Article Text

Abstract
Introduction Adrenal incidentalomas are lesions that are incidentally identified while scanning for other conditions. While most are benign and hormonally non-functional, around 20% are malignant and/or hormonally active, requiring prompt intervention. Malignant lesions can be aggressive and life-threatening, while hormonally active tumours cause various endocrine disorders, with significant morbidity and mortality. Despite this, management of patients with adrenal incidentalomas is variable, with no robust evidence base. This project aimed to establish more effective and timely management of these patients.
Methods We developed a web-based, electronic Adrenal Incidentaloma Management System (eAIMS), which incorporated the evidence-based and National Health Service–aligned 2016 European guidelines. The system captures key clinical, biochemical and radiological information necessary for adrenal incidentaloma patient management and generates a pre-populated outcome letter, saving clinical and administrative time while ensuring timely management plans with enhanced safety. Furthermore, we developed a prioritisation strategy, with members of the multidisciplinary team, which prioritised high-risk individuals for detailed discussion and management. Patient focus groups informed process-mapping and multidisciplinary team process re-design and patient information leaflet development. The project was partnered by University Hospital of South Manchester to maximise generalisability.
Results Implementation of eAIMS, along with improvements in the prioritisation strategy, resulted in a 49% reduction in staff hands-on time, as well as a 78% reduction in the time from adrenal incidentaloma identification to multidisciplinary team decision. A health economic analysis identified a 28% reduction in costs.
Conclusions The system’s in-built data validation and the automatic generation of the multidisciplinary team outcome letter improved patient safety through a reduction in transcription errors. We are currently developing the next stage of the programme to proactively identify all new adrenal incidentaloma cases.
- cost-effectiveness
- continuous quality improvement
- Decision support, computerised
- Diagnostic errors
- Healthcare quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- cost-effectiveness
- continuous quality improvement
- Decision support, computerised
- Diagnostic errors
- Healthcare quality improvement
Problem
Adrenal incidentalomas are lesions incidentally detected during abdominal imaging for other disorders. While most are benign, 3%–6% are malignant, rapidly progressive and life threatening. A further 12%–15% are hormonally active (including Cushing’s syndrome, phaeochromocytoma and Conn’s disease), with significant morbidity and mortality (eg, diabetes, uncontrolled hypertension, sudden death). Management of patients with adrenal incidentalomas and the approach to their investigation and follow-up are variable, both within and between centres. This often leads to overinvestigation (wasting National Health Service (NHS) resources) and underdiagnosis (missing potentially life-threatening lesions) and can result in extended delays in diagnosis and treatment. This variability in testing can lead to delays in treatment, which may result in a lack of patient engagement. This lack of engagement reduces patients’ understanding of the process, further increasing their anxiety.1
CT and MRI scan requests are being increasingly incorporated into diagnostic pathways. At University Hospitals of North Midlands NHS Trust, the number of abdominal CT scans has increased fourfold, exceeding 12 000 per annum over the last 6 years. There was a similar trend at our partner, the University Hospital of South Manchester Foundation Trust. Consequently, more adrenal incidentalomas are being identified. With a reported incidence of 4% in radiological studies,2 400–500 cases are identified annually for both our centres, 20% of which are potentially functional or malignant.3 This equates to an estimated total UK incidence of around 50 000 new adrenal incidentalomas annually (of which 1500 will be malignancies and 6000 will be functional lesions).
The sheer volume of cases is extremely difficult for any health system to cope with. If all these cases are proactively evaluated, as they should be, this would be equivalent to 25% of University Hospitals of North Midlands’ total block contract for new endocrinology referrals. These are presently not accounted for within the contract, despite 20% being potentially hormonally active or malignant.
Despite University Hospitals of North Midlands having a dedicated multidisciplinary team, initial data showed the median time (and IQR) between the patient receiving the radiological scan and multidisciplinary team deciding how to treat the patient was 6.00 (4.00–9.00) months. The median number of patient visits was 4.00 (3.00–4.25) and the median number of letters generated was 7.00 (5.50–8.50). Centres with no multidisciplinary team will likely have longer delays between scan and treatment decision and involve more patient letters and visits.
Given the above, adrenal incidentalomas are a major challenge, requiring an urgent and unified approach.1 4 We therefore decided to undertake a quality improvement project to better manage these patients, including developing a new adrenal multidisciplinary team process and electronic patient management system (eAIMS). We aimed to improve clinical safety around management of patients with adrenal incidentaloma, to reduce the time from initial identification of the adrenal incidentaloma to multidisciplinary team decision, and also to enhance cost-effectiveness. We also wanted to proactively identify all adrenal incidentaloma cases and optimise these into high-risk or low-risk categories to ensure that treatment was received at the appropriate level and speed.
