Article Text

Abstract
Background Globally most neonatal deaths occur within the first week of life and in low-income and middle-income countries. Strengthening health system linkages for frontline providers—such as lay midwives providing home-based obstetrical care—may improve neonatal outcomes in these settings. Here, we conducted a quality improvement study to increase the detection of neonatal complications by lay midwives in rural Guatemala, thereby increasing referrals to a higher level of care.
Methods A quality improvement team in Guatemala reviewed drivers of neonatal health services provided by lay midwives. Improvement interventions included training on neonatal warning signs, optimised mobile health technology to standardise assessments and financial incentives for providers. The primary quality outcome was the rate of neonatal referral to a higher level of care.
Results From September 2017 to September 2018, participating midwives attended 869 home deliveries and referred 80 neonates to a higher level of care. A proportion control chart, using the preintervention period from January to September 2017 as the baseline, showed an increase in the referral rate of all births from 1.5% to 9.9%. Special cause was obtained in January 2018 and sustained except for May 2018. The proportion of neonates receiving assessments by midwives in the first week of life increased to >90%. A trend toward an increasing number of days between neonatal deaths did not attain special cause.
Conclusions Structured improvement interventions, including mobile health decision support and financial incentives, significantly increased the detection of neonatal complications and referral of neonates to higher levels of care by lay midwives operating in rural home-based settings in Guatemala. The results show the value of improving the integration of lay midwives and other first responders into neonatal systems of care in low-resource settings.
- community health services
- control charts/run charts
- global health
- infant mortality
- mobile applications
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Rural indigenous communities in Guatemala have some of the worst neonatal outcomes in Latin America.1 Many births in rural Guatemala occur in the home, under the care of lay midwives. In addition to encouraging and fostering acceptance of facility-level births among the population, working to improve midwives’ capacity to assess and refer neonates to facility-level care when births do occur in the home is an important area where systems of care could be improved.
Wuqu’ Kawoq | Maya Health Alliance is a nonprofit primary healthcare system based in rural Guatemala. Since 2015, we have been working closely with lay midwives and regional public health authorities to improve workflows around the detection of maternal and neonatal complications and increase referrals of patients in need of high-level care. This work has included the development of mobile health technology to help midwives standardise their workflows and connect them with on-call medical teams who assist with triage. The use of this technology and back-up support has increased rates of obstetrical referrals to hospital care by >50%.2 However, similar improvements in the referral of neonates have not been observed. In fact, in the baseline period prior to the improvement project we report here, the rate of neonatal referral was only 1.5% of all live births. In comparison, high-quality prospective data from the region of Guatemala where we work have shown low birth weight rates of at least 10%, suggested that an ideal detection and referral rate of neonates for paediatric evaluation should be at least this high.3
With the goal of improving the neonatal referral rate among our collaborating midwives, we convened a working group of midwives and clinical and administrative staff from Wuqu’ Kawoq | Maya Health Alliance to investigate key drivers of neonatal care. Several key themes for improvement were discovered. First, both midwives themselves and many of the supporting clinicians providing triage support through mHealth felt insufficiently trained in neonatal assessment techniques and warning signs. Second, midwives’ mHealth interface lumped the neonatal assessment into the maternal intrapartum and postpartum visit, leading to them frequently skipping the assessment due to clinical attention to the mother. Third, many midwives with low numeracy skills felt interpreting birth weights to classify neonates as a low birth weight to be a significant challenge. Finally, as families reimbursed midwives only for maternal care, there was no specific incentive to spend extra time and effort on neonatal assessments.
With these findings in mind, our SMART (Specific, Measurable, Achievable, Relevant, and Timely) aim for this improvement project was to improve the proportion of neonates born at home under the care of midwives who were referred to a higher level of medical care to 10% within 6 months and, subsequently, to show sustained improvement over an additional 6-month period.
