Article Text

Abstract
Introduction A urinary catheter constitutes a one-point patient restraint, can induce deconditioning and may lead to patient mortality. An audit performed at Winchester District Memorial Hospital revealed that 20% of patients had a urinary catheter, of whom 31% did not meet the criteria for catheterisation. The main objective of this study was to use the Influencer Change Model and the Choosing Wisely Canada toolkit to create a bundle of interventions that would reduce the unnecessary use of urinary catheters in hospitalised patients.
Methods In a rural teaching hospital, a time-series quasi-experiment was employed to decrease inappropriate use of urinary catheters. Both the Choosing Wisely Canada toolkit for appropriate use of urinary catheters and the Influencer change management approach were used to create effective interventions.
Results This study revealed that there was no improvement in appropriate urinary catheter use during Plan-Do-Study-Act (PDSA) cycle 1. There was gradual improvement during PDSA cycle 2, with the percentage of inappropriate urinary catheter use dropping from an initial 31% before any interventions to less than 5% by the end of this study.
Discussion/conclusion This study aimed to reduce the inappropriate use of urinary catheters in a rural hospital with limited resources. The findings indicate that by using a change model, such as the Influencer Change Model, it is possible to promote better patient care through empowering healthcare staff to implement accepted protocols more stringently and thereby to decrease the inappropriate use of urinary catheters to 0%.
- unnecessary procedures
- quality improvement
- hospital medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Indwelling urinary catheters are commonly used during hospitalisation and may be beneficial in patients with conditions such as limited mobility, risk of falls, bladder outlet obstruction or a spinal cord injury.1 However, a urinary catheter comes with several risks, including trauma, skin breakdown and urethral strictures.2 Urinary catheters also increase the risk of urinary tract infection to 3%–7% per day.1 Likewise, healthcare-associated deconditioning is a major concern.3 Studies have shown that placement of a catheter prolongs hospitalisation, increases mortality and leads to additional costs for treatment of post-indwelling urinary catheter complications.2 4–6
The overuse of urinary catheters has been a growing concern in the USA and Canadian healthcare systems.7 It is estimated that 15%–25% of patients will have a urinary catheter placed during their hospitalisation.8 The US Centers for Disease Control and Prevention (CDC) published guidelines on the use of urinary catheters in 2009, clearly defining appropriate and inappropriate urinary catheter use.9 The Association for Professionals in Infection Control also set up guidelines for the use of urinary catheters in 200910 which was then revised in 2014.1 In Canada, the Saskatchewan Ministry of Health created guidelines in 2013 outlining proper urinary catheterisation for patients in long-term care settings.11 These guidelines serve as a framework that hospitals can use to develop protocols and prevent unnecessary complications due to inappropriate urinary catheterisation. However, greater effort is still needed to enforce these guidelines.12 13
Urinary catheters are sometimes placed inappropriately in patients without meeting the suggested criteria. Similarly, their removal is often forgotten when the indication is no longer present.14 In the USA, Medicare and Medicaid ceased to reimburse catheter-associated urinary tract infections that occur during hospitalisation in 2008, categorising them under preventable events. In addition, several studies have shown that medical directives for removal of urinary catheters and awareness of their proper use by healthcare staff can lead to significant improvement in patient care.15
A preliminary audit was performed at Winchester District Memorial Hospital (WDMH) to measure the level of appropriate urinary catheter use. Baseline measurement of urinary catheter use among inpatient medical–surgical care patient populations was sought through an internal prospective evaluation that constituted of collecting data during multidisciplinary rounds, conducting a shared assessment with the patient-designated nurse, and chart audit. The baseline internal evaluation was led by a staff registered practical nurse as part of ‘Late Career’ Initiative, sponsored by government of Ontario. The baseline audit revealed that over a period of 2 months, an average of 31% and 41% of the catheterised patients did not meet the CDC criteria.9 Moreover at any given point of time, an average of 20% of the inpatient population had a urinary catheter inserted. This falls at the high end of range identified by Darbyshire et al in 2016.16
The Choosing Wisely Canada toolkit was used to guide these improvements and implementation of a new guideline with the goal of reducing inappropriate urinary catheter use.17 Choosing Wisely Canada provides simple tools, resources and lists of recommendations supported by evidence to enable healthcare providers and organisations to put recommendations into practice. The toolkit provided by Choosing Wisely Canada was created in 2017 to improve appropriate urinary catheter use at Sunnybrook Health Sciences Centre in Toronto, Canada. The toolkit used the CDC guidelines as a basis to create its own consensus criteria for urinary catheterisation. It implemented a medical directive that allowed nurses to remove urinary catheters when they were not required as well as to manage urinary retention post-catheter use. The toolkit also emphasised training/educating healthcare personnel on proper urinary catheter use. This along with the behavioural change strategy, The Influencer Change Model, was used to create a bundle of interventions designed to create sustainable change in the culture and practice at WDMH in regard to appropriate catheter use.18
The main objective of this study was to examine the use of the Influencer Change Model and the Choosing Wisely Canada toolkit to create a bundle of interventions that would effectively reduce the unnecessary use of urinary catheters in hospitalised patients.
