Article Text

Abstract
Background Trauma care represents a complex patient journey, requiring multidisciplinary coordinated care. Team members are human, and as such, how they feel about their colleagues and their work affects performance. The challenge for health service leaders is enabling culture that supports high levels of collaboration, co-operation and coordination across diverse groups. We aimed to define and improve relational aspects of trauma care at Gold Coast University Hospital.
Methods We conducted a mixed-methods collaborative ethnography using the relational coordination survey—an established tool to analyse the relational dimensions of multidisciplinary teamwork—participant observation, interviews and narrative surveys. Findings were presented to clinicians in working groups for further interpretation and to facilitate co-creation of targeted interventions designed to improve team relationships and performance.
Findings We engaged a complex multidisciplinary network of ~500 care providers dispersed across seven core interdependent clinical disciplines. Initial findings highlighted the importance of relationships in trauma care and opportunities to improve. Narrative survey and ethnographic findings further highlighted the centrality of a translational simulation programme in contributing positively to team culture and relational ties. A range of 16 interventions—focusing on structural, process and relational dimensions—were co-created with participants and are now being implemented and evaluated by various trauma care providers.
Conclusions Through engagement of clinicians spanning organisational boundaries, relational aspects of care can be measured and directly targeted in a collaborative quality improvement process. We encourage healthcare leaders to consider relationship-based quality improvement strategies, including translational simulation and relational coordination processes, in their efforts to improve care for patients with complex, interdependent journeys.
- qualitative research
- teamwork
- organizational theory
- resuscitation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The care of major trauma patients is complex and often time critical—the patterns of injury require assessment, investigation and treatment from multiple disciplines. Patients can suffer harm if care is poorly co-ordinated or if conflict arises in clinical decision-making.1 2 The trauma community has responded to this complexity with a variety of structural and process interventions—including the creation of trauma teams, explicit criteria for trauma team activation and pathways to guide clinical decision-making.1 3 4 Individuals and teams also train for their roles, focusing on task-specific knowledge, clinical skills and teamwork behaviours.3 5–7 However, care providers are human—and these teamwork behaviours are underpinned by their relationships with colleagues, and by institutional culture. Trauma care is an example of healthcare as a ‘complex socio-technical system’.2 With this reality in mind, quality improvement approaches that include focus on relational aspects of care have intuitive appeal.
Relational coordination (RC) theory describes factors that facilitate optimal work in high functioning organisations.8 The theory specifies three relational dimensions that support the coordination of work: shared goals transcend specific functional task-related goals, shared knowledge enables team members to understand how their tasks interrelate with others, and mutual respect allows members to overcome status barriers and positively regard the work of others. These relational dimensions are reinforced by communication that is timely, frequent, accurate and problem solving-based. RC is particularly critical in situations where teams are faced with high levels of task interdependence, uncertainty and time constraint. The theory has been applied in several healthcare contexts and offers an attractive lens for inquiry in this setting.9–12
Examining culture and relationships in complex trauma care is challenging. RC offers an appropriate framework for the task. RC can be measured within and between teams through a quantitative survey which produces a numerical RC index. However, other methods such as ethnography—an on the ground approach to evaluating culture—may be more appropriate to develop a nuanced understanding.8 13–15
Collaborative ethnography is a research approach which empowers participants in all stages including project conceptualisation, research design and analysis.16 17 Continuous commentary and evaluation are reintegrated back into the research process. A cyclical progression of collective fact finding and reflection evolves, leading to inquiry and action that is community desired and community driven.16–20 The research itself becomes a community building exercise.16–20 As such, collaborative ethnography seems a logical approach to embolden front-line care providers to share their stories, collectively reflect on their experiences and together drive progress.
We describe a unique collaborative ethnography that incorporated the RC framework. We aimed to understand and improve relational aspects of interdependent work in the setting of complex trauma care at Gold Coast University Hospital (GCUH).
