Article Text

Abstract
A major challenge for hospitals in low-income and middle-income countries is to improve management of patients diagnosed with sepsis. The objective of the present study was to evaluate the Institute for Healthcare Improvement (IHI) Model as a strategy to implement a managed sepsis protocol aimed at reducing sepsis mortality. We performed a longitudinal, prospective, non-randomised study using PDSA cycles for translating and implementing improvement actions and tools. Baseline case mortality/case fatality data were collected, and compliance rates were evaluated according to the Surviving Sepsis Campaign guidelines (3-hour care-bundle). Sepsis multidisciplinary work teams were designated and were responsible to develop Driver Diagrams and implement process changes in the intensive care unit, wards and emergency department. Satisfaction levels of healthcare professionals were assessed (balance variables). The study was carried out in a public quaternary hospital, in São Paulo city, Brazil (Hospital Municipal da Vila Santa Catarina). The number of patients with sepsis studied was 416 who were followed over a 15-month period. The data analyses were carried out by statistical process control. Case fatality rates were kept below a prespecified target of 25% (15.9%) during the period. Satisfaction level of the participating staff was high (95.2%) and 71% of participants reported no work overload. The IHI model was found to be a feasible and useful strategy for implementing a sepsis management clinical protocol.
- clinical practice guidelines
- implementation science
- patient safety
- quality improvement methodologies
- PDSA
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- clinical practice guidelines
- implementation science
- patient safety
- quality improvement methodologies
- PDSA
Problem
Sepsis is one of the most frequent diagnosis in intensive care units (ICUs).1–4 Studies carried out in high-income countries extrapolated to low-income and middle-income countries suggest that, in these, the total prevalence of sepsis cases would amount to 85% of the world prevalence.1 5 In the past years, many healthcare institutions around the world started to seek ways to improve their quality and safety procedures. In this setting, prospective studies on the development of care bundles to reduce nosocomial infections emerged which improved the clinical outcomes.6–9 After the establishment of an international joint initiative named the Surviving Sepsis Campaign, medical societies and specialists from different areas committed to increase awareness about this neglected and highly relevant disease, and defined standards on how to diagnose and treat sepsis. In summary, evidence-based guidelines were developed, and a set of interventions was recommended (organised in 3-hour and 6-hour care bundles) to be carried out early in the phases of sepsis.10–13 Access to published medical advances is not a problem in modern society, but implementing new guidelines to the bedside of patients with sepsis poses several challenges.1 14–16 For instance, early presumptive diagnosis and medication are essential to successful sepsis treatment although no specific diagnostic tests exist for the early phase of this condition.
In more detail, current sepsis management relies on the use of bundles. Bundles are a group of interventions which, taken together and in a timely way, have a synergistic effect. This strategy has been successfully employed for more than a decade in the management of sepsis.17 The 3-hour sepsis bundle recommendation includes: the early measurement of lactate levels; obtaining blood samples for culture prior to antibiotics; administration of broad-spectrum antibiotics and intravenous fluids (30 mL/kg crystalloids for hypotension or when lactate levels are ≥4 mmol/L).18 19 These early interventions are the most important ones to be performed because they reduce mortality as well as the length of hospital stay and its related costs.20–22 Even though they are relatively simple interventions, sepsis constitutes a major public healthcare problem in Brazil. A nationwide epidemiological study on the incidence, prevalence and in-hospital patient mortality due to sepsis in 227 Brazilian ICUs reported an incidence rate of 290 cases of sepsis per 100 000 habitants (420 000 cases per year for the entire Brazilian population) and a mortality rate of 55.7% (230 000 in-hospital deaths).1
Background
Quality improvement initiatives became more frequent in the last decades of the twentieth century23–26 and it was not different in Brazil, despite still being restricted to the biggest medical centres. In 1999, a survey applied to 159 hospitals of the state of São Paulo27 28 revealed that only 23% of the answering institutions had current quality improvement initiatives (most often restricted to measuring quality indicators).28 More recently, in 2018, a study released by a non-governmental organisation in Brazil reported that six patients per hour die due to severe or catastrophic adverse events of several causes in Brazilian public hospitals.29
In 2004, a large epidemiological study in Brazil showed that the mortality rate of patients with septic shock exceeded 50%; this rate is two to three times higher than the rates observed in other parts of the world.30 Subsequently to this landmark study, a group of researchers leaded by Dr Eliezer Silva founded the Latin American Sepsis Institute (LASI), in São Paulo/Brazil in July 2004. The group followed an international joint initiative headed by medical societies and scientists of different countries, whose aim was to publish international guidelines for management of this condition, and importantly inform support hospitals and patients on how to recognise and treat sepsis. Over the years, LASI focused on studies of the sepsis burden in Brazil, on countrywide training of physicians and nurses, on sepsis diagnosis and management, and performing and fostering research on strategies to reduce sepsis mortality.31
Rationale
Sepsis is a complex medical condition. The diagnosis is based on a group of clinical and laboratorial features and the treatment has to be started early relying on several interventions. Sepsis is still a relevant cause of hospital mortality in Brazil. Sepsis Management Guidelines exist since 2004 but their implementation depends on several coordinated procedures by a team of trained healthcare professionals to facilitate early diagnosis and provide timely treatment. The Institute for Healthcare Improvement (IHI) model for improvement is practical, inexpensive and adequate to accelerate improvements in healthcare institutions. We present here the results obtained with the use of the IHI model to implement a managed sepsis protocol (MSP) in a public hospital in São Paulo, Brazil. We consider that our experience in this area is of interest and can be transferred to other hospitals in low-income to medium-income countries.