Methods
Research question
Would effective use of the Influencer Model of Change and the Choosing Wisely Toolkit help correct the inappropriate urinary catheterisation use among patients in the acute medical–surgical care unit?
Context
WDMH is a 53-bed community hospital located in rural Winchester, Ontario. WDMH serves a population of about 37 000 in an area of 1500 km2. It is a teaching hospital and directs the Centre of Excellence for Rural Health and Education. The hospital has an emergency department, childbirth centre, continuing complex care unit (CCCU), surgical operating rooms and inpatient wards. It admits an average of 128 patients a month into its acute medical–surgical care unit and complex continuous care unit. The medical–surgical and CCCU units agreed to participate in this study. These inpatient units contain a total of 37 beds.
Behavioural change strategy
The Influencer Change Model, developed by Grenny et al, was used to change the prior behaviour around catheterisation observed at WDMH.18 The study team agreed on an action plan consisting of a bundle of interventions and strategies, outlined below, which leverage the maximum number of sources of influences that the Influencer Change Model suggests18 (table 1). They ranged from low-leverage interventions such as awareness campaigns to high-leverage interventions such as medical directives. Since the behaviour we are trying to change is not only a result of lack of knowledge, education alone was not enough to induce a significant change. Our ultimate goal was to ensure that every staff member is capable of doing what is required and is motivated to do so.
The influencer change model
Interventions
The quality improvement project was designed to test appropriateness of catheterisation during three phases: pre-intervention, Plan-Do-Study-Act (PDSA) cycle 1 and PDSA cycle 2. Initially, in the pre-intervention phase data were collected for 2 months on appropriate urinary catheter use to measure baseline levels. The intervention then occurred over a 12-month period until stable improvement was observed. There were two PDSA cycles of interventions (table 2).
Overview of the intervention period and its stages
PDSA 1 (months 1–6)
The team used two forces of influence by boosting personal and structural abilities. First, they involved staff and stakeholders in discussions around a list of appropriate catheterisation criteria to reach consensus, using the Choosing Wisely Canada Toolkit as an implementation guide.17
List of consensus criteria requiring urinary catheterisation
Acute urinary obstruction.
Perioperative use in selected surgeries.
Assistance with healing of stage III or IV sacral wounds in incontinent patients.
Comfort for end of life patients
Required immobilisation for trauma or surgery patients
Established permanent indwelling catheter
Continuous bladder irrigation for gross haematuria.
Enhanced Care Unit (ECU) only: Accurate measurement of urinary output in critically ill patients (eg, q1hr).
The list became part of a Catheter Assessment Tool, which was used while auditing (online supplementary appendix A). The team also adapted an algorithm for assessing and removing urinary catheter (online supplementary appendix B) that was created and published by Leis et al in 201615 and found in the Choosing Wisely toolkit.17 The creation of WDMH appropriate list of catheterisation criteria and catheter removal algorithms resulted in alignment among different clinical staff and produced a necessary structural enabler.