Methods
Overview
Over a 3-month period, and with a constructivist stance, we engaged a community of trauma care providers in a mixed-methods collaborative ethnography.16 17 The ethnography included narrative surveys, participant observation, interviews and a quantitative measure of RC. Data gathered during the initial phase was shared with participants and informed interpretation and the collaborative development of interventions which are now in various stages of participant-led implementation and evaluation.
Context
GCUH is a large tertiary care hospital and major trauma centre in Australia. Over 400 staff from a variety of disciplines participate in the early stages of care for major trauma patients. In the financial year 2017/2018, there were 1739 trauma team activations, including 203 ‘Trauma Responds’, which is the highest level of acuity. There are key identifiable groups involved in the early phases (within the first hour) of major trauma care and their inter-relationships for the initial phases of major trauma patient care are represented in figure 1. Each group is represented by function and/or geographical location, rather than a professional discipline.

Web of core providers involved in trauma care. ED, emergency department; ICU, intensive care unit; Pre-hosp, high acuity response unit paramedics.
For the past five years, members from each of these groups have participated monthly in an in situ trauma respond simulation exercise including a case and debrief. The focus of these exercises is ‘translational’—including exploration of system strengths and weaknesses, and practising targeted interventions to improve.21 Prior to this project, independent groups (the trauma service and emergency medicine) had at various times identified trauma-related quality improvement goals, mainly related to care processes or systems. There was limited formal recognition of the role of relationships between or within multidisciplinary work groups contributing to the quality improvement agenda in trauma care.
Core project team and initial consultation
The research team was composed of EIP who is master’s student in applied anthropology and an emergency medicine trainee; DM who is a project lead at the Centre for Health Innovation at GCUH; CA a junior doctor who has worked across disciplines for the trauma service, surgical service and emergency department; VB who is a senior emergency physician and trauma team leader; and DH who is an anthropologist at the University of North Texas. As the first step in the collaborative ethnography process, leaders from each of the main disciplines, outlined in figure 1, were consulted via email and group meetings for question and project design and formed the core project team. Many coauthor this paper. This team decided understanding and improving relationships between trauma care providers was of interest and importance as a potential path towards improving patient care. They also had specific interest in understanding the role of monthly trauma simulations. The aforementioned research team offered logistical and methodological support for those goals. At research and core project team meetings, we collectively reflected on our positioning and how our perspectives may have affected results.
Data collection
The core project team distributed a survey (online appendix A) with three distinct parts: RC survey, narrative experience with trauma care and experience with in situ simulation. The RC questions assessed the strength of communication and relationship ties between participating work groups. Participants were asked to rate their perception of communication and relationship behaviours between their own work group and the other work groups along the seven dimensions of RC. The RC survey is a tool that has met psychometric validation standards across multiple populations and is suitable for use by unbounded teams in the healthcare setting.22 23 Four narrative questions related to experience with trauma care provision and five questions related to experience with in situ simulation followed the RC survey. These questions were piloted and refined with representatives from each group. The survey was distributed via an individual unique online survey link to each care provider in every working group depicted in figure 2.