Specific aim and methodological approach
A longitudinal prospective study was carried out with the aim of changing procedures and translating ideas into actions. The method of PDSA (Plan-Do-Study-Action) cycles was adopted. An MSP was developed and implemented over an 18-month period (from 1 January 2016 to 30 June 2017), based on actions, new tools, processes and flows proposed by teams comprising healthcare professionals from participant areas including specialists and scientists.32 Factors affecting the implementation process were identified and changed as part of an optimisation process, taking into account benefits and risks. The aim of the project was to keep case fatality/case mortality rates below or equal to 25%, and to ameliorate the compliance rates of the Surviving Sepsis Campaign 3-hour care bundle. Participating healthcare professionals expressed their opinion on the project by answering questionnaires using the Likert Scale.
Our main interest was to quantify three parameters of the IHI model: (1) Sepsis and septic shock case fatality rates (outcome measurements). (2) Compliance rates to the Surviving Sepsis Campaign 3-hour care bundles (process measurements). (3) Rates of satisfaction of the professionals during the process of implantation of the MSP (balancing measurements).32
In order to measure the impact of the MSP (based on the above-mentioned study variables), a prospective audit of 600 clinical records of adult patients (>18 years) admitted to the Hospital Municipal da Vila Santa Catarina with suspected sepsis and/or septic shock was carried out32 for 15 months (1 January 2016 to 31 March 2017).32 All patients were followed up until hospital discharge.
The project was structured to be carried out in four phases corresponding to diverse hospital sectors as follows: (1) ICU department. (2) Adult wards (oncology, transplantation, surgical medical clinic and maternity). (3) Emergency Obstetric Unit. (4) Emergency Unit (part of the Municipal Health Department).32 The fourth phase, developed in the Emergency Unit started in 1 July 2017 and ended 30 November 2017. The sequence was defined based on the expected level of difficulty and potential barriers estimated in each area (‘easier first’).
Baseline measurement
Before the study, the Hospital Municipal da Vila Santa Catarina did not have established sepsis quality indicators. Therefore, the first 6 months of the study were considered as the baseline.
Sepsis mortality (case fatality rate) was highly variable in the first 5 months, ranging from 15% to 35%. During the first 3 months, the baseline observed time intervals were: 45–90 min until haemoculture collection; below 60 min till blood collection for lactate; 30–60 min until starting antibiotics; 60–120 min till start of fluid replacement. The general compliance with the 3-hour sepsis management bundle was about 30%–40%.
Strategy
Four multidisciplinary work teams (MWTs) were organised among scientists, team leaders, technical support persons and front-line staff. Each of these teams was designated to act on a particular study phase. Work meetings of MWT participants were scheduled weekly in order to develop driver diagrams and plan the PDSA cycles.
Each MWT was responsible for creating a driver diagram to guide interventions and improvement actions for its specific area.32 Each one of these interventions was tested in small trials (PDSA cycles) with staff members (nurses and medical doctors) and patients, or during simulations so as to evaluate their impact on the current system. The PDSA results were discussed by the pertinent MWT members who identified successful interventions and adapted those not working well, always aiming for the best care of patients with sepsis. Each PDSA cycle lasted from 4–6 hours to 1 day. PDSA cycles were performed by MWTs and were grouped as follows:
PDSA cycles group 1 (observational/initial tools)
A series of cycles was initially dedicated to map the processes and flows for sepsis management before implementing MSP to identify the main instances requiring improvements in the ICU setting. It was found that time between drawing blood samples and receiving confirmatory lab results of sepsis-related organic dysfunction (for instance, arterial serum lactate and creatinine) was a major obstacle. The following tools were proposed by ICU sepsis MWTs during this set of PDSA cycles: (1) ‘Suspected Sepsis Stamp’ (based on prespecified alterations of vital signs present in patients with suspected or confirmed infection, the attending nurse should trigger a sepsis alarm so that an evaluation by a medical doctor should take place in 5 min time to verify the suspicion and immediately order sepsis diagnostic blood tests). (2) ‘Lab Stamp’ (a blood sample order carrying this stamp means priority in handling and reporting; the arterial serum lactate result should be available in less than 30 min while other tests should be reported before 1 hour).32 (3) Sepsis training programmes for nurses, offered during shifts, focusing on sepsis identification, and based on real cases together with role-playing elements.