Supplemental material
Supplemental material
Since the key to personal ability is to invest in skill building, we provided nurses and doctors with the necessary knowledge to ensure that they know exactly when it is appropriate and inappropriate to insert a urinary catheter and how to carefully and systematically monitor a urinary catheter removal. Nurses and doctors were given multiple rounds of education on the importance of proper urinary catheter use and the new catheter removal algorithm. Education was given face-to-face and through Surge Learning, a Canadian-based online education company brand that WDMH uses to deliver and track education. In addition to motivating nurses to avoid inserting or removing unnecessary catheters, the programme showed them how they can appropriately do so with an appropriate monitoring plan in place and without putting patient at risk.
Additionally, the team created and placed reminder stickers on urinary catheter collection bags in the stock room. They contained the appropriate catheterisation criterion and were supposed to work as visual reminder for nurses whenever they grab a new urinary catheter bag (online supplementary appendix C).
Supplemental material
During PDSA 2 (months 7–12)
Additional strategies were implemented to leverage an extra four sources of influence: personal motivation, social motivation, social abilities and structural motivation.
Personal motivation
Personal motivation was necessary to enable the team to overcome the discomfort associated with changing an old, familiar routine to a new, unfamiliar one. To achieve this goal, the team showed clinical staff the positive outcome data associated with catheter removal, allowing nurses and physicians to better understand how removing a catheter contributed positively to patient functional status. We also shared meaningful stories about how some patients feel when having a urinary catheter and how it results in decreased mobility leading to deconditioning, sometime irreversible. This was delivered during team huddles and through presentation of educational slides. Harnessing peer pressure during the PDSA-2 was critical for the behavioural reform, as social influences usually support the status quo and discourage adapting the new behaviour.
Social motivation and abilities
Social motivation and abilities were accomplished by employing clinical champions to get peer pressure working for quality improvement. The champion’s role was to educate providers, provide 2 min reminders in the ward team huddles, answer questions from staff, identify implementation barriers and provide social approval for the change. We believed that the frequent interactions between staff and their peer champions would shape and sustain the newly adapted practice. The team identified a primary nurse champion with interest and strong belief in the project and provided her with extra training by the stewardship team to ensure that she could answer any possible questions from staff. She was also advised to identify two extra secondary champions to maximise the chance of having a champion present during any given shift at the medical–surgical care ward. Champions played a significant role in motivating staff to use urinary catheter algorithms and criteria appropriately and provided an extra hand if the bladder scanner needed to be brought from another floor. The chief of family medicine was a key member of the team and acted as a champion for physicians. Champions’ involvement in delivering education fortified its efficiency and boosted the personal abilities of participants.
Structural motivation
Structural motivation was attained via recognition of champions’ effort by management and offering them the opportunity to present their work to quality committees. The front-line nurses were recognised by the nurse champion and given a US$5 coffee shop gift card. A critical change during the PDSA 1 was to introduce a medical directive, a structural enabler, that empowered nurses and saved physicians time from unnecessary interruption (online supplementary appendix D). It gave nurses the authority to remove urinary catheters without a physician’s order if the urinary catheter was no longer required by the patient based on an evidence-based algorithm adapted from Leis et al (online supplementary appendix B).15 Using this algorithm allowed the nurses to respond to patients’ needs in a timely manner and eased the use of guidelines. An additional structural ability was achieved by reporting back results and using a wall poster as an additional visual cue.
Supplemental material
Measures and analysis
Audits were conducted twice a week to determine patients with urinary catheter and whether patients met criteria of appropriate urinary catheterisation. If a urinary catheter had been inappropriately placed as determined using the algorithm and appropriate catheterisation criteria, the nurse in charge of the patient was notified to rectify the situation. The primary outcome was number and percentage of patients with catheters who met the appropriate catheterisation criteria.\
Patient and public involvement statement
Patients and public were not involved.