Introduction
Improving the continuum of care for neonates in rural, lower-resource settings is an important global health concern. According to the WHO, 2.5 million neonates die annually around the world, with most of those deaths in the first week of life.4 Improving neonates’ access to skilled healthcare providers is a critical priority. The rural areas of Guatemala have one of the highest neonatal mortality rates in Latin America.1 In line with the WHO’s Safe Motherhood framework, a key strategy for improving maternal and neonatal outcomes is to increase linkages between community-based providers and higher-level facility-based care.5 Importantly, in rural Guatemala, much prenatal care, births and early neonatal care are provided within the home by lay midwives.6 7 For example, in a recent national survey, only 50% of indigenous women gave birth within a healthcare facility.7
In most indigenous communities, lay midwives have limited formal education and Spanish-language fluency. Training is largely by apprenticeship to more experienced midwives. This is supplemented by monthly medical education sessions held within local government health posts. Attendance at these sessions is required in order to receive a license to practice. Other than these monthly education sessions, however, there is limited formal support—such as assistance with triage—from public health posts for midwives.8 9 Within this practice environment, mobile health (mHealth) technology may be able to improve the continuum of care, as it may provide midwives with decision support to assess complications and make referral decisions and to formalise their interactions with other health systems staff.10 11
Recently, working in collaboration with a group of indigenous Maya midwives affiliated with a primary healthcare organisation, Wuqu’ Kawoq | Maya Health Alliance, in a remote area of Guatemala, we conducted a randomised clinical trial of a package of mHealth perinatal tools, including smartphone-based symptom checklists, and remote phone-based and text-based medical back-up. We found that the mHealth package significantly improved the rate of facility-level prenatal and obstetrical care.12 As a result of this trial, the mHealth package was adopted as the standard of care at the collaborating primary care institution.
In this project, our goal was to use this existing practice network of lay midwives and mHealth platform to improve the quality of care for neonates. Several studies have demonstrated that lay midwives in various contexts can be trained to provide elements of neonatal care with improvements in outcomes, including early neonatal referrals.13–17 In addition, others have studied using mHealth to improve care for neonates in low resource settings. However, these studies have largely targeted higher-level health facility staff or patients themselves and have therefore not assessed the clinical impact of better integration of lay midwives.18–21
Measurement
Our primary quality improvement outcome was to increase the rate of referral of neonates born to participating midwives within the first week of life. Secondary outcomes were the proportion of neonates receiving a documented examination by participating midwives within the first week of life, the proportion of neonates identified as needing referral who completed the referral (rather than remaining at home) and neonatal death. Process outcomes monitored included volume of phone calls and text messages to the on-call medical team.
Given the limited clinical and demographic information collected by participating midwives as part of their routine workflow, community health workers bilingual in Spanish and Kaqchikel Maya performed home visits with new pregnant patients under midwife care as part of this improvement project. During these visits, they obtained signed informed consent for the use of individual-level data and collected demographic and prior obstetrical history, which was documented in each patient’s electronic health record (EHR). They also conducted a second visit, approximately 1–2 weeks after delivery, to collect additional information on neonatal health and any perinatal or postnatal complications. In addition, all calls by midwives to the on-call line, as well as the generation and clinical outcome of all neonatal referrals were documented in the EHR. A physician reviewed all the charts to confirm final outcomes and diagnosis, confirming these through conversation with the clinical staff at the receiving facilities when necessary. Call-backs to each midwife on a monthly basis by the nurse champion were used to verify the accuracy and completeness of birth records, which were all double-checked in the EHR. All data used in this project were subsequently extracted from the EHR. In particular, the monthly neonatal referral rate was calculated as the number of neonatal referrals in the EHR over the number of registered births.
Subsequently, data were extracted from the EHR using a structured query language. Descriptive statistics were generated using STATA V.14 (College Station, Texas, USA). Run charts and proportion control charts (P charts) were constructed using Minitab V.17 (State College, Pennsylvania, USA). For control charts, we used three calendar quarters of data preceding the intervention (January–September 2017) to construct the baseline. We used 3-sigma control limits and defined special cause as data points lying outside the control limits. The study was approved by the Institutional Review Boards of Maya Health Alliance (WK-2017-003) and Partners Healthcare (2017P000122). Individual patients gave signed, informed consent for the use of individual-level data.