Background
The significant variability in the approach to treating patients with adrenal incidentalomas stems from the fact that there were no UK NHS-compatible guidelines for managing the condition. Guidance has limited utility, as highlighted in a NHS report confirming that adrenal incidentalomas are a common clinical dilemma and the majority of affected patients are inappropriately investigated.5
A recent literature review (using search terms including ‘adrenal incidentaloma management’ and ‘adrenal incidentaloma guidance’) indicated that US/European guidelines have been largely based on retrospective, limited and often conflicting data relating to thresholds and timelines for planning investigations.6 7 NHS management plans are not driven by insurers or fee-for-service payments (unlike US/European-based systems), limiting the relevance of these guidelines to the UK.
A study from a UK district general hospital identified 75 patients with adrenal incidentalomas in 2010.5 The majority (80%) received no biochemical investigation or follow-up, with only 13 (17%) referred for specialist review and two further patients undergoing additional evaluation in primary care. A further UK study, focusing on biochemical investigations, accepted that, for patients with adrenal incidentaloma, ‘Their best management strategy is unknown’.8 The medical literature emphasises international acknowledgement that these tumours pose a management dilemma,9 but there is no NHS-compatible system to ensure appropriate management.
In summary, these studies highlight the lack of consensus regarding adrenal incidentaloma management. There is a risk of missing serious conditions that could be life threatening (including phaeochromocytoma and excess cortisol production) and that require rapid intervention. Many patients who ultimately do not require further follow-up need appropriate and timely investigation and effective communication to avoid unnecessary distress.
Our proposal, therefore, aimed to combine the new NHS-compatible European adrenal incidentaloma guidelines with information technology (IT) infrastructure and NHS-based referral processes to establish the first streamlined, clinically effective, patient-centred electronic Adrenal Incidentaloma Management System (eAIMS). This is highly innovative because it is
Evidence-based: eAIMS uses newly developed guidelines appropriate for integration into NHS processes (acknowledging the magnitude of the problem, referral processes and patient safety).
Multidisciplinary: Involving all key stakeholders (patients, commissioners, radiologists, clinical biochemists, hospital IT and Service Transformation experts as well as acute hospital physicians) in the design and evaluation from the outset.
Patient-orientated: Engaging patients in designing eAIMS (eg, steps followed in investigating and communicating results) and development of information leaflets. Patients will also help in evaluation via a survey of impact on anxiety.
Embedded: By involving IT experts and Service Transformation teams, this System will be embedded into routine clinical pathways for adrenal incidentaloma management.
Efficient: Exploiting IT to establish an integrated management system to facilitate interaction between the different steps and specialists in the pathway, ensuring timely investigations, multidisciplinary team interpretations, and communication with patients and general practitioners.
Cost-effective: Eliminating unnecessary investigations, outpatient visits and interventions10 (independently evaluated by University of East Anglia).
Generalisable: By selecting two sites with differing demographic populations and approaches to adrenal incidentaloma management, the potential for roll-out across the wider NHS is more assessable.
Addressing an unmet need: There is currently no system to address this gap in proactively managing patients with adrenal incidentalomas.
Measurement
Despite the advantage of University Hospitals of North Midlands having their own dedicated multidisciplinary team, our own initial data showed that the median (IQR) time between the patient having their radiological scan and multidisciplinary team decision on how to treat that patient was 6.00 (4.00–9.00) months, the median number of patient visits was 4.00 (3.00–4.25) and the median number of letters generated (sent to the patient or his or her general practitioner or the referrer) was 7.00 (5.50–8.50).
Our outcome measures (for the current study) were as follows:
Primary
Time from initial radiological detection to multidisciplinary team decision
We aimed to reduce the median time from initial radiological detection of the adrenal incidentaloma to multidisciplinary team decision by 20% (from 6.00 to 4.75 months based on University Hospitals of North Midlands data).
Two additional or secondary measures focused on safety aspects of adrenal incidentaloma patient management. The first of these was a reduction in the number of functional tumours missed or not actioned, compared with retrospective audit data. The second was a reduction in the number of malignant tumours missed or not actioned.
Process measures
The time taken from initial identification of an adrenal incidentaloma to a multidisciplinary team decision was expected to be shorter and less variable compared with the current practice. It was possible to break this part of the patient pathway down into five component parts or stages. The first is the time taken from the date an adrenal incidentaloma is identified to electronic referral to a consultant. The second stage is the time from this referral to a patient clinic appointment date. The third stage is the time from this clinic appointment to the resulting tests being completed (ie, results known). From this, the fourth stage is the time until the patient is reviewed at a multidisciplinary team meeting. The final stage is the time from multidisciplinary team discussion to the multidisciplinary team decision.