Results
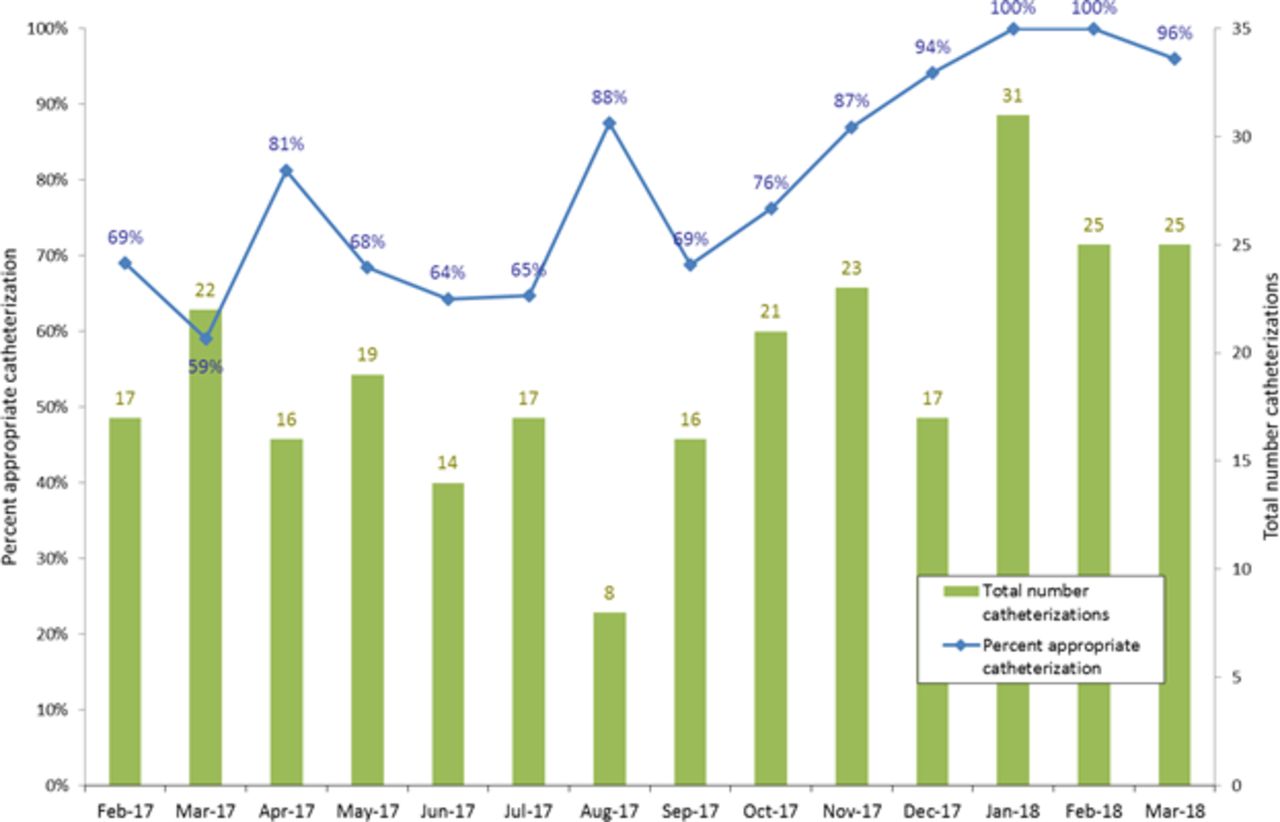
A total of 224 patients with urinary catheters were assessed over 13 months. Before the intervention, 69% of patients with a urinary catheter had appropriate indications for its use, meaning 31% of patients with a urinary catheter did not require it (figure 1).
{kind=link}
Appropriateness of catheterisation before and after intervention. Zero months indicates pre-intervention measurements. The percentage of patients with urinary catheters who met the CDC criteria are shown in blue. The sample size for each audit is shown in green. Our quality improvement project target of 85% shown in red has been achieved. Implementation of PDSA 1 interventions occurred at months 1 to 6 and PDSA 2 from months 7 to 12. CDC, US Centers for Disease Control and Prevention; PDSA, Plan-Do-Study-Act.