Design
Design context
Maya Health Alliance is a primary care organisation working in five departments of Guatemala to provide healthcare to rural indigenous Maya communities. For more than a decade, Maya Health Alliance has worked closely with indigenous lay midwives, who are the primary providers of prenatal and obstetrical care for many communities. In 2015, Maya Health Alliance developed a smartphone application to provide enhanced decision support to collaborating midwives. The application—which has been described in detail elsewhere—includes image-guided and audio-guided checklists for prenatal, intrapartum, and postnatal encounters, the ability to collect automated blood pressure and fetal Doppler using peripheral devices, and SMS-based and voice-based support from an on-call medical team.22 The application has significantly increased the proportion of facility-level births from midwives’ communities and was adopted as a standard of care by Maya Health Alliance in 2017.12
This prior mHealth work and this current improvement project are part of a long-standing public–private collaboration between Maya Health Alliance, two health districts (Tecpán and Paquip, total catchment area ~150 000 population) and the regional referral hospital located in central Guatemalan province of Chimaltenango. The goal of this collaboration has been to provide additional private sector inputs to strengthen the integration of lay midwives into the health system and improve maternal–child health outcomes.
Improvement team and activities
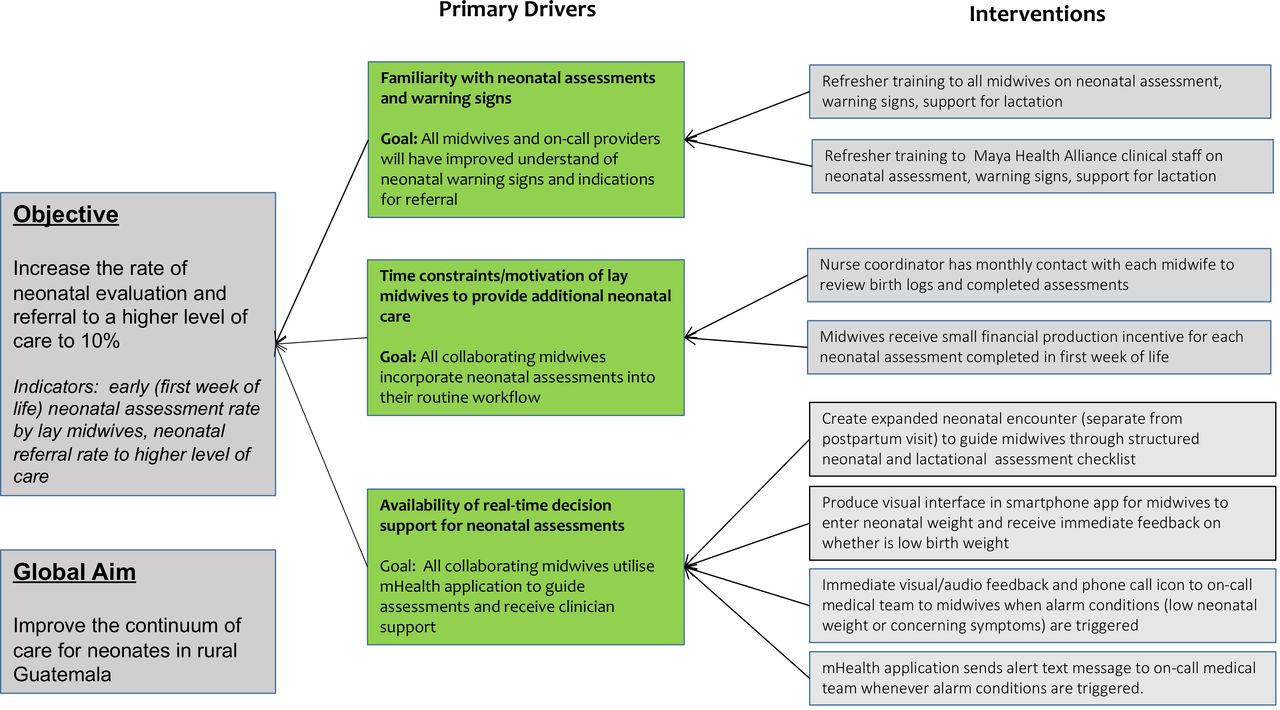
We formed a quality improvement team, which included a nurse champion (YJ), physician champion (MJ) at Maya Health Alliance as well as representative lay midwives and institutional leadership (PR). This team began by investigating the key drivers of neonatal care by midwives and related opportunities for improvement, as summarised above under ‘Problem’. Key areas were summarised using a key driver diagram and interventions to address each driver developed (figure 1).