Design
Course of intervention
The intervention was developed through four distinct, interlinked processes. First, we re-designed the adrenal incidentaloma pathway. This was achieved by developing a prioritisation strategy, in collaboration with the radiology and biochemistry multidisciplinary team members. This ensured that high-risk individuals were prioritised for detailed prompt discussions, while streamlining the process for low-risk cases. These were classified in accordance with European guidelines. For example, lipid-rich lesions on scanning, with no evidence of excess hormone production, were considered low-risk while those with evidence of excess hormone production and/or lipid-poor (or expanding) lesions were considered as high-risk. Patients with a risk of malignancy were fast-tracked for discussion at the next multidisciplinary team meeting, in line with the UK ‘2-week wait’ principles.
Next, we developed the eAIMS. This was done in collaboration with University Hospital of South Manchester and the IT teams at both NHS Trusts. This system captures the key information on all adrenal incidentaloma cases and generates a pre-populated outcome letter, saving both clinical and administrative time and effort while ensuring a timely management plan with enhanced safety (achieved through reduced need to re-dictate and type results, minimising transcription errors). The system is also aligned with the newly published European Guidelines for adrenal incidentaloma management and uses the same prioritisation strategy as described above.
The third stage was to use data obtained from patients to inform the process-mapping and the re-design of the multidisciplinary team process. Patients also helped to develop a patient information leaflet.
Finally, we used our partnership with University Hospital of South Manchester to explore the generalisability of the utility of the system. The system was conceived as web-based from the outset to facilitate wider adoption. We also established dialogue with national professional bodies to showcase the work.
Primary and secondary data used
Initially, the time from radiological detection of the adrenal incidentaloma to multidisciplinary team decision on how to treat the patient was our primary outcome. However, while we were developing the eAIMS, we had to accommodate rising numbers of largely low-risk cases while promptly handling the urgent complex cases. Therefore, we upgraded our processes to include clinical prioritisation for multidisciplinary team case selection. This meant that we exceeded our target of speeding up the process, even before the eAIMS system was implemented.
We therefore present data on the impact of these improvements on the time between identifying and making a decision on the nature of the adrenal incidentaloma, including any further management if needed. We also focus on three key benefits of the system, namely, safety, efficiency and cost-effectiveness.
The first of these identified benefits, safety, considered the proportion of patients currently being missed (identified by radiology as having an adrenal incidentaloma, but not referred for further evaluation). Using key terms, a database of CT scans with adrenal incidentalomas was created. A consultant radiologist and consultant endocrinologist reviewed the radiological and clinical data to identify those with genuine adrenal incidentalomas and the proportion referred for further evaluation. Based on expected prevalence data, we believed that most patients are missed.
The second benefit was improved efficiency, that is, the time taken, in terms of staff hands-on time, in processing each case. This was calculated based on discussion with the key staff who perform each step in the patients’ treatment pathway (secretary, endocrinologist, biochemist, radiologist, multidisciplinary team staff).
The final identified benefit was cost-effectiveness. To determine cost-effectiveness, the above data were independently assessed by a health economist to facilitate estimation of the cost impact of the intervention.
Strategy
Team
This included the clinical teams (including members from endocrinology, clinical biochemistry and radiology, urology from the two hospitals) who worked closely with the IT (IT trust management team on both hospital sites together with the programmer) and the project team (including the clinical academics, project management, study methodologist as well as independent statistician and health economy teams) to ensure this project was conceived and implemented.
Approach and organisation of intervention
The initiative was triggered by the observation that the workload emanating from management of adrenal incidentalomas was escalating significantly. We also noted that the process included much repetition, wasting clinical and administration time. The median time from detection to decision was also noted to be long in many cases, with many patients reporting anxiety and distress. Almost all had to resort to the internet for information, which compounded their uncertainty.
This led us to review the literature to assess current evidence on clinical management and process-related initiatives for these patients. We also reviewed the existing approach to managing adrenal incidentalomas, leading to a process mapping exercise. We then used stakeholder groups to develop a driver diagram to assist in the development of the interventions. Finally, we developed a number of Plan-Do-Study-Act (PDSA) cycles as follows:
PDSA cycle 1
We initially identified the main problem: that patients with newly diagnosed adrenal incidentaloma were waiting, on average, 6 months between initial identification of the lesion and multidisciplinary team decision.
We developed a prioritisation strategy based on available guidance to ensure patients with lesions requiring urgent attention (eg, cancer) will be given priority for discussion in the multidisciplinary team meeting. This was discussed and agreed among the team members.