No significant change was seen during PDSA 1 of this study. However, significant improvement was seen after implementation of the changes in PDSA 2. The baseline inappropriate urinary catheter use decreased from 31% at the beginning of the study to 0% by month 10 (table 3).
Percentage of appropriate catheterisation before and after intervention
Discussion
Before the study, urinary catheters were being inappropriately used in 31% of inpatients who had a catheter. Ten months into the intervention, this percentage was reduced to 0% and held consistent over month 11. Application of the Influencer Change Model and the Choosing Wisely Guidelines proved to be effective in decreasing inappropriate urinary catheter use.
Furthermore, significant improvement was seen after implementation of PDSA cycle 2. The selection of champions allowed the team to harness peer pressure and motivated healthcare staff to put more effort into following hospital protocol. To date, several studies have commented on the strong impact champions13 19–21 and medical directives15 22 can have on improving proper urinary catheter use, and we believe that this effect was seen at WDMH as well.
The urinary catheter removal medical directive and algorithm successfully decreased improper urinary catheter use at WDMH. Initially, nurses would have to wait for orders by physicians before a urinary catheter could be removed. By allowing nurses to remove catheters on their own, the directive greatly simplified the process for both physicians and nurses. It also held nurses accountable for their patients, giving them more incentive to follow guidelines. Since the medical directive and algorithm was made available, nurses became more proactive with removing urinary catheters.
Effective reduction of inappropriate urinary catheter use to 0% was mainly due to the implementation of several interventions simultaneously and consistently over a long period of time (11 months). It is difficult to ascertain the influence of each intervention separately or to determine which intervention resulted in the most significant impact. Several other studies have also demonstrated significant reduction in inappropriate urinary catheter use through implementing bundles of interventions.7 23 24 These appear to be more effective than single interventions.5 25
At a rural hospital such as WDMH, efficient time and resource utilisation are key. By leveraging the usage and capabilities of the different characters in healthcare, we attempted to reduce unnecessary workload and cost. This simple implementation model and plan leveraged the front-line staff and simple interventions to bring about a sustainable change in appropriate catheter use.
Limitations of this study included a lack of statistical significance due to a small sample size. In addition, the ability to convey a hospital-wide goal to healthcare staff and the relationship/teamwork between employees in a rural setting may differ from that in an urban environment. Thus, similar results may be obtained by other rural hospitals, but it may be necessary for urban or larger organisation to implement different change motivators and champions to achieve the same results.
Conclusion
This study demonstrates bundles of interventions that successfully improved the appropriate use of catheters, empowered front-line staff and created sustainable changes in behaviour that leads to better patient care. The change model was used at WDMH to enable the healthcare workers and medical professionals to positively impact the care of their patients by using verified protocols more stringently. Adopting these learnings could also enable other hospitals to increase their healthcare quality indicators and become leading providers of healthcare.
Acknowledgments
The authors would like to thank Emily Mulligan, Amanda Pinches, the WDMH staff and physicians for their cooperation and hard work during this project.
References
Footnotes
Contributors Concept and design: MG, JC, FH, LH, KW, CC, SB, ML, AP, DT. Acquisition of data: MG, LH, CC, SB, ML, AP. Analysis and interpretation of data: MG, JC, FH, DT. Drafting of the manuscript: MG, FH, DT. Critical revision of the manuscript: JC, LH, KW, CC, SB, ML, AP. Administrative support: LH, SB, ML, AP. Study Supervision: MG.
Funding This quality improvement project was funded by the Late Career Nurse Initiative which was provided by the Ministry of Health and Long-Term Care.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval Ethics exemption for this quality improvement study was granted by the WDMH Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All statistics come from data that is de-identified participant data. Data is available upon reasonable request. For more information, please contact research@wdmh.on.ca.