Driver diagram for neonatal care continuum improvement initiative. Primary drivers and proposed interventions from the project planning phase are shown in relation to the key project objective.
After the start of improvement activities, the team met every 2 weeks to review performance data and evaluate and modify proposed interventions using a ‘Plan-Do-Study-Act’ methodology.23 The physician champion extracted clinical and process outcomes data from Maya Health Alliance’s EHR in advance of each meeting, presenting data in the form of run charts to assist with decision making and intervention evaluation.
To address the need for training in neonatal assessments and triage by midwives and back-up clinical staff, the improvement team reviewed Guatemala’s public health guidelines for primary care, as well as a review of the WHO’s Safe Childbirth Checklist and Essential Newborn Care Course.24–26 This content was distilled into short 1-day refresher courses for clinical staff.
In addition to improve standardised workflows for neonatal assessment by midwives—and to assist with improved decision support around classifying low birth weight—the improvement team proposed several changes to the existing mHealth interface in use by midwives (figure 1). This included a new structured symptom checklist for neonatal warning signs (online supplementary table 1, online supplementary figure 1) as well as a visual interface with automated decision support for entering birth weight (online supplementary figure 1). For these modifications, an agile design process was used whereby a small group of five midwives worked closely with our software engineers to iteratively alpha test changes to the interface.2 After initial design decisions were worked out, a larger group of 15 midwives began a beta test, using the modified interface in their clinical work, with additional feedback and modifications by the software team before implementation with the entire cohort. In the final application modifications, all user screens are pictogram-driven and do not require text entry. In addition, audio prompts in Kaqchikel Maya provide instructions to midwives on each screen (online supplementary figure 1). We have previously shown that these design features lead to applications with excellent usability characteristics, even for lay midwives with limited literacy and no prior exposure to smartphone technology.2 12
Supplemental material
Supplemental material
Implementation strategy
Our general strategy was to roll-out proposed improvement interventions from least to the most complex (table 1). We began with content refresher training on neonatal care, an intervention that was easy to implement in a timely manner while our development team worked on modifications to the mHealth platform. Similarly, performance incentives were delayed until mHealth modifications were complete, as we planned to use device visit logs to verify visit completion. Throughout the improvement initiative, midwives followed standard referral guidelines, referring neonates to local government health posts or to the regional referral hospital, as appropriate. The quality improvement team assisted by documenting all referral outcomes and providing feedback to both midwives and health personnel on neonatal outcomes.27
Timeline of interventions tested and other important events during the improvement intervention
PDSA cycle 1: training on neonatal assessment and warning signs
For this cycle, we focused on provide refresher training to providers on core neonatal warning signs and reasons for referral consolidated from national care guidelines and from the WHO’s Safe Childbirth Checklist and Essential Newborn Care Course (online supplementary table 1).24–26 From September to November 2017, separate 1-day training programmes were offered for participating lay midwives and for nurses and physicians providing back-up support for midwives, in order to allow for differences in learning style and content readiness. Both training programmes used an interactive, case-based approach to conduct a focused review of guidelines. The course for nurses and physicians was led by a senior physician on the improvement team. The course for midwives was led by a senior nurse at Maya Health Alliance's, who served as the nurse champion for this project.