{kind=link}
{kind=link}
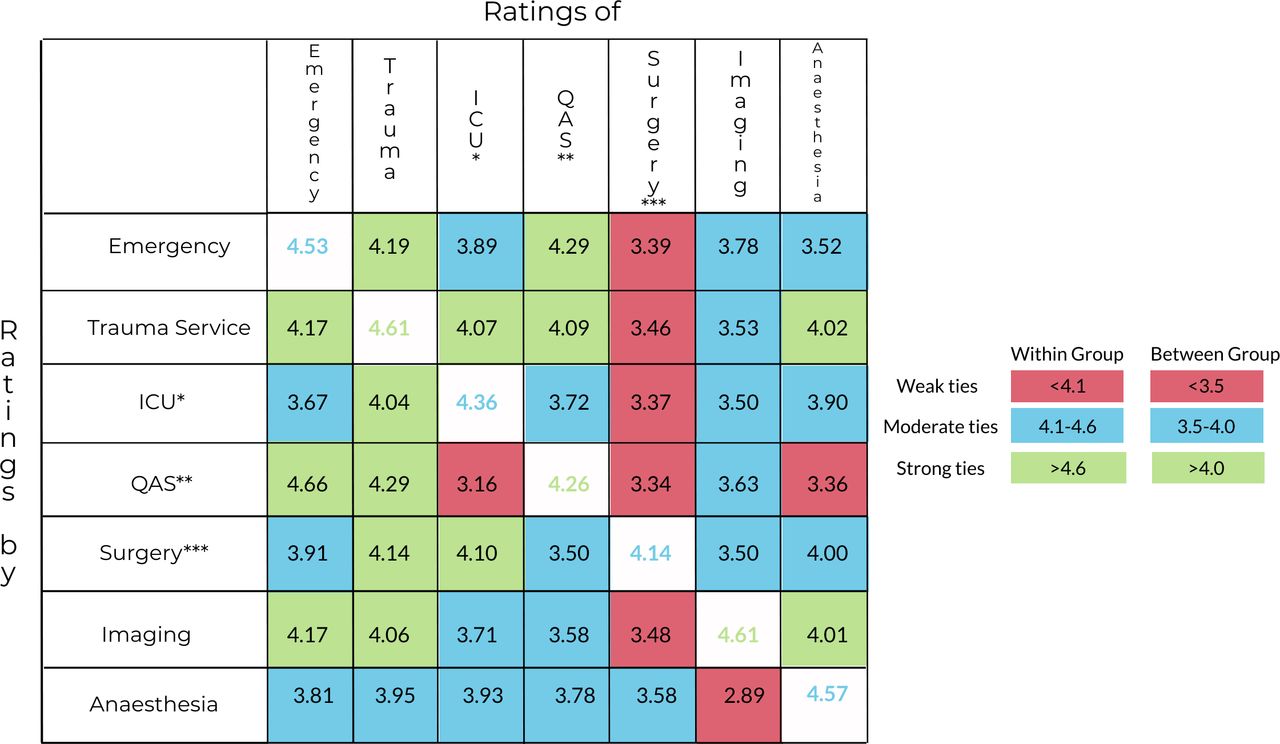
Relational coordination ties between groups involved in early trauma care. The relational coordination matrix shows how each workgroup rates the others (horizontal) and how it is rated by the others (vertical). The diagonal shows how each group rates itself. Comparing above and below the diagonal, you can see how the same relationship is rated by each of the two workgroups involved. *ICU, Intensive care unit; **QAS, queensland ambulance service high acuity response unit; ***Surgery, general surgery.
To further contextualise the survey results, over a 3-month period EIP conducted participant observation, informal interviews and formal interviews. This included approximately 75 hours of participant observation of randomly selected traumas, consecutive educational activities and daily activities of individual trauma providers identified through key informants. She engaged in an additional 25 hours of informal interviewing of trauma providers across these contexts. This activity informed field notes. Five formal interviews were performed with key personnel to further explore issues raised in the survey or through observation. These interviews were recorded and transcribed by EIP. Participant observation and interviewing stopped when saturation of RC themes occurred, and no new themes were identified as determined by EIP, CA and VB.
Data analysis
Quantitative RC data were analysed by the RC analytics team according to procedures detailed by the instrument’s developer.24 RC indices were constructed at the individual participant level across the seven dimensions of RC then aggregated to the group level to provide an overall RC index and a numeric indicator of the strength of each relational interface in each dimension between and within each working group. Cut points for strength of ties (weak, moderate and strong) between and within groups are based on norms from established data and were used to present data in a tangible way to facilitate the reflective process.24
Qualitative data from narrative surveys, participant observation, informal interviews and interviews were input into NVivo and analysed using a recursive approach. Data were anonymised then coded by EIP and CA using the RC framework (shared goals, shared knowledge, mutual respect and four domains of communication) as initial themes. Further themes were identified and agreed on by EIP and CA which then became additional focus of observation as the ethnographic process evolved. Ethnography, used this way, as a tool to gain both deductive and inductive insights has been previously described.14
The raw data, in full in addition to the analysis, were presented to the research team and core project team for member checking of analysis and for identification of any further themes.
