Article Text

Abstract
Background A high incidence of missed posterior shoulder dislocations is widely recognised in the literature. Concern was raised by the upper limb multidisciplinary team at a London major trauma centre that these missed injuries were causing serious consequences due to the need for surgical intervention and poor functional outcome.
Objective To identify factors contributing to missed diagnosis and propose solutions.
Methods A local quality improvement report was performed investigating time from admission to diagnosis of simple posterior dislocations and fracture dislocations over a 5-year period. Factors contributing to a delayed diagnosis were analysed.
Results The findings supported current evidence: a posterior shoulder dislocation was more often missed if there was concurrent fracture of the proximal humerus. Anteroposterior and scapular Y view radiographs were not always diagnostic for dislocation. Axial views were more reliable in assessment of the congruency of the joint and were associated with early diagnosis and appropriate treatment of the injury.
Discussion As a result of these findings a new protocol was produced by the orthopaedic and radiology departments and distributed to our emergency department practitioners and radiography team. The protocol included routine axial or modified trauma axial view radiographs for all patients attending the emergency department with a shoulder injury, low clinical suspicion for dislocation and a low threshold for CT scan. Reaudit and ongoing data collection have shown significant increase in axial view radiographs and improved diagnosis.
- continuous quality improvement
- diagnostic errors
- patient safety
- surgery
- teamwork
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Ninety-eight per cent of traumatic glenohumeral joint dislocations displace in an anterior direction.1 This is due to the anatomy of the joint and the more common mechanisms of injury forcing the humeral head anteriorly. Posterior dislocations are significantly rarer. The ‘textbook’ causes are electric shock and epileptic fit; however, in reality any high-energy injury may lead to a posterior displacement. It is well documented in the literature that these posterior injuries are often missed.1–5 Low clinical suspicion due to relative rarity may be one explanation but there are several others.
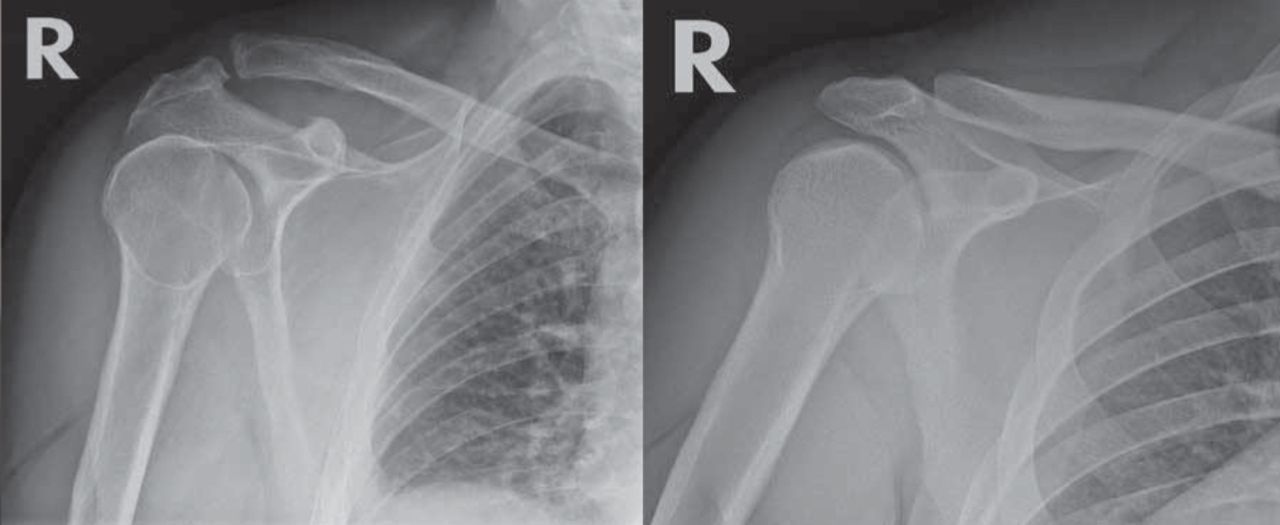
Traditionally clinicians are taught to look for the ‘light bulb’ sign on anteroposterior (AP) radiograph as pathognomonic of a posterior dislocation (figure 1). However, this radiological phenomenon may be unreliable since the patient is often immobilised in a sling at the time of imaging, therefore internal rotation views are to be expected regardless of injury. Scapular ‘Y’ views are routinely obtained to accompany the AP view but these vary considerably in quality and often do not contribute to diagnosis.