PDSA cycles group 2 (early warning system)
This series of PDSA cycles aim to identify instances or situations suspected of early sepsis and is mainly focused on ward inpatients. The existing identified problems were: (1) Poor communication. (2) High variability in clinical practice standards. (3) Lack of familiarity with sepsis management guidelines (elements of the 3-hour care bundle).32
PDSA cycles group 3 (sepsis standard order set)
This series focused on sepsis treatment. The aim was to ensure correct sepsis treatment at the right time to the patient. Accurate sepsis treatment included early intravenous fluid administration (minimum 30 ml/kg in the first 3 hours) and antibiotic administration within 1 hour after sepsis diagnosis. The MWT sepsis-ICU together with the local infection control department designed a standard order set for sepsis32 to be followed by ICU physicians and clinicians to increase compliance with the MSP. This standard order set comprised all the recommended sepsis management interventions such as lab and imaging tests to be ordered, a guide for use of antibiotics and crystalloid fluids, as well as vasoactive drugs to treat septic shock. The directives were very quickly adopted by local physicians and nurses. Lab kits were proposed to make it easier and quicker ordering lab tests in the early phase of sepsis, and they were made available at ICUs and wards.
PDSA cycles group 4 (standardised flows)
The research group was aware that improving sepsis management in the internal medicine or surgical wards would be more difficult than in the ICU. This was because of the higher number of patients and proportionally less attending staff together with the lack of familiarity with critical illness. This group of PDSA cycles aimed first to share and implement the successful changes already established for the ICU phase and, thereafter, to test specific adaptations as locally needed. The fact to be noted is that ward-sepsis MWTs argued that implementation of the ‘suspected sepsis stamp’ would not work well in the wards. The reason is that wards are mainly staffed by nurse technicians (shorter technical training) supervised by one or few university-graduated nurses. This setting is common in Brazilian hospitals; nurse technicians are responsible for less complex interventions such as peripheral vein puncture, drug administration and patient hygiene. For these reasons it was deemed that they would have difficulties identifying abnormal vital signs promptly. To face the problem, forms for vital signs were revised. New forms were proposed in which colours were used to identify normal (green) and abnormal (red) values. It was established that at least two altered vital signs (appearing in red) at two consecutive times were to be an independent criterion to call for rapid team evaluation within 5 min.32 Additionally a system of designated Sepsis Champions was introduced and a video with specific alerts and instructions was created to be given at hospital discharge of high-risk patients (immunocompromised patients, transplant recipients).
A communication plan was developed to divulge the programme within the hospital. That included written texts on MSP that were posted at the hospital’s intranet system and publication of the new procedures in the institutional newspaper. In addition, posters with information on the notification system were fastened in the different ward areas.
Activities developed in the Emergency Obstetric Unit (started on 1 December 2016 and finished on 30 June 2017) did not include any PDSA cycle but only implementation of the previously developed tools and training activities.32
PDSA cycles group 5 (early referral of patients with sepsis)
The last series of PDSA cycles was performed at the Emergency Unit of the Municipal Health Department. A research team, with the support and participation of the ICU MWT, established a partnership with the neighbouring Emergency Unit to establish a local MWT there. The main problems identified were the lack of a system to promptly identify and treat patients with sepsis as emergencies, ‘urgent’ lab tests yielding results only 6 hours later, and highly variable medical care and nursing care quality. A formal partnership was agreed upon between the Municipal Health Department and the Hospital Municipal da Vila Santa Catarina. Consequently, the latter provided diagnostic kits and performed lab tests for patients admitted to the Municipal Emergency Unit. This was accompanied by educational initiatives and process changes that were discussed and implemented.
Additional information about the PDSA cycles performed can be found in the following table 1.
Learning Cycle (PDSA) to improve the management process of septic patients
Patient and public involvement
Patients were not recruited, nor were they directly involved, in the study or in the interventions. All information regarding patients was obtained from the electronic medical records and all collected data were kept confidential.
Analyses
We analysed the outcomes and process variables of the IHI model by the statistical process control method, with P-charts or moving ranges (I-MR) charts, when appropriate, to monitor trend and stability over time. Minitab V.18 statistics software was used in the analyses.
Charts exhibit three lines parallel to the axis of the abscissa. The centre line on each chart represents the general proportion/mean, while the parallel lines represent the upper and lower control limits defined as ±3 SD of the centre line value (establishing if the processes are under control or not). The SD was used for measuring the overall variability of each process and to calculate the centre line and the upper and lower control limits. Normality and correlation tests were not necessary in any of the charts, since less than two points (2%) were outside the control limits in relation to the general mean or average range.
All observations were made on a patient-by-patient basis, during 15 months. P-charts were used for case fatality rates (proportion of non-conforming units). For process variables (time for blood sample for cultures and lactate measurement; antibiotic and fluids administration) I-MR charts were used (continuous data). Two types of I-MR charts were used, allowing monitoring of mean and variation (mobile amplitude).
Descriptive analyses were provided for the balancing measures and were expressed as absolute numbers and percentages.
Ethical considerations
The Research Ethics Committees of the Hospital Israelita Albert Einstein and the Municipal Health Department waived the requirement of informed consent for patients. Informed consent was obtained from healthcare professionals who answered the satisfaction questionnaire.
The present study was a focal quality improvement project with no potential harms to patients.
Results
Of the 6891 patients >18 years old admitted during the study period, 416 fulfilled sepsis criteria and were included in the analysis.
Fatality rates (shown as P-charts in figure 1) were highly variable in the first 6 months and thereafter tended towards stabilisation at a lower level. All points were always within the statistical limits and below (approximately 15.9%) the prespecified goal of 25%.