PDSA cycle 2: implementation of neonatal warning signs checklist
As training sessions above were finishing, our engineering team (TN, CS and GC) had time to complete the development of a new neonatal warning signs checklist (online supplementary table 1), now presented as a separate, expanded workflow with the midwives’ mHealth interface separate from maternal workflows (online supplementary figure 1A). This checklist was developed by consensus in meetings of the entire implementation team. Subsequently, the physician champion coordinated work with the engineering team, whereas the nursing champion collected feedback on the interface design from midwives. From December 2017 to January of 2018, the cohort of participating midwives was trained in half-day sessions by the nurse champion in small groups on the use of this new workflow and, by the beginning of February 2018, all midwives had the new version of the mHealth application loaded on their phones.
PDSA cycle 3: refinement of triage criteria and production-based incentives
Based on our experiences when developing the original mHealth application, we anticipated a significant amount of over-referral with the new workflow through the mHealth application. During this cycle (February–March 2018), the physician champion reviewed medical chart data on each referral to determine the appropriateness of each triage decision. Subsequently, the nurse champion provided individual feedback based on this data to each midwife, focused on reinforcing appropriate referral decisions and discussing alternative management strategies for inappropriate referral decisions (eg, utilising ambulatory consultations at health posts rather than emergency referral mechanisms for minor complaints). To keep engagement and motivation high, small production-based incentives were introduced at this point for each neonatal assessment (~US$3/assessment), paid out monthly to midwives by the nursing champion during regular debriefing sessions.
PDSA cycle 4: improved detection of low birth weight and consolidation of technical support
In a final cycle (April–September 2018), the engineering team and physician champion introduced a final modification to the mHealth interface, a graphical input screen for registering neonatal birth weight (online supplementary figure 1B), with automatic alerts to the midwife for low birth weight cut-off points. Midwives were again trained on these changes to the interface by the project's nursing champion in small group half-day sessions. In addition, the nursing champion provided ongoing monthly individual feedback to each midwife on referrals generated, using data provided by the physician champion's chart review. By September 2018, after several months of process stability, data collection was scaled back, and the initiative was consolidated under the leadership of Maya Health Alliance’s midwife-nurse liaison (EC).
Results
Patient characteristics
From September 2017 to September 2018, affiliated midwives attended 869 births. Of these, 80 resulted in a neonatal referral to a higher level of care. Out of 869, 840 (97%) mothers gave informed consent for analysis of individual-level data, and these data are presented in the online supplementary table 2 (73 referrals). There were no statistically significant differences between neonates referred vs not referred by midwives to a higher level of care for any of the examined variables, except for birth weight. Overall neonatal mortality rate (before 28 days of life) was 7% in the referred cohort and 3% in the non-referred cohort, a difference that was not statistically significant.
Supplemental material
Using available individual-level data in the EHR, we determined the most common causes of pregnancy-related complications occurring for referred versus non-referred neonates. Important pregnancy-related complications, including hypertensive disorders, premature rupture of membranes, and threatened abortion occurred in both referred and non-referred neonates, but the total proportion as well as the distribution of different complications was not statistically different between the two groups (online supplementary table 3). We similarly determined the most common indications for midwife-initiated neonatal referral for the group of neonates who were referred. By far, the most common indication for referral was low birth weight, but other important indications included feeding difficulties, jaundice, respiratory distress and concern for sepsis (online supplementary table 3).
Supplemental material
Neonatal continuum of care and process outcomes
The primary improvement outcome was to increase the proportion of neonates evaluated by midwives and referred to a higher level of care for the evaluation of potential complications or warning signs. This improvement goal was supported by modifications to an existing mHealth interface to improve neonatal assessment and linkages to an on-call support team, training programmes on obtaining neonatal weight and physical assessment of neonates, and production-based incentives (figure 1, online supplementary table 1).