Broad participant ethnography and working groups
The data, both qualitative and quantitative, from the ethnography were not designed to be evaluative, rather they served primarily as a as a launch point for collective reflection, discussion and the design of collaborative interventions with a broader group of participants. At two points, findings were shared with all trauma care providers through written communiques (online appendixes B and C). All were invited to smaller in-person group meetings where the findings were discussed in detail and open to further interpretation. At those meetings, VB facilitated a discussion that sought participants’ perspectives on potential interventions to improve trauma care based on the initial findings.
Intervention development and implementation
The potential interventions suggested during participant working groups were brought back to the team of core leaders in each of the clinical areas for prioritisation. Champions for each intervention, not necessarily core project team members, were identified. Support of the research team and simulation service were available for those designing, instituting and evaluating specific projects. The implementation and evaluation of these individual projects is ongoing.
Patient and public involvement
Patients and the public were not involved in the design or presentation of this work.
Findings
Baseline relationships within the trauma service
The overall picture from the quantitative RC data and qualitative ethnography was that of strong interdepartmental relationships with opportunities and enthusiasm for progress. In addition, 180/482 (37%) individuals across all care groups completed the survey, but notably we had challenges reaching the general surgeons with a response rate from that cohort of only 12% which was much lower than all other groups (ED 43%, Trauma 93%, ICU 35%, Queensland Ambulance Service (QAS) 100%, Imaging 29%, Anaesthetics 24%). The RC ‘Team Score’ was 3.80 which is an aggregate score across all domains and signals moderate ties between all groups. These data were further broken down into ties between and within individual groups, as depicted in figure 2. Of particular note are the strong relational ties of trauma service as rated by other groups and the weaker with the surgical service as rated by all other groups, except anaesthetics.
Qualitative aspects of the ethnography provided considerable insight into the relational foundations of trauma work at GCUH. Each domain of RC was relevant to trauma care. Table 1 shares participant insights from survey responses about each domain of RC that were either in practice when care was perceived to have gone well or were lacking in moments when the team felt they could be working better. Based on initial survey responses, two additional themes (the ‘team briefing’ and ‘involvement of senior decision makers’) were initially identified by EIP and CA to be particularly relevant. Though, on deeper probing in informal interviews and observation, the effect of these two themes could be accounted for by the RC framework. The theme of ‘team briefing’ featured prominently in responses about trauma activations that were perceived to have gone well by providers. For example, one survey participant responded:
Relational coordination (RC) framework applied to narrative survey data
“[traumas go well when] we are notified in advance, roles[are] allocated prior topatientarrival, [we have] discussed likely issues with thepatientand how we would manage them and the likely sequence of events prior topatient’s arrival”.
Yet participant observation revealed significant variability between individual trauma team leaders as to whether and how the team briefing was performed. Further informal interviews and observation facilitated the understanding that effective team briefing can scaffold each domain of RC at the beginning of a given case for the specific care team involved—setting up shared knowledge (about each team member’s role and about the patient’s condition), shared goals (by outlining initial, and contingency, priorities for patient management), mutual respect (by learning names and thanking everyone for attending), and setting the stage for timely and problem solving–based communication (by asking for input from others attending).
The involvement of senior decision-makers was most relevant in moments when definitive management or disposition of a patient relied on input from surgical specialties. Occasionally, this occurred with critically ill patients (ie, decision to go to the operating theatre immediately) but more often it related to the multi-injured patient who did not require immediate intervention but still necessitated management and disposition plans from consulting services. One participant wrote:
“Trauma activations at night do not go as well, without senior decision makers present. The surgical registrars often disappear without communicating management plans (probably because they don’t know the plans). It takes an awful lot longer to come to a management plan about a patient's disposition (OT or no OT) at night”.