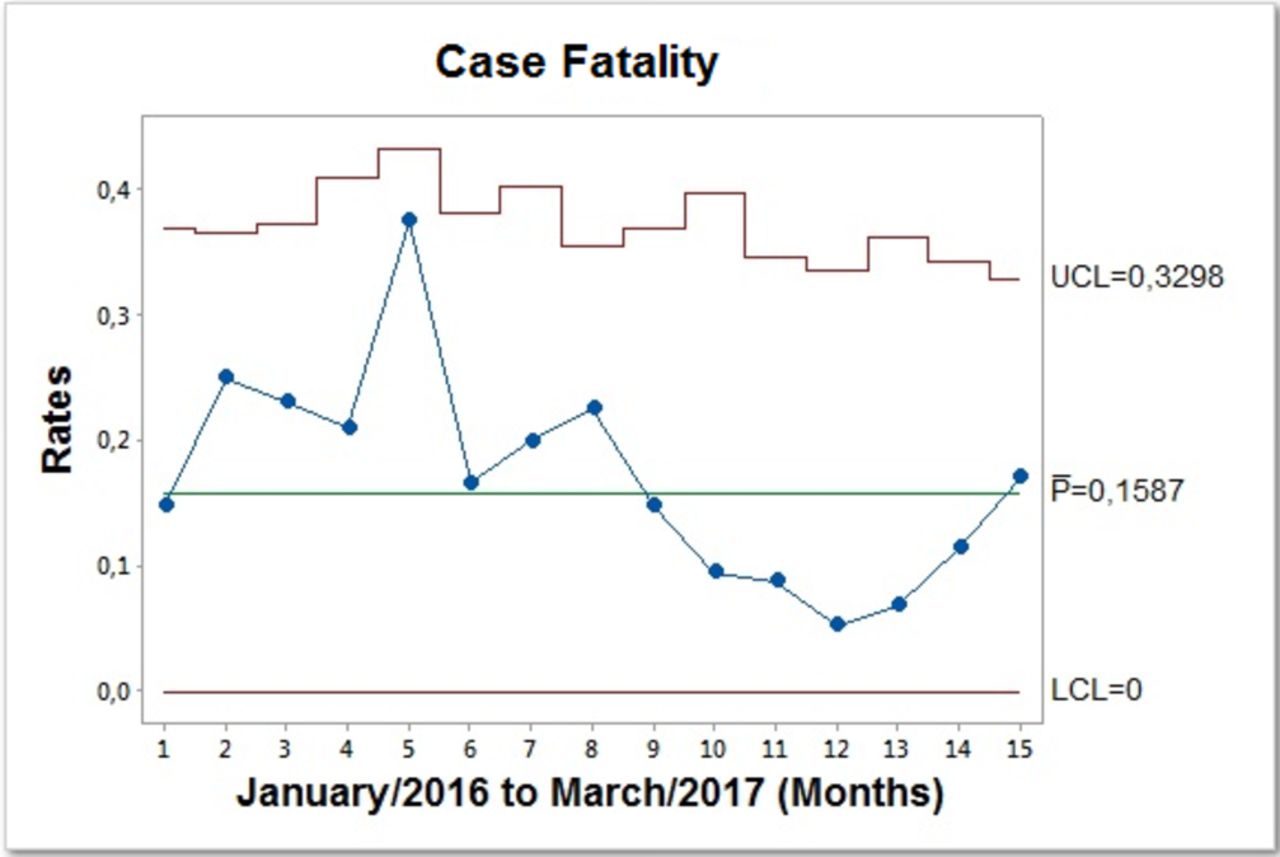
Sepsis case fatality rates. Weekly measurements. Individual values calculated by the total monthly number of patients with sepsis who died divided by the total number of patient with sepsis identified, multiplied by 100. LC, center line; LCL, upper control limit; UCL, lower control limit.
The interval for blood culture collection prior to antibiotic administration varied widely in the first 3 months followed by stabilisation later on at lower levels. All time points were always within statistical limits and below the prespecified goal (within the first hour after opening the MSP). The average time was 46 min 01 s with a variation of 21 min 46 s.
The interval to the first lactate quantitation did not significantly changed over time (data not shown). All time points were below the prespecified goal (within the first hour after opening of the MSP). The average time was 46 min 58 s with a variation of 29 min 05 s.