Lay midwives generated 111 phone calls involving 110 neonates (monthly median 9, IQR 3–11) to the on-call medical team to discuss management during the 12-month intervention, and they generated 80 successful referrals (monthly median 6, IQR 2–8) to a higher level of care. These were compared with monthly medians of 1.5 and 1 phone calls and successful neonatal referrals, respectively, during the preintervention period (online supplementary figure 2). Although training on neonatal assessments and pilot test of the optimised mHealth interface began with PDSA cycle 1 in September 2017 (online supplementary figure 2, arrows), increase in call and referral volume was only marked after general roll-out of the updated smartphone application to all midwives in the cohort in PDSA cycle 2 (online supplementary figure 2, arrows). Also notable is the decrement in calls and referrals in May 2018, when a software bug was inadvertently introduced into the application during routine maintenance, requiring debugging and application version roll-back.
Supplemental material
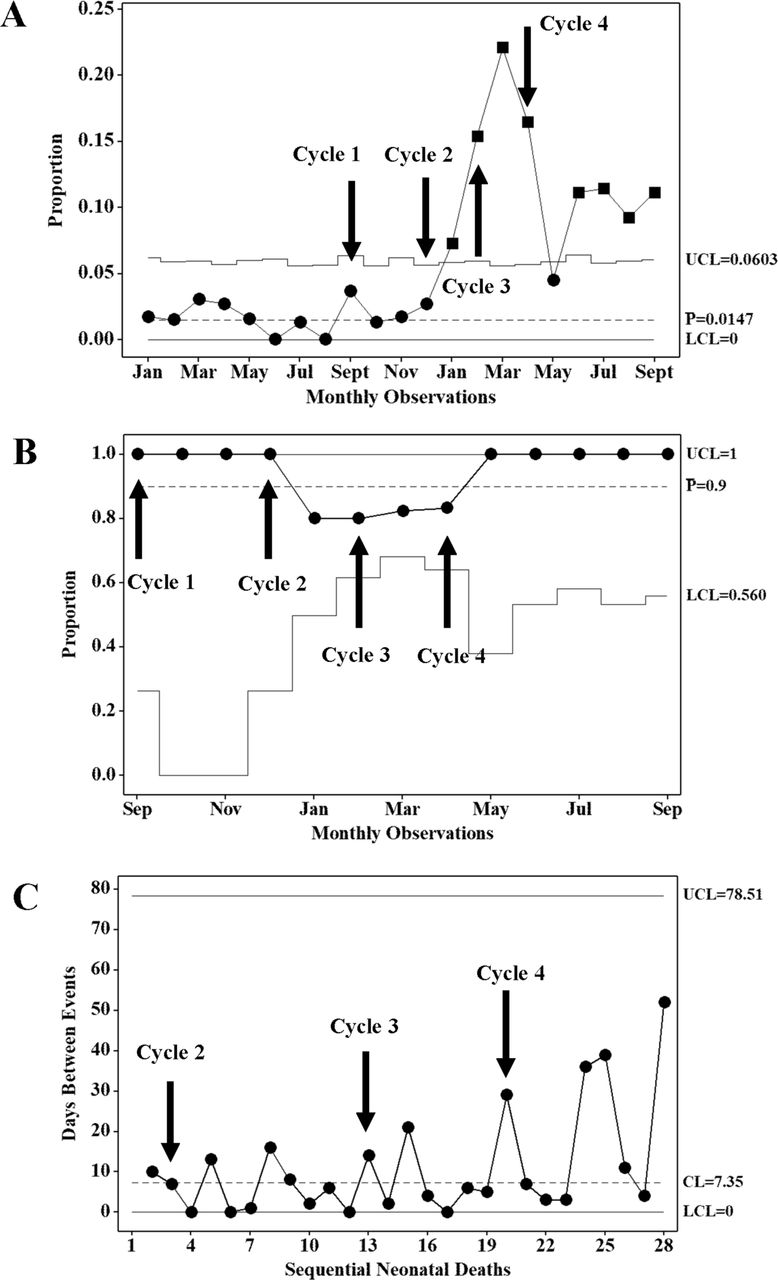
A proportion control chart was generated for the primary outcome of the proportion of all neonates in the cohort referred to a higher level of care (figure 2A). The mean preintervention proportion of neonatal referrals was low (monthly mean, 1.5%), increasing to a monthly mean of 9.9% in the intervention period. The special cause was obtained in January 2018 and sustained throughout the intervention period, with the exception of May 2018, when an application software bug was introduced inadvertently. In the first few months after the general roll-out of the updated smartphone application (PDSA cycles 2–3), the proportions of neonates referred were very high, exceeding 25% of all births in February 2018. In meetings of the QI team this was determined to be due to initial over-referral by midwives (eg, mild neonatal fussiness) and duplicated referrals (eg, several premature infants delivered to mothers with pre-eclampsia in the regional referral hospital were re-referred by midwives for low birth weight, after being safely discharged from the hospital). These issues were addressed through individual debriefings by project nurses with participating midwives in PDSA cycle 3.