Light bulb sign due to internal rotation on left compared with posterior dislocation on right.16
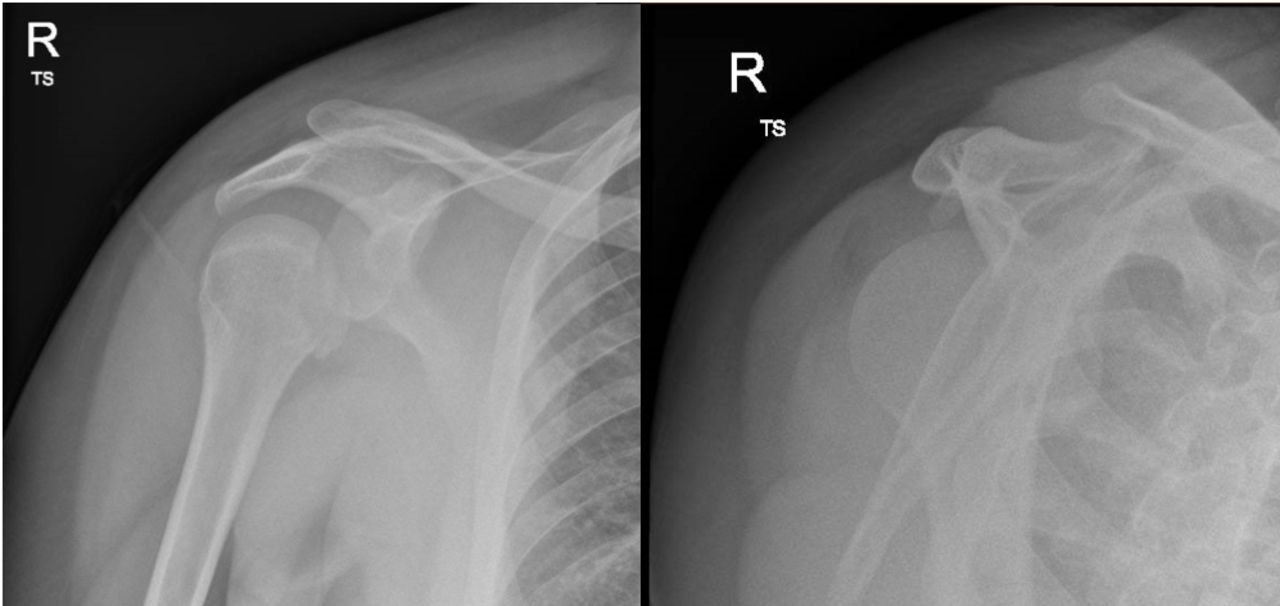
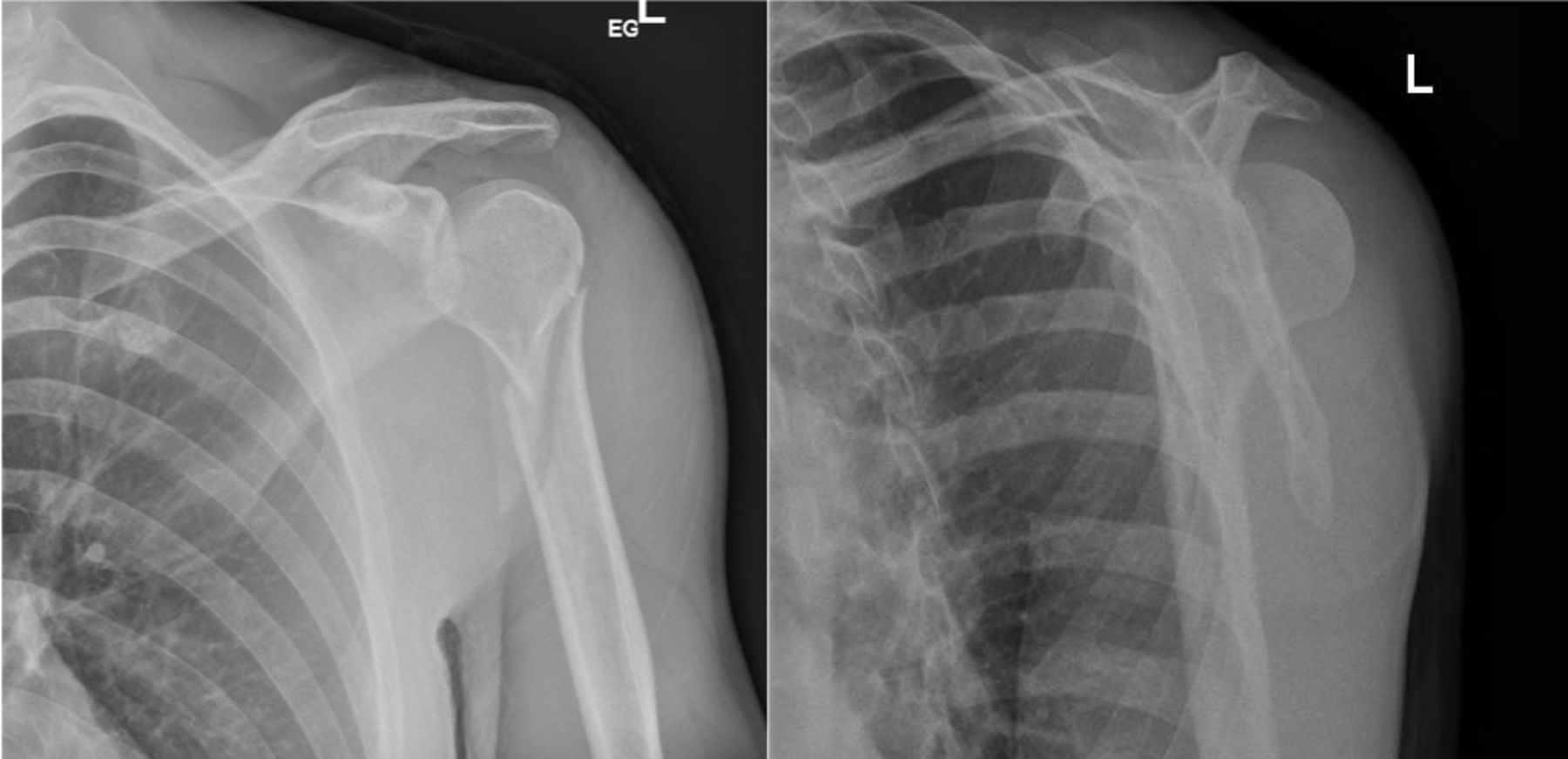
Dislocations may have an associated fracture of the proximal humerus.6 These fractures tend to be obvious on radiographs. More so than any associated dislocation. The radiological term ‘satisfaction of search’ describes how, after having found one abnormality on a study, individuals no longer continue to look hard enough at the remainder of the images. This may lead them to miss any concurrent additional injuries (figure 2). There may be a mistaken belief that if the patient has a proximal humerus fracture then this satisfactorily explains their presentation and symptoms, therefore no further investigation is necessary. As a result, it has been known for patients to be discharged home with their shoulder still out of joint. In particular, an apparently isolated fracture of the lesser tuberosity is almost always accompanied by posterior dislocation which may well be missed (figure 3).7–9 A perceived ‘simple’ proximal humerus fracture will often be dealt with by emergency department clinicians without involving the on-call orthopaedic team. The patient is given a collar-and-cuff sling and discharged to await an appointment in the fracture clinic.