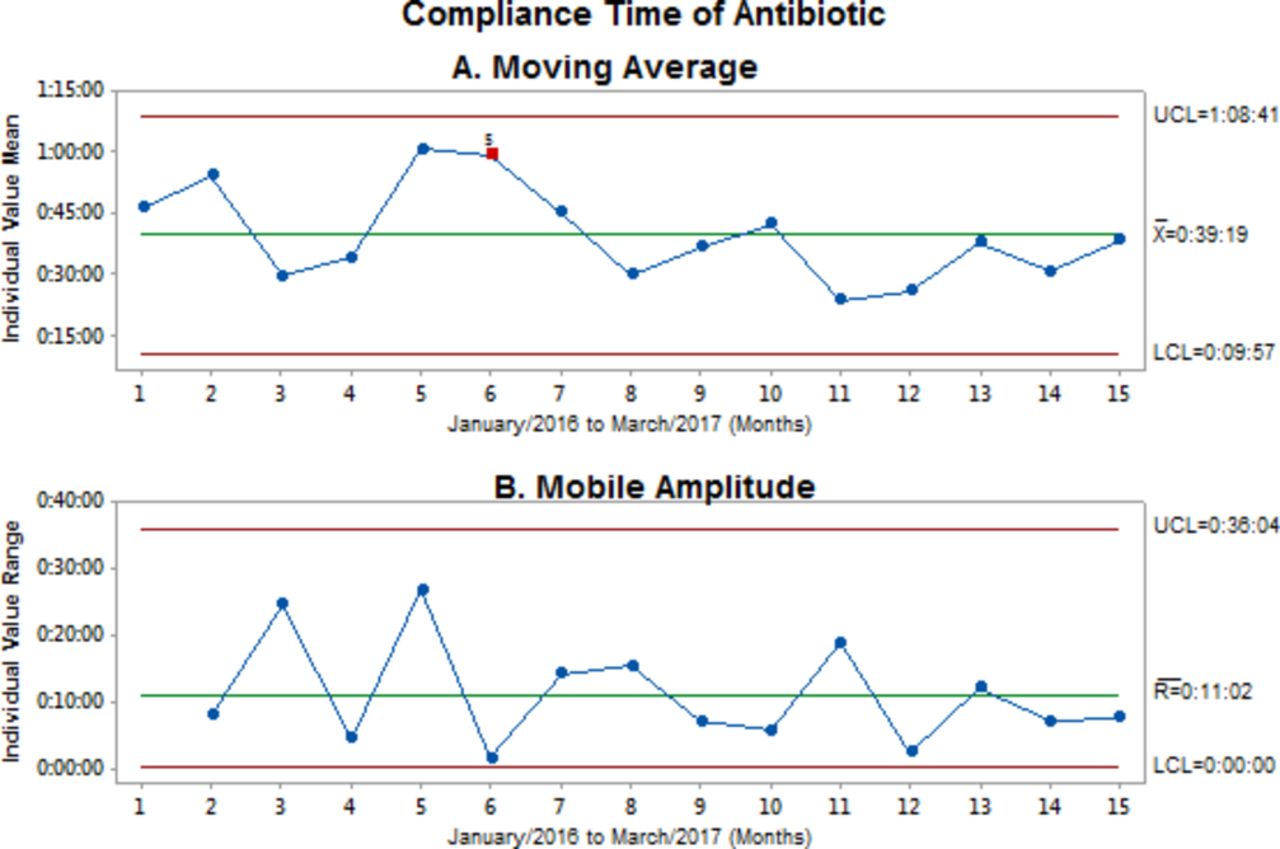
The interval to antibiotic administration is shown in figure 2A. It was highly variable during the first 6 months, and the marked variation observed between points 5 and 6 (figure 2A) possibly reflected an unidentified extraneous cause. Thereafter the tendency was towards stabilisation at a lower level. All time points were within the statistical limits and below the prespecified interval goal (within the first hour after opening the MSP). The average time was 39 min 19 s (figure 2A) with a variation of 11 min 02 s (figure 2B).
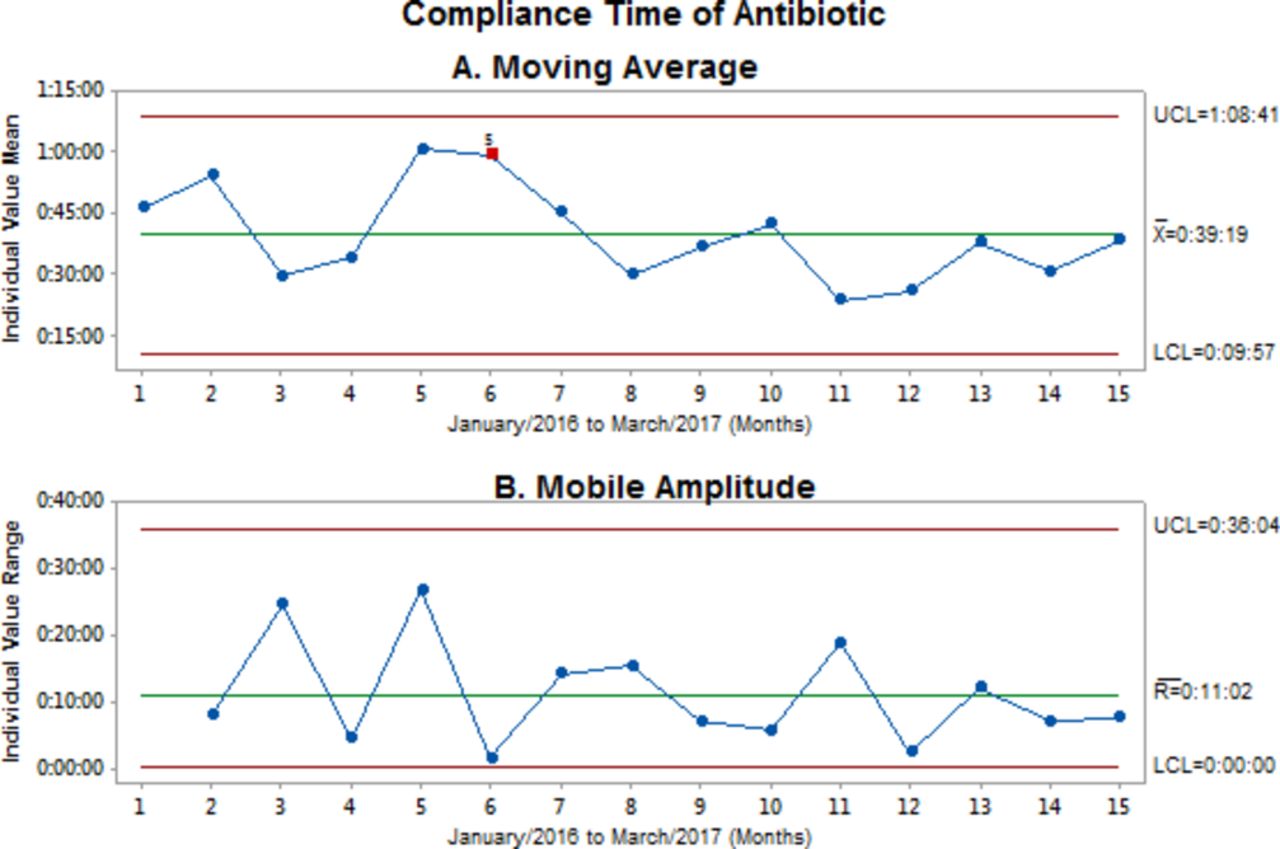
Compliance with time to antibiotics administration. Weekly measurements. (A) Moving average: plotted points on the I chart are the individual observations. LC on this chart is an estimate of the process average. (B) Mobile