PDSA cycle 2
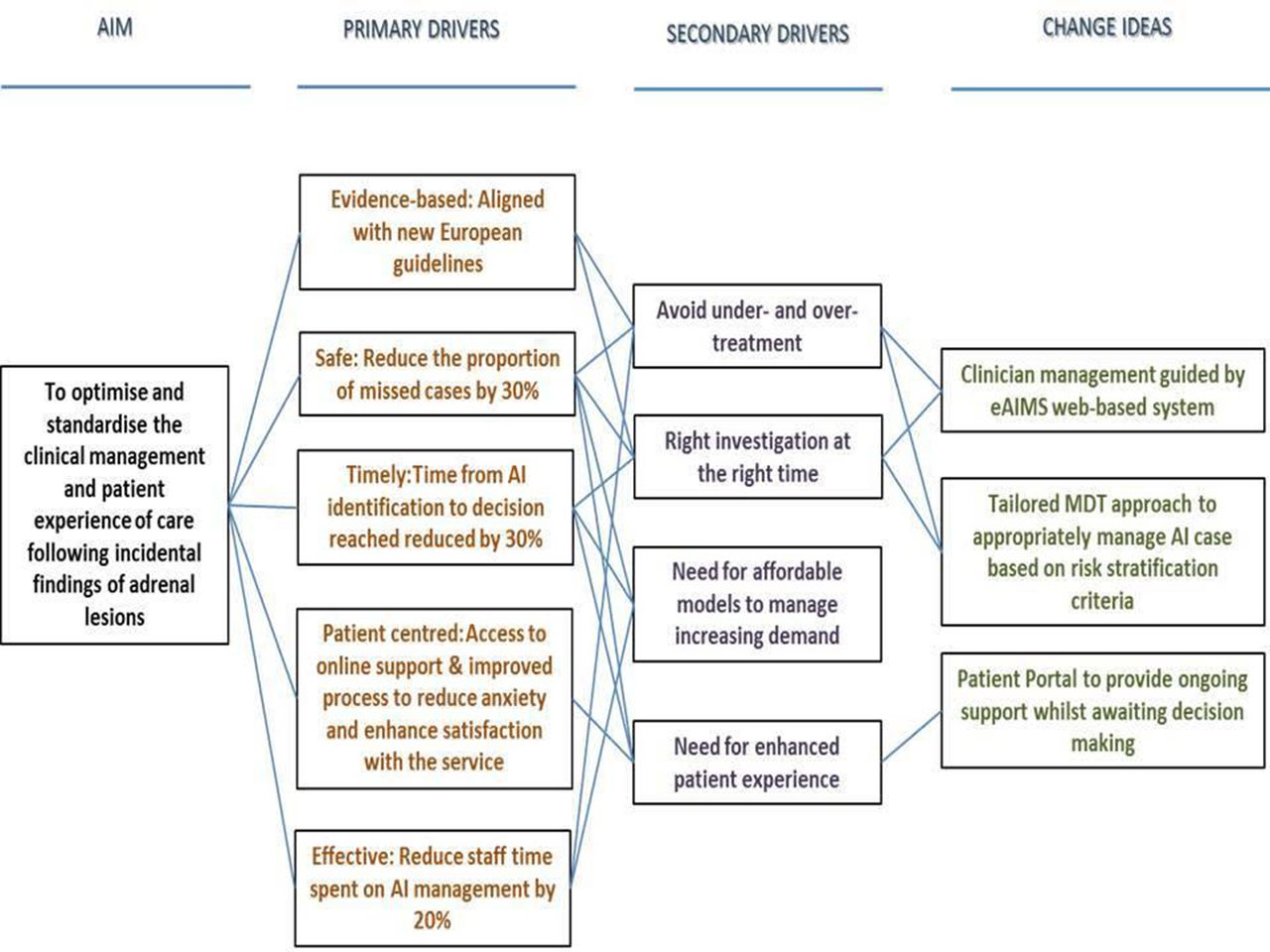
Faced with the ongoing pressure on the service from the process of managing adrenal incidentaloma referrals, with its impact on staff time and potential delay incurred, we created a driver diagram to assess the main reasons for this delay, which led to identification of ideas for change (figure 1).

Driver diagram showing the main drivers to address the shortfalls in adrenal incidentaloma management, with potential solutions provided by the electronic Adrenal Incidentaloma Management System (eAIMS) and revised processes. MDT, multidisciplinary team.