Anteroposterior (AP) radiograph demonstrating a proximal humerus fracture. There is a concurrent posterior dislocation present though this is not obvious on the single view. The Y view demonstrates it more clearly.
Anteroposterior (AP) radiograph demonstrating a lesser tuberosity fracture. Once again only careful analysis of the Y view reveals the concurrent dislocation.
This satisfaction of search phenomenon combined with inadequate clinical examination may also mislead the attending physician to attribute the poor range of motion to fracture-associated pain rather than the true locked internal rotation of a posterior dislocation.
All these factors combined with low clinical suspicion due to the relative rarity of the injury means more reliably diagnostic forms of imaging such as an axial view of the glenohumeral joint or CT scans are not performed.
Background
Missed posterior dislocations of the shoulder can have serious consequences for the patient. The longer any joint remains dislocated the harder it is to relocate due to muscular spasm and capsular tightening.10 Closed reduction using Entonox or conscious sedation in the emergency department becomes more and more challenging the longer the delay. This increases the risk of requiring formal hospital admission, a general anaesthetic, plus closed or even an open reduction of the joint in the operating theatre. ‘Open reduction’ describes a surgical approach to the glenohumeral joint with direct reduction using surgical instruments. All surgical procedures have inherent risk including infection, blood loss and iatrogenic damage to surrounding nerves, vessels and tendons. All these can potentially be avoided with timely diagnosis and reduction in the emergency department.
Additionally, the primary arterial supply to the humeral head runs within the joint capsule. If this is under stretch due to prolonged dislocation, the blood supply may become compromised and lead to avascular necrosis (AVN) of the humeral head, a catastrophic complication causing collapse of the articular surface of the joint leading to pain and decreased range of motion that may require arthroplasty (joint replacement) surgery. This is a disaster in young or otherwise highly functioning patients.
Certain proximal humerus fracture patterns can damage the circumflex vessels supplying the humeral head. Primary injury during the traumatic event accompanied by prolonged dislocation may raise the risk of AVN significantly. Most posterior fracture dislocations require surgical fixation to restore the function of the joint. This may also help prevent subsequent AVN and possible collapse of the articular surface. Delayed definitive management leads to a worse prognosis and a higher likelihood of requiring arthroplasty.11
Specific aims
Concern was raised by the upper limb multidisciplinary team (MDT) at one of London’s major trauma centres that an unacceptably high number of posterior dislocations and fracture dislocations were being missed. Several instances were encountered of a patient presenting to a specialist upper limb fracture clinic with a shoulder that was still dislocated. This first review was often several days after injury.
The decision was made to investigate these patients and analyse what factors led to a delayed diagnosis both on a human and institutional level. Once analysed, the MDT would propose solutions to reduce this incidence.
Measurement
Data were collected retrospectively over a 5-year period (May 2012–2017). All patients admitted to the emergency department with a shoulder injury were investigated. Using our electronic care records system (Cerner) and the keyword search function on our picture archiving and communication system we identified all patients with a posterior dislocation and recorded time from admission to diagnosis and definitive treatment. All emergency department radiographs at our unit are routinely reviewed and reported by senior radiologists. This forms part of an existing system to highlight injuries that may have been missed on initial presentation. Indeed, several of the patients in this study were only flagged up due to this system.
We recorded the method of injury for each patient and analysed the documentation of initial clinical examination findings plus which radiological studies were performed. In particular, which radiological views were obtained. AP radiographs are the most common. They show the glenohumeral joint in a coronal plane. Scapular ‘Y’ views show a sagittal plane. The third standard view is the axillary or axial.