amplitude: plotted points on the MR chart are the moving ranges (absolute value of the difference between two or more consecutive points). LC on this chart is the average of all moving ranges. The distribution of the mean values of each subgroup was considered normal according to the Shapiro-Wilk test with a value of p<0.05. LC, center line; LCL, upper control limit; UCL, lower control limit.
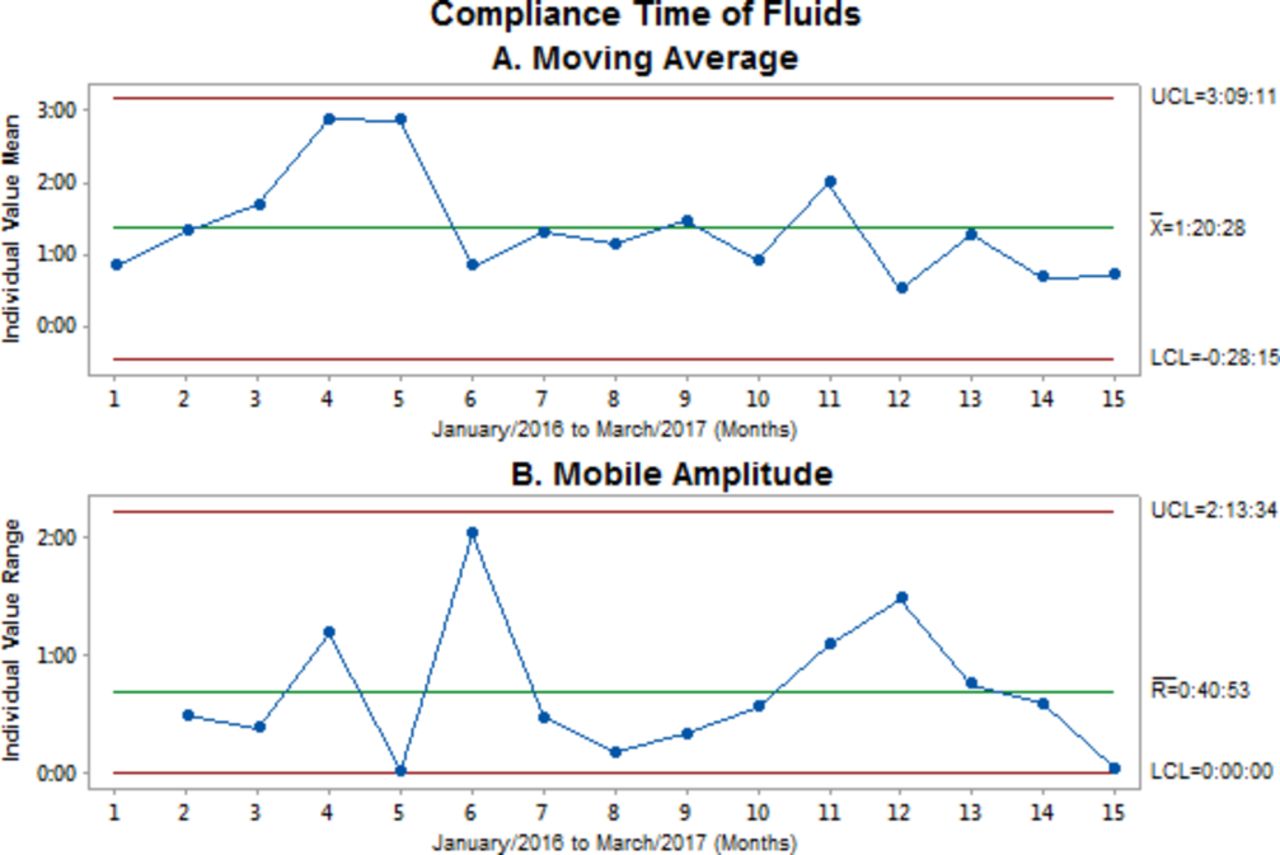
Fluid administration intervals are shown in figure 3. During the first 6 months there was wide variation tending to augment; subsequently, there was stabilisation at a lower level. All time points were within the statistical limits and below the prespecified interval goal (within 3 hours after opening of the MSP). The average time was 01 hour 20 min (figure 3A) with a variation of 40 min 53 s (figure 3B).