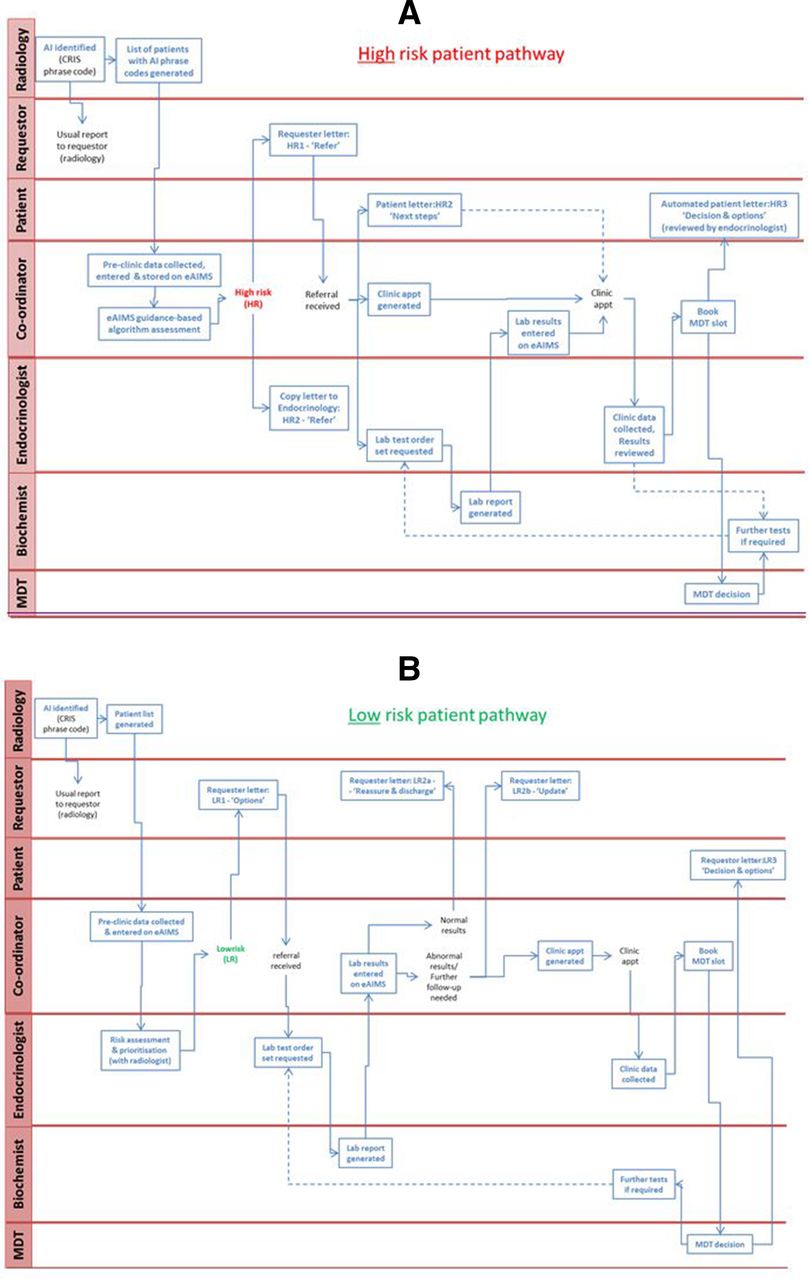
We then held a focus group with patients who had been treated for adrenal incidentalomas to discuss our proposed ideas for change and our suggested approach. Importantly, the patients identified key elements in terms of timings in order to inform the generation of the new process map. For example, they identified that it was important to progress the laboratory investigations while awaiting a clinic appointment rather than waiting to be seen in the clinic before investigations were initiated. The proposed new process map (figure 2) informed the specification for the development of the web-based eAIMS system. Patients were identified as low-risk based on the radiology report (lipid-rich and/or stable lesion in comparison with earlier scans) and functional status. The effectiveness of the eAIMS was assessed by (1) a time-and-motion study to evaluate hands-on time, and (2) a cost-effectiveness analysis.