Our panel of consultant experts ruled that any diagnosis made more than 24 hours after presentation was classified as ‘missed’.
For patients who did not have their dislocation reduced in the emergency department or were classified as ‘missed’ we followed their clinical course and final outcome using the care records system and outpatient clinical documentation.
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research
Results
Over 5 years, a total of 34 patients were identified to have had a posterior dislocation. Of these, 23 were simple dislocations and 11 were fracture dislocations.
Only two injuries were due to a fit (6%), all others were secondary to trauma (94%).
Six of the 34 were diagnosed beyond 24 hours (18%). One hundred per cent of the simple dislocations were identified and reduced in acceptable time (table 1). However, 55% of the fracture dislocations were missed. Documentation by the emergency department clinicians in these cases recorded recognition of fractures but not of the associated dislocation. Of the missed dislocations 80% did not have an axial view performed (table 2). All the injuries that were not diagnosed on initial imaging were later diagnosed with a CT scan, some as late as 20 days after initial presentation.
Time of diagnosis of simple and fracture dislocations
Presence or abscence of Axial view in relation to missed dislocations
All fracture dislocations underwent surgical fixation by a consultant shoulder surgeon. Of the missed injuries two progressed to AVN. One of these required revision surgery to a hemiarthroplasty (replacement of the humeral head). Two required a primary hemiarthroplasty as fixation was deemed inappropriate by the surgeon at the time of operation. The injuries that were diagnosed and definitively treated within an appropriate time went on to have acceptable outcomes.
Discussion
Our results are consistent with current evidence. Fracture dislocations are more often missed than simple dislocations. Low clinical suspicion, lack of routine axial radiographs and the satisfaction-of-search phenomenon contribute to this high incidence.
