance with the SDCfHP can be attributed to a number of possible factors:
Clinicians seeing the SDCfHP as ‘yet another form’, to be avoided if possible.
Lack of awareness about the SDCfHP, for example, among bank/locum staff.
Staff seeing use of the SDCfHP as optional, rather than mandatory.
Staff being unaware of the perceived benefits of using the SDCfHP.
Staff seeing homelessness as a non-medical issue, and one which they need not engage with. Despite the compelling evidence that homelessness is associated with appalling health outcomes, ‘healthcare staff are still reluctant to accept homelessness as a healthcare matter’.42
We believe that this was a useful QIP which has contributed to a sustainable improvement in the quality, safety and equity of healthcare delivered to homeless patients, as well as an improvement in staff satisfaction in terms of their subjective ability to care for homeless patients in the ED.
Implications for practice
All EDs which see a significant number of homeless patients should consider an HHI as a low-cost intervention with the potential to improve healthcare delivery for homeless patients, as well as staff satisfaction.
Further studies should address
How compliance with checklists such as the SDCfHP can be improved.
How such checklists can be made more robust, for example, by including contact with community inclusion health/street outreach teams.
How follow-up communication with these teams and GPs can be improved.
Extending the reach of the study to ensure that all homeless patients, not just (predominantly) rough sleepers, are included.
Suggested next steps include
Updating the SDCfHP in light of the April 2018 Homelessness Reduction Act.
Assessing ED performance with respect to homeless healthcare nationwide, as part of the RCEM national audit programme.
Acknowledgments
The authors thank all of the team members and consultees for their support with the project, the BMJOQ editorial team and the expert reviewers. CG would also like to thank: Potenza Atiogbe, Marisa Martinez Ortiz and Yin Ping Leung of the Hirson Library, Epsom and St Helier University Hospitals NHS Trust; Lynsey Hawker of The King’s Fund; the Housing and Support Services/Rough Sleeping Team Managers at The Passage charity; Amir Hassan for his review of the QIP and Koorosh Alaghmand for his supervision.
References
Footnotes
Contributors CG conceived the project, designed data collection tools, undertook data collection, analysed the data, implemented the interventions, drafted and revised the paper. He is guarantor. SH advised on local resources for homeless people and on suitable interventions and measures, designed the maps, helped implement the interventions and revised the paper. LH helped implement the interventions, with ancillary data collection and revised the paper. AW advised on suitable interventions and measures and revised the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.