{kind=link}
{kind=link}
{kind=link}
Compliance with time to fluid administration. Weekly measurements. (A) Moving average: plotted points on the I chart are the individual observations. LC on this chart is an estimate of the process average. (B) Mobile amplitude: plotted points on the MR chart are the moving ranges (absolute value of the difference between two or more consecutive points). LC on this chart is the average of all moving ranges. The distribution of the mean values of each subgroup was considered normal according to the Shapiro-Wilk test with a value of p<0.05. LC, center line; LCL, upper control limit; UCL, lower control limit.
Altogether, the compliance rates with the 3-hour care bundle were about 38.94%.
The healthcare staff opinions relative to the IHI strategy model were recorded by an anonymous survey questionnaire applied at the end of the study period. Forty-three employees responded. Of these, 22 (71%) disagreed with the following statement ‘the use of the IHI model as a strategy to implant MSP increased my workload’. Forty employees out of 43 (95.2%) answered as ‘being satisfied with the use of the IHI model’.
Interpretation
An MSP implemented using the IHI model methodology achieved the goal of maintaining sepsis and septic shock case fatality rates below 25%. Marked variation in fatality rates was observed at the beginning of the study (January to June 2016); those rates tended to reduce during the last months.
In addition, we also observed that the following process measurements: intervals to haemocultures, serum lactate quantitation, antibiotics and fluid administration, were not significantly modified. In the process of antibiotic administration, there were intermediate deviations, possibly due to random or inherent variation (‘common cause variation’). They were interpreted as have been caused by insufficient training and practice of the new MSP and/or recently hired health professionals.
It is noteworthy that both the outcome and the process variables presented a large variability in the first 6 months of the study with subsequent homogenisation, probably resulting from the intervention, that was followed by stabilisation after an initial period of adaptation.
Finally, the statistical control process showed that the nature of our data was dynamic (iterative and cyclical over time). The absence of previous performance data before MSP implementation may have hindered the observation of more significant effects on the analysed variables.
Discussion
Using the IHI model to implement an MSP was feasible and achieved the goal of keeping fatality rates below a prespecified rate of 25%.
We found that a set of changes implemented over a relatively short period (15 months) permitted the functional evaluation of a complex care process such as sepsis management. In addition, full involvement of local staff in designating MWTs and in the planning/carrying out the interventions was an essential step of the process studied.
In Brazil, epidemiological studies on sepsis are scarce, but multicentric and observational cohort studies, such as those performed by Silva et al in 2004,30 showed sepsis mortality rates due to sepsis, severe sepsis and septic shock in public hospitals reach 52.2%. Other investigations such as SEPSE Brazil33 and COSTS34 show similar case fatality rates at 46.6%, and the PROGRESS Study35 reported rates as high as 56% for Brazilian ICUs. Still another study carried out in 2003–2004 in the southern region of Brazil, showed mortality rates of 66.5%.36 Pereira et al (2008) reported hospital mortality of 36.4%.37 Koenig et al (2010) reported 32.2% mortality rate for private hospitals in comparison to 41% in public hospitals.38 The more recent SPREAD 2017 study informs that mortality rates remain equally high for both types of institutions, being 56% for the former and 55.7% for the latter.1 Similar rates up to 58.9% were reported by Machado et al (2017) for 226 public institutions studied.39
Regarding the levels of compliance, we obtained a compliance rate close to 39% for the 3-hour care bundle among 162 patients out of the 334 who opened the MSP (n=416) (online supplementary file) reflecting the effective adherence of the healthcare staff of Hospital Municipal da Vila Santa Catarina. This was a very good result in comparison to the compliances reported for the 6-hour and 24-hour care bundles by Camelier et al (2008)—23.3% and 21%, respectively,40—and by Pacheco Martins etal (2014)—10% and 13%, respectively.40 Recently a nationwide study in 46 public hospitals showed compliance of 12% with the 3-hour care bundle; and still less at 5.7% with the 6-hour care bundle.39 Finally, the SPREAD Study reported compliance rates of 20% for the 6-hour care bundle.1 We ascribe our good results in compliance to the IHI model that, since the beginning, proposes the participation and commitment of all healthcare personnel and also of the administrative instances.