Axial view radiographs have been consistently demonstrated to be the most sensitive diagnostic view for shoulder dislocation6 (figure 4). This is because the congruency of the glenohumeral joint is most easily assessed when looking in an axial plane. It is a routine diagnostic view of the shoulder; however, it requires the patient to abduct their arm to at least 30° in order to align the X-ray beam appropriately. On discussion with the radiology department, the low rate of axial images was partially explained by the practicalities of obtaining this standard axial view. The patient was unable to abduct their arm to the required position due to pain so the view was not obtained.

Axial view radiograph demonstrating obvious posterior dislocation of the humeral head.
Design and strategy
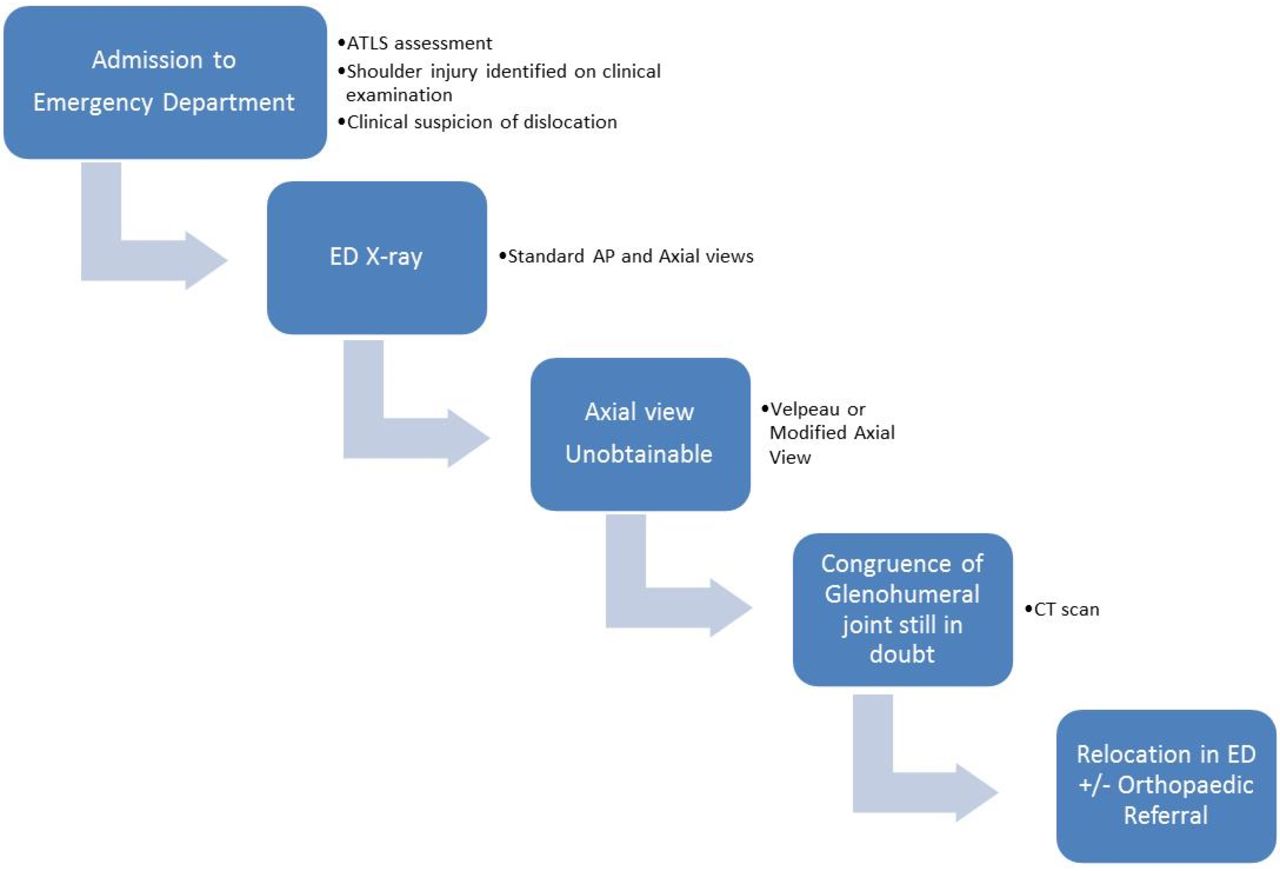
An MDT consisting of a consultant upper limb orthopaedic surgeon, two consultant musculoskeletal radiologists, orthopaedic and radiology specialist registrars and senior radiographers analysed these findings and devised a protocol designed to prevent missed injuries. This has been systematically introduced across the three sites within our trust via face-to-face seminars and email communications with both permanent and temporary staff (figure 5).

Protocol for management of shoulder injuries. AP, anteroposterior; ATLS, Advanced Trauma Life Support; ED, emergency department.
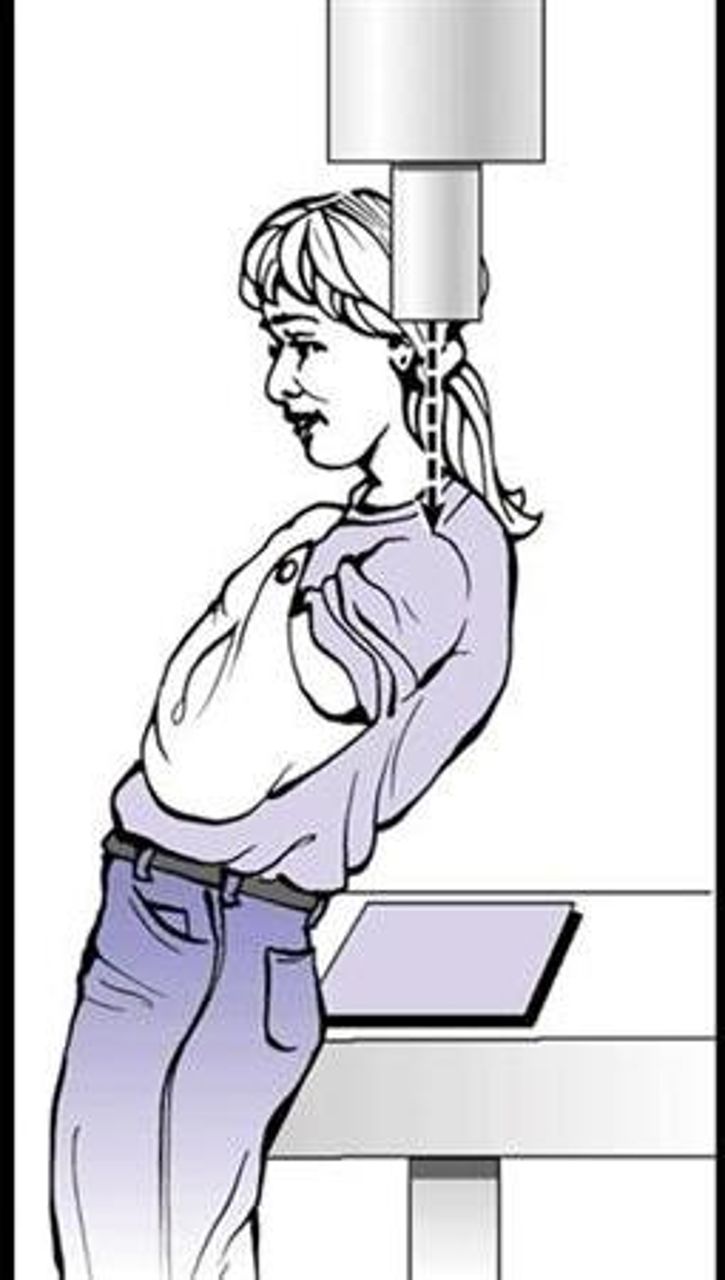
All patients admitted to our emergency department with a shoulder injury now receive AP and axial shoulder radiographs as routine. When the standard axial view cannot be obtained due to pain, a modified trauma axial or ‘Velpeau’ view is performed12 13 (figure 6). These views provide reliable assessment of the congruency of the shoulder joint without the need for the patient to abduct their injured arm.14 15 If, for any reason, adequate radiographs cannot be obtained a CT is performed as a matter of urgency.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patient position required to obtain a Velpeau view. The arm can remain in a sling therefore preventing pain.17