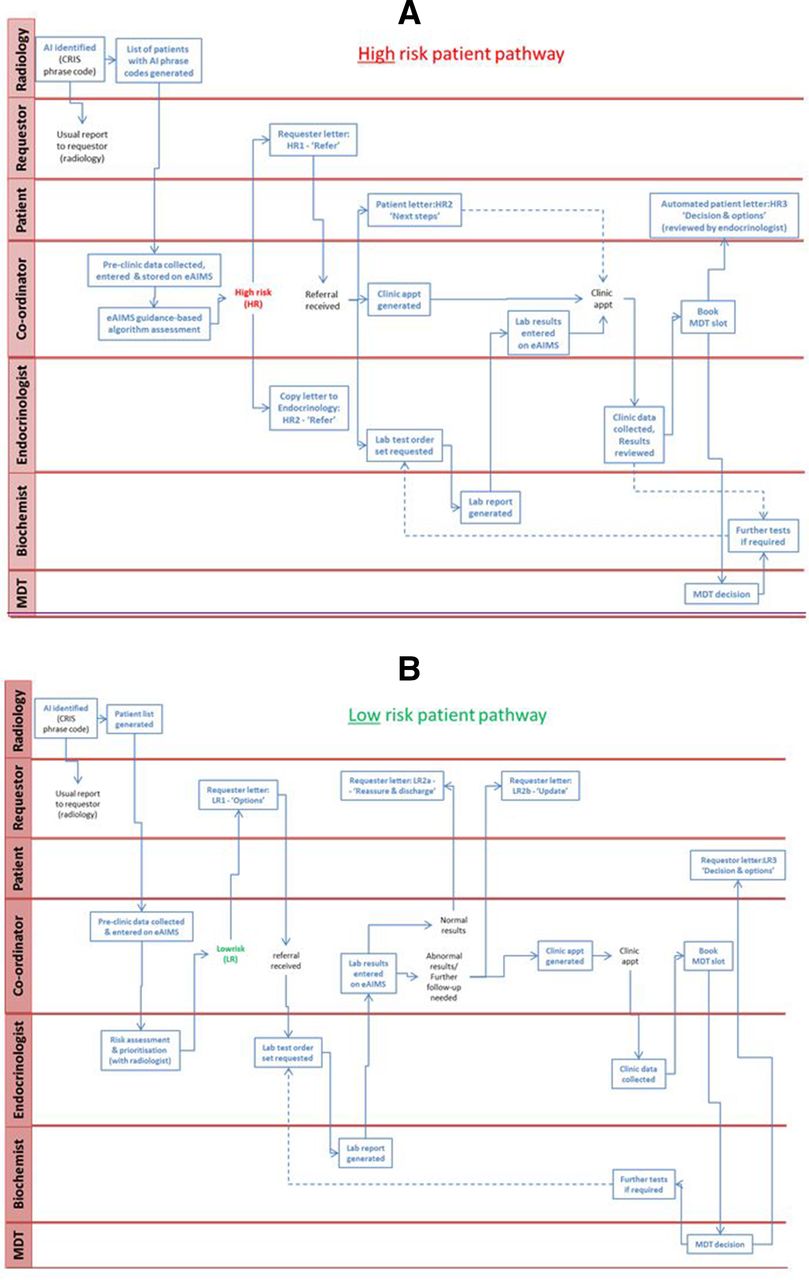
Process map following risk stratification for (A) high-risk patients and (B) low-risk patients. eAIMS, electronic Adrenal Incidentaloma Management System; MDT, multidisciplinary team.
During this process, it became clear that many adrenal incidentaloma cases may have not been referred to endocrinology (based on the disparity between the expected number and those actually referred). We therefore instigated an assessment to determine the proportion of cases that were being missed. This required the collection of retrospective radiological data using ‘key phrases’ in the reports. It identified that a significant proportion of cases were being missed (see Results section).
PDSA cycle 3
Given the ongoing dependence on CT and MRI scans, together with the increasing awareness of adrenal incidentalomas, we became acutely aware of the inevitable increasing number of referrals. We are currently implementing further change to allow the endocrinology team to manage the additional workload. This involves the development of a pre-multidisciplinary team streamlining process, which is based on the time and motion study and linked cost-effectiveness analysis. We have also involved patients to gauge their thoughts on how to provide support during the waiting process. While this allowed the development of a patient leaflet (with patient input), it is planned that this will eventually feed into the development of a patient portal within eAIMS. This will provide information for patients using frequently asked questions generated from a pool of existing patients.
Challenges
During the project, we identified three key challenges. The first of these was the importance of being able to automatically generate letters via the eAIMS platform. While this was outside the original project’s plans, it was still prioritised and subsequently developed. Second, clinical and biochemical data are entered manually by a multidisciplinary team co-ordinator. We are currently enhancing the platform’s capability to interface with existing hospital systems in order to minimise manual data entry and hence reduce the risk of errors. Finally, the need for generalisability became obvious early in the project and hence we opted for a web-based solution.
Results
This study was designed to develop a new process for managing patients with adrenal incidentalomas. This comprised the development and testing of a novel digital solution followed by its evaluation and integration into clinical practice. These two components are described below.
eAIMS system development
We successfully developed eAIMS, including
Conceptualisation: Discussion among key stakeholders to agree the system requirements and associated deliverables.
Specification development (with Trust IT collaboration): Based on process mapping (figure 2) and discussion with IT colleagues, the concepts were translated into an IT-compliant NHS system specification document.
Prototype development: A Trust-assigned IT programmer translated the specification into an initial prototype, which was then subjected to several iterations based on ongoing discussions with the project team.
Information governance compliance assessment: As an integral part of ensuring information governance requirements were fulfilled, especially given the web-based nature of the product, the Trust Information Governance team were engaged to ensure compliance.
Technical testing and de-bugging: Following the development of the initial prototype, a comprehensive and rigorous testing protocol was undertaken, using a series of testing scripts based on clinically relevant scenarios, to ensure optimum system performance.