{kind=link}
{kind=link}
Control charts of referral rate (A), successful referral completion (B) and days between neonatal deaths (C). UCL, LCL and baseline mean proportion ( ) or mean days between events (CL) are shown. Arrows indicate the timing of sequential PDSA cycles. Squares indicate the special cause. CL, control limit; LCL, lower control limit; UCL, upper control limit.
) or mean days between events (CL) are shown. Arrows indicate the timing of sequential PDSA cycles. Squares indicate the special cause. CL, control limit; LCL, lower control limit; UCL, upper control limit.
We also monitored key secondary outcomes. Beginning in September 2017, we tracked the proportion of neonatal referrals that were successfully completed (received indicated facility care) (figure 2B). Success remained high throughout the project, and it was lowest in the months when over-referral was temporarily a problem (as shown earlier). Beginning in February 2018, after the roll-out of the smartphone redesign to all midwives, we tracked the proportion of all neonates receiving a documented physical examination through the application. In February 2018, the proportion was 59%, subsequently rising to a monthly mean of 92% for the remainder of the intervention period (results not shown). For each neonatal visit completed in the first week of life, midwives were paid a production incentive of 25 Guatemalan quetzales (roughly US$3). Median monthly payout (IQR) per midwife over the course of the intervention was 275 (125–663) quetzales. Finally, we monitored neonatal deaths using a time-between-events chart (G chart). Toward the end of the improvement period, there seemed to be a trend toward an increase in the number of days between neonatal deaths (figure 2C), but this did not attain special cause.
Lessons and limitations
Rural indigenous communities in Guatemala have some of the worst neonatal outcomes in Latin America. Given the fact that many births in rural Guatemala occur in the home under the care of lay midwives, in this improvement project we sought to identify and overcome barriers to timely neonatal care by lay midwives in rural communities (figure 1). The improvement project occurred within a long-standing practice collaborative with lay midwives and an existing mHealth platform that could be modified relatively easily to introduce new workflows designed by the improvement team.
Specific interventions that we implemented included (a) training both midwives and on-call medical providers on neonatal assessment, warning signs and triage; (b) augmented decision support for neonatal assessments (and, especially, assessment of low birth weight) through an existing mHealth platform; and (c) financial production incentives for midwives conducting neonatal examinations. We found that this package of interventions effectively increased timely neonatal examinations by midwives and the proportion of neonates referred for evaluation at a higher level of care (figure 2A). The initiative seemed highly acceptable to participating communities, as the large majority of neonates identified as needing evaluation were successfully referred (figure 2B).