Further informal interviews and observation elucidated that the critical features associated with ‘involvement of senior decision makers’ were most related to the ability to engage in problem solving–based communication and the timeliness of communication as it related to patient management plan and disposition.
Role of simulation in strengthening RC
The trauma service co-ordinates monthly simulation exercises. These simulations are conducted involving providers from across the care continuum—paramedics, emergency department staff, medical imaging, operating theatre staff, surgery teams and intensive care teams, as well as support services such as blood bank, orderlies and security. Staff participate in simulations as part of their education, and as a standard part of trauma service delivery improvement. The survey responses and associated participant observation of simulation exercises revealed an impact that included but went beyond the specific medical nuances of individual cases or improvement in trauma processes. Simulation directly targeted the development of all domains of RC (table 2). Most noticeably, simulations seemed to foster mutual respect between specialties, with one survey participant representatively noting,
Simulation and relational coordination domains*
“Relationships have definitely strengthened over the time we’ve been doing monthly Trauma Sim. The conversations in the back room enhance the conversations in the Resus room”.
Further analysis of simulation-specific data is available in Brazil et al.2525
Intervention development and implementation
Data from the initial phase were communicated to all trauma care providers through a communique (online appendix B) and open working meetings with each group were held to reflect on and build from the findings. In total, we held seven 1-hour working groups with 69 health professionals over a 1-month period. No formal working group meeting was held with the high acuity response paramedic group as this was a small cohort external to the hospital, with whom we sought input via email, informal and formal interviews, and through paramedic author GB’s direct communication with his colleagues. We were unable to arrange a meeting with the surgical group. Input was sought via alternate means including email, and informal and formal interviews with surgical residents. From these working groups, potential interventions were brought to the core leadership for prioritisation and implementation planning.
Table 3 shows 16 interventions co-created with participants, and prioritised by the leadership team, for implementation as they relate to specific organisational interfaces. Some interventions were structurally rooted (ie, video feed from resuscitation room to theatre) while others were more process focused (ie, team briefing rehearsals). All interventions also included a relational component. Relationships featured either directly (ie, peer feedback for trauma team leaders) or more often indirectly, as the design and development naturally brought people together from across organisational interfaces (ie, collaboration between anaesthetics and paramedics to improve handover of critically bleeding patients in the operating theatre). The implementation of these 16 interventions are in varying stages from planned to completed and their impact is being monitored through a variety of scholarly projects, many headed by the participants themselves rather than the core project team. For example, a mixed group of CT radiographers, radiology registrars, emergency registrars, nurses and orderlies are implementing and evaluating a project designed to improve transfer to and from the CT Scanner ‘fast and safe’, while an emergency medicine fellow and nurse have collaborated to implement and evaluate ‘OneTeam Practice’, a daily mental rehearsal of team briefings.
Collaboratively developed interventions
Discussion
We report a unique, relationship-based approach to quality improvement in management of severe trauma. Using a collaborative ethnography that included RC analytics, participant observation, narrative surveys, interviews and working groups we effectively engaged front-line care providers in a reflective process and the design and implementation of interventions targeted at improving the relational foundations of trauma care delivery at a large tertiary care trauma centre.
RC in trauma
While RC theory has been used in healthcare settings such as postsurgical wards, inpatient wards, and outpatient clinics, to our knowledge, we are the first group to apply the concept to a hyperacute resuscitation environment of severe trauma.9 10 12 We decided to simultaneously collect qualitative data, in addition to the RC metrics, to build further understanding about this construct in the setting of trauma. As outlined in table 1, its domains accounted for many of the factors identified in resuscitations that went well and were perceptibly missing from those cases that were felt to be less than ideal. Of note, the centrality of team briefings to trauma care is in keeping with the findings from other studies that suggest cross-functional meetings, with broad participation, are a mechanism to promote RC.12 26 We found RC to be a useful framework in the acute trauma environment and hypothesise it can likely be applied more broadly in other resuscitation contexts.