Compliance with the new protocol was audited by randomly selecting 40 cases (20 left shoulder and 20 right shoulder) during May 2018. Comparison was made with practice before the change in protocol. In May 2018, following the educational intervention, compliance with performing AP and modified trauma axial views for patients presenting to the emergency department with shoulder trauma as per the new protocol was 40% (16/40). In May 2017, before the change in protocol, modified axial views had been performed for 7.5% (3/40). This still fell below our target outcome so further cross-site education has taken place and repeated data collection shows ongoing increased compliance. This is an ongoing process and is driven by the orthopaedic and radiology consultants as well as the senior radiographer in the MDT which meets weekly.
Lessons and limitations
Sustainability of any new protocol is always a potential issue especially with constant staff turnover in the emergency and radiology departments. Today, should our upper limb MDT members identify any new cases of missed dislocation, steps are taken to ensure all current staff members remain educated about the pathway.
Conclusion
Where high-energy trauma causes a shoulder injury it is of vital importance to consider posterior dislocation. Delayed diagnosis has the potential to cause serious harm to patients and has significant implications for ongoing quality of life and function. Our study has revealed that incidence of missed posterior fracture dislocations remains high. A simple intervention such as our shoulder trauma imaging protocol can be widely distributed across the National Health Service and has the potential to significantly improve patient outcomes.
References
Footnotes
Contributors APM: study design, data collection, write-up, submission. CW: study design, data collection, implementation of quality improvement. NT: implementation of quality improvement. MW, DA, DG: study design, implementation of quality improvement.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.