Real-world system testing and revision: After completing IT-instigated assessments, the system was assessed using real patient data. This enabled identification of areas for improvement of data entry. This process included the key step of generating an automated multidisciplinary team outcome letter, enhancing the potential of the system to be scaled up and adopted at other centres.
Implementation. The system was implemented into clinical practice. A demonstration (with fictional patients) is available online (http://mi.cx/eaims-phase1-demo.mp4).
eAIMS system and process evaluation
Our initial objective was to reduce the delay between adrenal incidentaloma identification and multidisciplinary team decision by 20%, from 6 months (pre-project) to 4.8 months. As a result of this project, a stepwise reduction in this delay was observed as different elements of the programme were implemented, resulting in a markedly greater reduction in the time to multidisciplinary team decision than originally anticipated. For example, introduction of the improved prioritisation of cases within the multidisciplinary team resulted in the median delay being reduced by 58.3% to 2.50 months (figure 3), while implementation of the eAIMS system reduced this further to 1.25 months (78.3% total reduction in delay).

Median time between adrenal incidentaloma identification and multidisciplinary team (MDT) decision, before and after electronic Adrenal Incidentaloma Management System (eAIMS) implementation.
Balancing measure: proportion of missed adrenal incidentaloma cases
During the implementation of the eAIMS system and associated process redesign, it became clear that not all adrenal incidentaloma cases were being appropriately referred. We therefore assessed the proportion of these cases as a balancing measure. To evaluate this, data on adrenal lesions reported on CT scans were collected from 2014 to 2016, focusing on the referral for the month of November each year as a representative sample (table 1).
Adrenal incidentaloma cases referred to endocrinology
Key phrases from radiology reports were used to identify cases linked to possible adrenal lesions. These included the terms Adrenal adenoma, Adrenal incidentaloma, Adrenal lesion, Adrenal mass, Adrenal nodule, Incidental adrenal and Indeterminate adrenal.
Patients with known cancer were excluded and those with genuine adrenal incidentalomas were then checked (based on multidisciplinary team note entry and/or review of endocrinology letters) to confirm whether or not they were acted on and were referred to endocrinology for further assessment.
Analysis showed that, despite having a dedicated multidisciplinary team and service, which is not routine practice in most centres in the UK and globally, only ~30% of cases were referred for evaluation. This means that even in the presence of a dedicated team and spreading knowledge, 70% of adrenal incidentalomas were being missed.
The eAIMS and prioritisation process will enable detection of these missed cases to be highlighted to referring clinicians and general practitioners. The additional workload would be circumvented by the implementation of the more efficient and streamlined process, underpinned by the eAIMS.
An independent health economic assessment, led by the University of East Anglia, assessed the hands-on time of clinical staff at three phases. Phase I was prior to the project implementation. Phase II was the time period following implementation of the multidisciplinary team prioritisation process and the eAIMS go-live. The final phase, phase III, is the proactive adrenal incidentaloma identification and case streamlining process (post-project phase currently being implemented).
The impact of these phases (figure 4) showed that the estimated cumulative time taken for progressing each case was: phase I, 168 min; phase II, 115 min; and phase III, 66 min.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Time-and-motion study showing the estimated time managing an individual adrenal incidentaloma case for each of the phases of the process: (I) pre-intervention, (II) eAIMS implementation with case prioritisation and (III) proactive case identification and streamlining into low-risk and high-risk groups. eAIMS, electronic Adrenal Incidentaloma Management System; MDT, multidisciplinary team.
The cost impact of this phased change was then evaluated using standardised staff costs, in conjunction with a novel Adrenal Incidentaloma Intervention Cost Assessment Tool. This analysis showed that the combination of using a multidisciplinary team prioritisation process and introduction of the eAIMS (phase II) significantly reduced the number of steps and tasks in the patient management process, the total time taken (from adrenal incidentaloma identification to multidisciplinary team decision) by 48.6% and the total costs associated with treating each patient by 28.2%.
As a result of the focus group discussions, we developed a simple patient leaflet. We will hold further focus groups on both sites to review this and include frequently asked questions. These will be uploaded onto eAIMS on a patient-accessible section for online support.
Lessons and limitations
Evolution of our understanding of the financial impact
The time taken to progress a case through the system from identification until multidisciplinary team decision was costed, using standardised NHS costs for both administrative and clinical time.
The total cost per case was then evaluated, comparing phase I (pre-project) against phase II (the implemented project, with eAIMS implementation and prioritisation process).
However, we have always been focused on the fact that a key deliverable was the identification of all adrenal incidentaloma cases. Even with a dedicated well-publicised multidisciplinary team, only 30% of University Hospitals of North Midlands’s adrenal incidentalomas were referred. We have therefore developed our practices to allow us to streamline the process even further to enable the handling of more cases in a cost-effective manner. Our projected (phase III) figures are encouraging. These will be formally evaluated, using the specifically designed adrenal incidentaloma cost attribution tool.