Application of the RC framework to qualitative data, exposed fundamental areas of success and tension within a complex and dynamic working environment. These data, in combination with the quantitative RC analytics, served as a powerful launch point for facilitating engagement of a web of trauma care providers in meaningful, collective reflection about the work that we do and how we might do it better. With ongoing support from the research team, trauma care providers are now the ones driving the design, implementation and evaluation of a series of interventions that span organisational boundaries. Beyond the independent effect of any one specific product that results from a collaborative ethnography, the design and conduct of project itself often influences communities and culture.16 17 This was consistent with our experience. At one particular research meeting, we reflected that working on the study seemed to bolster RC within the core project team in ways that individuals found affected their clinical work too. By bringing people to the same table, sharing narratives related to experiences and collectively creating a path forward, we hope that the project itself fostered the development of shared goals, shared knowledge and mutual respect in a way that spanned hierarchies and crossed professional interfaces within our organisation.
Collaboratively developed interventions
There was wide variation in the nature of the specific interventions suggested. The diversity in outputs is evidence of the multifaceted ways in which trauma care providers experience relationships in the context of their work and how they perceive they can shape them. Simulation, team briefings, trauma stand downs, codes of conduct and feedback mechanisms are not new concepts in trauma care, but trauma providers’ desire to channel energy in these directions in an effort to improve relationships adds to our understanding of why these specific interventions are important and effective. We were particularly intrigued that nearly half of the proposed interventions included some form of simulation. Although it is becoming a more popular tool in quality improvement, simulation’s ability to shape relationships and culture in work environments has not been well studied. These and other reflection on translational simulation by our participants strongly suggest that a thoughtfully designed programme can directly target each domain of RC, with particularly impressive implications for the development of mutual respect between groups.25 The potential for simulation to shape culture is in keeping with previous research in the medical school context.27 We recognise that participants’ previous positive experiences with simulation at our institution and the presence of simulation educators on the core project team may account for why it features so prominently in proposed interventions at our site.
As noted throughout the findings, we had difficulty engaging general surgery colleagues which we see as a critically important result itself. The reasons are multifactorial, and require ongoing reflection and investigation. One contributing factor is likely related to the strong presence and portfolio of two trauma service surgeons during daytime hours which could limit trauma involvement of other general surgeons and registrars who provide after-hours coverage only. Our ethnographic data showed that it is during times when the trauma service is not available that the timeliness of communication and the ability to engage in problem solving–based communication with general surgeons is most threatened. As such, deliberately fostering RC with this group remains a particularly high priority. A number of the interventions directly aim to improve the co-ordination of decision-making without any significant investment from surgical teams. These include exercises directed at improving team briefings and the implementation of trauma stand downs. But perhaps more importantly, directed efforts to further understand surgical priorities and perspectives are underway. These efforts, proposed by anaesthetists (who have the strongest relational ties with surgeons) and surgeons themselves, include damage control resuscitation surgical simulations and a similar study of RC of teams involved in the trauma patient’s journey once in the operating theatre. Both of these programmes are designed to include continued overlap with trauma care providers from multiple other disciplines but in a different, perhaps more meaningful, setting for surgeons. We are optimistic these endeavours might facilitate further understanding and simultaneously impact RC between groups.
Investing in the interventions designed by a community that was informed by qualitative and quantitative RC data is a positive step towards fostering employee functional relationships in a systematic way and that goes well beyond encouraging collegiality—a worthy goal in the pursuit of organisational excellence.26
Limitations
The findings we describe and the interventions our participants developed reflect our own organisational milieu and also reflect experiences of individuals motivated to engage in the process. Readers may be able to draw parallels to their experience but we encourage focus on our methods, not our specific results. The outcomes and interventions should be unique to every group that this process is applied to, that is in fact the goal.