Our findings can be compared with others from the literature in Guatemala and elsewhere. For example, several studies have demonstrated that lay midwives can be trained to provide some elements of neonatal care with improvements in selected outcomes, including early neonatal referrals.13–17 A large multisite trial that included Guatemala trained lay midwives and other community-based providers on essential newborn care and neonatal resuscitation, it reduced stillbirth but not neonatal death rate and did not assess for changes in neonatal referral patterns.28 Another study in Guatemala provided similar training but added professional midwifery liaisons to advocate for improved perinatal referrals by lay midwives, but the impact on primary outcomes and referral patterns have not yet been reported.29 Finally, a recent metanalysis concluded that training for lay midwives and other frontline providers on essential newborn care and neonatal resuscitation can improve stillbirth and early neonatal mortality, but that gains after the first week of neonatal life require a more comprehensive continuum of care interventions.30
A strength of our improvement study, based on our key drivers analysis (figure 1) is that it addresses multiple steps along the neonatal care continuum, including not just training in neonatal assessment and triage by frontline providers (similar to the training offered in nearly every other neonatal intervention reviewed above), but also real-time mHealth and on-call support for assistance after the decision to refer was made. We used a mHealth design approach that included a close design collaboration with the midwife end users and produced an application usable even by those midwives with limited literacy or prior smartphone technology exposure.2 We also addressed the financial disincentives lay midwives face for taking on additional clinical work with neonates, which many may feel is outside their scope or interest. Multipronged continuum of care interventions like this is especially important in Guatemala where the extensive literature on obstetrical referrals has shown that the decision to refer is complex and often fear-laden, given the prevalence of disrespect and low-quality care that both lay midwives and their indigenous patients often experience within referral facilities.12 31–34
Our improvement study has several limitations. First, birth volume and in-home birth outcomes were self-reported by participating lay midwives. Although the improvement team was in close contact with each midwife, working to verify clinical volume and helping to adjudicate outcomes, the possibility remained for under-reporting both of overall births and, specifically, adverse outcomes. In addition, the overall observed neonatal mortality rate was high (7% among referred neonates, 3% among non-referred). It is possible that this rate may be artificially elevated, as deaths in the home were self-reported by midwives who may not have carefully distinguished between stillbirths and early neonatal deaths. At the same time, these rates do highlight the marked disparities in health outcomes in this rural population. For comparison, a large, representative population-based cohort study in rural Guatemala has also recently reported a 2%–3% mortality rate among neonates.3 35 Along these lines, although our time between rare events control chart showed a trend toward increased time between neonatal deaths, the sample of participating midwives and the birth cohort was small and therefore the data from our improvement project did not have the power to detect a change in mortality over the time course of the project.
Finally, this improvement intervention occurred within the context of a small, motivated group of practising midwives and a nonprofit primary care organisation providing technology support. Additional work will be needed to determine if similar improvement interventions can generalise other practices contexts in Guatemala where lay midwives provide care. As well, the financial sustainability of this and similar mHealth applications is an important area of ongoing exploration, if solutions like this are to be sustainable and scalable. Potential areas we are exploring now include (a) development of a ‘subscription model’ for smartphone applications with individual lay midwives as subscribers; (b) licensing of the application to institutional uses, such as large non-profits; (c) exploring subsidies by telecommunications providers in Guatemala.
Conclusions
In conclusion, an improvement intervention using traditional training sessions, mHealth decision support, on-call medical support and financial production incentives was successful at improving timely neonatal assessments and appropriate referrals to a higher level of medical care by a group of lay midwives working in rural indigenous communities in Guatemala. Our improvement approach, as well as the types of interventions used, may be of use to other rural global health settings where lay midwives are primary providers of neonatal care and where significant barriers to facility-level care exist.
Footnotes
Twitter @raxqij
Contributors MJ: coordinated and supervised the study, performed statistical analyses and drafted the initial manuscript. YJ and EC: coordinated and supervised the study and reviewed and revised the manuscript. TN and CS: programmed the app and provided support for data collection and engineering development. RH-C: provided design input to the mobile health technology and reviewed and revised the manuscript. GC: supervised the development of the mobile health technology and reviewed and revised the manuscript. PR: designed the study, performed statistical analyses, and reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding All phases of this study were funded by the Charles Hood Foundation.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository at: https://doi.org/10.7910/DVN/IXQ1BU