Supplemental material
Our study was able to observe the maintenance of relatively low case fatality rates (15.9%) which is comparable to those reported in many international studies.17 20–22
Lessons and limitations
The most important lesson is neither original nor new, in that success of improvement projects requires continuous support from the leadership (administrative and clinical), and motivated people at the front line, boosted by trained champions responsible for multiplying the required actions and spreading information. Another lesson relates to the know-how and familiarity with the IHI model acquired by the teams (MWTs). The hospital staff benefited from learning about the model and its elements, as the PDSA cycles that can be further applied to other protocols and other quality improvement projects.
Likewise, we have learnt that after achieving our goal, MWT groups and the processes created by them must be continually maintained and improved by the leaders. Sustainability is crucial and it was not assessed by the present study protocol. There is a risk that the implemented procedures would not persist after the end of the project.
In addition, it is important to acknowledge that the present study has the following important limitations: it is a single-centre experience with a non-randomised design; a true baseline is lacking (because it was carried out in a recently opened hospital), and the data were manually acquired from multiple databases in a limited period.
Conclusion
We conclude that the IHI model was useful and feasible as a strategy to implement an MSP, and to maintain case fatality rates within an established target that is below the reported nationwide rates.
The use of the IHI model provided a multifaceted approach to the treatment of sepsis and septic shock, allowing relatively high and stable compliance rates, and raising awareness among health professionals, in an easy, fast, effective, safe, timely and equitable manner. These aspects may be particularly relevant to institutions with limited resources.
Acknowledgments
The authors thank the professionals at the departments of Hospital Municipal da Vila Santa Catarina involved in the project and their contribution to the development of this study. The authors also thank Professor Ises de Almeida Abrahamsohn (MD, PhD) for her assistance in editing and revising the manuscript.
References
Footnotes
Collaborators We would like to acknowledge the sepsis multidisciplinary work teams: Guilherme de Paula Pinto Schettino, MD, PhD (Medical director); Ana Paula Metran Nascente Pereira, MD, PhD (ICU Department); Adolfo Wenjaw Liao, MD, PhD (Obstetrics Department); Midgley Gonzales, MD, PhD (Obstetrics Department); Monica Andrade de Carvalho, MD, MSc, MBA (ICU Department); Rosana Mandelbaum, MD (Clinician, Rapid Response Team); Fernanda Domingos Giglio Petreche, MD (Clinician, Rapid Response Team); Cristina Tiemi Amadatsu, MD (Obstetrics Department); Carolina Devite Bittante, MD (Infection Control); Leonardo Jose Rolim Ferraz, MD (Medical Manager); Carlos Alberto Eduardo Gomes, MD (Medical Manager Municipal Emergency Unit) ; Rodrigo Vone Fregoneze, MD (Medical Coordinator Municipal Emergency Unit); Rodrigo NG Taniguchi MD (Municipal Emergency Unit Attending Physician); Gabriela Sato, MBA (Hospital Manager); Marcia Galluci Pinter, MSc (Surgical Unit Coordinator); Adriana Martins da Silva, MBA (Wards Coordinator); Maitê Augusta C. C. Rossetto (Quality Coordinator); Eliton Paulo Leite Lourenco, MBA (Head of ICU Nurses); Samira Scalso de Almeida (Imaging Department); Silvana Aparecida Eleodoro dos Santos (Obstetric Coordinator); Marcelo Longarezi Valvassora, MSc (Transplant Department Nurse); Maria Aparecida Machado (Oncology Nurse); Caroline Gusmão Alves Santos (Wards Nurse); Camila de Carvalho Gambin (ICU Nurse); Natalia Nunez de Souza (ICU Nurse); Priscilla Santini Ramalho (Wards Nurse); Érika Brosco Lima (Obstetric Department Nurse); Maria Caroline de Oliveira (Obstetric Department Nurse); Andreza Moreira Santana (Emergency Nurse); Andreza Michele Secolo (Emergency Nurse); Denise Simas Lamarão, MBA (Pharmacist); Francisco Neves Pereira (Lab Coordinator); Ana Paula Doria Santos (Emergency Nurse); Claudia Regina Basilio Foglietto (Emergency Nurse); Priscila Reimão de Melo Fortunato (Wards Nurse); Ernane Cruz da Silva (Medical Records Department); and Ana Paula de Oliveira Ribeiro (Medical Records Department).
Contributors ES and AJP conceived the study. All authors and coauthors contributed to the planning. LKCN and AJP led the MWTs in producing the study tools. LKCN carried out the PDSA cycles. LKCN and AC were responsible for the results and analysis, and LKCN was responsible for its submission. All authors have participated in writing, revising, correcting and editing the manuscript.
Funding LKCN was funded by a master's studentship from the Brazilian Ministry of Education (CAPES). The study was conducted in partnership with the Brazilian Ministry of Health through the Institutional Development Program of the Unified Health System (PROADI - SUS), and classified as one of the objectives of the National Health Plan, highlighting the relevance and potential contribution of the project to the governance of the SUS, according to the ordinance 3.362, 12/8/2017.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Research Ethics Committees of the Hospital Israelita Albert Einstein and the Municipal Health Department approved this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available. All data relevant to the study are included in the article or uploaded as supplementary information. We can only share data without the identification of audited patients, only tables.