Calculation of the cost of the intervention
To facilitate the development of a web-based system within the tight time frame of the project, we had to appoint a dedicated IT programmer. This meant we had to change the original costing allocations awarded by the funder, the Health Foundation. This was shared with, and approved by, the funder early on.
Implementation costs
Quality Improvement projects often struggle with financial hurdles on implementation. We were pleased that phase II evolved seamlessly and no additional cost implications to the grant arose. This was facilitated by the fact that the Trust noted the additional workload created by the adrenal incidentaloma project and appointed an additional band four multidisciplinary team co-ordinator (this could be viewed as a positive balancing measure).
Commissioning challenges
Each patient with adrenal incidentaloma referred to us is costed as a new case, as per an agreement with the Clinical Commissioning Group.
Based on our data (that we receive only 30% of patients with adrenal incidentaloma as referrals) and the projected surge in adrenal incidentaloma cases to be identified and processed (~500 cases per annum in our Trust, projected to an estimated 50 000 cases per annum across the UK), we are engaging the service commissioners to agree the most suitable and cost-effective way to manage these cases.
The system we have developed (eAIMS) will enable us to detect all these missed cases. We can highlight them to their general practitioners and, if they wish, we will process them efficiently through our streamlined multidisciplinary team process and electronic management system. Our system and pathway will handle more cases within the existing budget limitations, given the more streamlined and efficient approach, while also removing waste and enhancing safety. We are engaging with other Trusts, and with national professional bodies, to facilitate wider uptake and spread of our patient management processes. This could also be the beginning of a national registry that will, in the future, form the evidence-based data required to inform further guideline development.
Endocrinology engagement/capacity
Endocrinology colleagues could fear being swamped by the many extra, proactively identified, adrenal incidentalomas that were previously missed or lost in the system. Our approach, using eAIMS, has been confirmed to reduce the time spent per patient, with a corresponding reduced cost. We shared this with a cohort of our colleagues in the Autumn meeting of the Association of British Clinical Diabetologists (London, November 2017). This was well received, with many clinicians indicating that the process improvements were necessary to enable clinicians to cope with the workload. Many clinicians were appreciative of the patient support approach and indicated they would consider supporting the management of their patients using such an approach.
Conclusion
Faced with the challenge of increasing adrenal incidentaloma patient workload, together with limited guidance on how to manage these cases effectively, we undertook this quality improvement initiative.
First, we re-designed the adrenal incidentaloma clinical management pathway, developing a prioritisation strategy, in collaboration with radiology and biochemistry multidisciplinary team members. This ensured that high-risk individuals were prioritised for detailed prompt discussions, while streamlining the process for low-risk cases.
We also developed a web-based patient management system (eAIMS). This captures the key information on all adrenal incidentaloma cases and generates a pre-populated outcome letter, saving both clinical and administrative time and effort while ensuring a timely management plan with enhanced safety (reduced need to re-dictate and type, thereby minimising transcription errors). The system is aligned with the recently published European guidelines for adrenal incidentaloma management.
The eAIMS system and multidisciplinary team process will enable detection of previously missed adrenal incidentaloma cases, of which 20% could be hormonally active or malignant. These cases can be highlighted to general practitioners. The additional workload would be circumvented by the implementation of the more efficient and streamlined process, underpinned by the eAIMS system.
We gathered patients’ views to inform the process mapping, helping to re-design the multidisciplinary team process to address the concerns expressed in our focus group discussion. Patient views also helped develop an information leaflet.
We have an established partnership with University Hospital of South Manchester. We used this to demonstrate the generalisability of the utility of the system. The system was conceived as web-based from conception to facilitate wider adoption.
Acknowledgments
The authors would like to thank Mr Chris Hale for his expertise in developing the eAIMS and Ms Helen Robertson for her help with the time-and-motion analysis and for helping to test the eAIMS in practice.
Footnotes
Contributors FFWH: project originator, project (clinical) lead (University Hospitals of North Midlands) and contributed to writing the paper. AAF: project (Clinical biochemistry) lead (University Hospitals of North Midlands) and contributed to writing the paper. SCL: project manager and contributed to writing the paper. BGI: project (clinical) lead (University Hospital of South Manchester) and contributed to writing the paper. MF: quality improvement contribution. JS: statistics and methodology. RF and GX: health economics. CG and AG: clinical management of AI cases and membership of the multidisciplinary team. EM: IT management and Trust adoption. SO supported the work in his capacity as a primary care clinician and also providing a commissioner’s perspective. All authors reviewed the manuscript.
Funding This study was support by a grant from the Health Foundation (GIFTS 7555: CRM 2216).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.