There are additional players involved in trauma care that were not included in this initial study but whom we recognise the importance of engaging with moving forward such as environmental services personnel, social work, subspecialty surgeons and interventional radiologists.
This was a grassroots study that used minimal resources and incurred minimal cost. Throughout the course of the project, we received suggestions for proposed interventions, such as providing 24-hour trauma service coverage, that would be likely to improve RC significantly but that were unfortunately far outside the scope of what we could offer. We were not positioned to make significant structural changes. Data related to these larger systems-based suggestions were shared with institutional leadership. Since doing so, trauma service hours have been extended to include Saturday and Sunday daytime hours. We do not know if this decision was a direct result of our study findings, but the narratives and data did provide additional urgency, context and impetus for the structural change even if we were not powered to provide it directly.
Finally, collaborative ethnographies are deliberately designed so that those driving the research are also members of the community being studied. This is one of the greatest strengths of our work but also a necessary point of reflection. Throughout the conduct of this project, it was impossible—and not the intention—for our authorship team to divorce themselves from their personal experiences within the organisation. The make-up of the research team may have also affected engagement of other study participants. Though pure objectivity was not the goal, to protect against overwhelming individual biases, we created a diverse project team with voices from each of the different groups involved. Furthermore, data analysis was overseen by EIP, an anthropologist and partial outsider, DH an external anthropologist and DM who is not involved in trauma care. Finally, results were member checked with those in the organisation and felt to be in keeping with broader experience.
Future action
Building on the work of Blakeney et al, at 1 year out we plan to remeasure RC.12 At that time, we will also compare relevant trauma-specific clinical indices. We see these as secondary outcomes to the benefits the process of undertaking a collaborative ethnography has offered our community in terms of reflective practice across boundaries and empowerment of providers to consider how they might do their work better, together.
Stemming from our work are a number of projects evaluating specific interventions. These studies are largely led by participants turned collaborators. Future research will explore the application of RC theory to other high acuity patient presentations such as deteriorating patients on hospital wards or teams involved in obstetrical emergencies. Further detailed understanding of the specific features of translational simulation that foster the development of RC would be beneficial for simulation educators who are interested in relational and organisational culture outcomes.
Conclusions
Through collaborative engagement of clinicians spanning organisational boundaries, relational aspects of care can be measured and directly targeted in a collective quality improvement process. We encourage healthcare leaders to consider relationship-based quality improvement strategies, including translational simulation and RC processes, in their efforts to improve care for patients with complex, interdependent journeys.
Supplemental material
Supplemental material
Supplemental material
References
Footnotes
Twitter @purdy_eve
Presented at Gold Coast Hospital Research Day, Queensland Trauma Symposium.
Contributors EIP was involved in project design, participant observation, informal interviews, interviews, focus groups, survey design, data analysis and initial draft of the manuscript. DM was involved in project design, survey design, data management and analysis, and review of the manuscript. CA was involved with data management and analysis and critical review of the manuscript. MS was involved with project design, survey distribution, data analysis and critical review of the manuscript. AD was involved with project design, survey distribution, data analysis and critical review of the manuscript. DC was involved with project design, survey distribution, data analysis and critical review of the manuscript. MW was involved with project design, survey distribution, data analysis and critical review of the manuscript. GB was involved with project design, survey distribution, data analysis and critical review of the manuscript. DH was involved with project design, data analysis, drafting of the manuscript and critical review of the manuscript. VB was involved with project design, distribution of surveys, data analysis, drafting the manuscript and critical review of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the GCUH Human Ethics Research Committee (HREC/18/QGC/13).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available. Data are not available in total as some of them are identifiable. Quantitative data and de-identified qualitative data are available on request (epurdy@qmed.ca).