Article Text

Abstract
Objective Chronic low back pain is very common and often treated with epidural steroid injections (ESIs). As ESI referrals had been rapidly increasing at our Veterans’ Administration hospital, we were concerned that they were supplanting more comprehensive care. The objective was to determine how referral patterns and multidisciplinary care might change with the implementation of evidence-based guidelines.
Methods In this retrospective observational study, multidisciplinary evidence-based guidelines were implemented in 2014 (EAGER: Esi Appropriateness GuidElines pRotocol) as part of the ordering process for an ESI. Time series analysis was performed to assess the primary outcome of subspecialty referral pattern, that is, the number of patients receiving referrals to ancillary services which might serve to provide a more comprehensive approach to their back pain. Secondary outcomes included patient-level changes (ie, body mass index, number of injections, opioid use), which were compared before and after protocol implementation.
Results Comparing preimplementation and postimplementation protocol periods, referrals to physical medicine/rehabilitation increased 11.7% (p=0.003) per year and integrative health increased 2.1% (p<0.001) per year among the 2294 individual patients who received ESI through the neurointerventional radiology service. Of 100 randomly selected patients for patient-level analysis, the median body mass index decreased from 31.57 to 30.22 (p=<0.001) and the mean number of injections decreased from 1.76 to 0.73 (p<0.001). The percentage of patients using oral opioid analgesics decreased from 72% to 49% (p=<0.001).
Conclusion Implementation of evidence-based guidelines for ESI referral helps guide patients into a more comprehensive care pathway for chronic low back pain and is correlated with patient-level changes such as decreased body mass index and decreased opioid usage.
- epidural steroid injections
- evidence-based medicine
- chronic low back pain
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Low back pain (LBP) is the most common pain symptom experienced by American adults and the second most common reason for primary care physician visits.1 LBP is a significant socioeconomic problem, estimated to cost $30 billion in direct healthcare expenditures and $100–$200 billion in decreased wages and disability in the USA annually.2 As the population ages, LBP prevalence has been increasing, with one study showing a 169% rise over 15 years (from 3.9% in 1992 to 10.2% by 2006).3 Multifactorial aetiologies including age-related degeneration and structural pathology, as well as occupational,4 5 lifestyle6 7 and psychological factors,8 potentially contribute to this ubiquitous, often debilitating condition.
The first line of treatment for LBP in patients without ‘red flags’9 is conservative medical management (ie, oral analgesics, physical therapy (PT)). However, when these steps fail to provide relief, epidural steroid injections (ESIs), often a combination of steroid and analgesics, are commonly used to treat LBP when there is pathoanatomical correlate (ie, disc protrusion impinging on nerve root).10 11 In fact, ESIs are the most commonly performed intervention in the USA to manage chronic/subacute LBP.12 13 Although these injections can be useful for short-term management of chronic/subacute LBP, they have not demonstrated a long-term effect on pain or surgical rates.14 15 ESIs are also not without risk. Procedural risks include bleeding, infection and nerve injury, and effects secondary to systemic absorption of injected steroid include suppression of the hypothalamic–pituitary axis resulting in decreased cortisol levels, disruption of glucose levels in patients with diabetes resulting in hyperglycaemia, and decreased bone mineral density over time.16 17
ESIs may often be used as a panacea for LBP, despite data showing that they are most effective for specific structural aetiologies.18–21 As such, a multifaceted multidisciplinary approach should be priority when managing patients with LBP who are being considered for ESIs. This comprehensive health management approach includes PT, behavioural therapy and lifestyle modifications. Several studies have shown benefit from such multidisciplinary approaches to chronic LBP compared with routine conservative treatment and analgesics, including better comparative effects on long-term pain and disability.22–25
Mirroring a general nationwide trend,26 referrals for ESIs to the neurointerventional radiology (NIR) service from primary care providers, and to a lesser degree other subspecialties at our Veterans’ Administration (VA) hospital, had been increasing over the most recent 5–7 years. We noticed more referrals for patients with non-specific LBP and requests for repeat injections, exceeding the recommended frequency of no more than four injections per 12-month period or four consecutive injections in the same region per 18-month period.20 In order to promote more appropriate ESI usage and encourage a multifaceted multidisciplinary approach, we instituted a practice quality improvement initiative by implementing evidence-based appropriateness guidelines for ESI (EAGER: Esi Appropriateness GuidElines pRotocol) in January 2014. The objective was to assess changes to referral patterns to ancillary services with the goal of comprehensive treatment of back pain. Second, we aimed to evaluate patient-level changes. The outcome measure was the change in referral patterns in our NIR practice levels and at the patient level before and after implementation of the EAGER programme.
Materials and methods
Procedural codes were used to identify patients receiving ESIs at our VA hospital between 1 January 2010 and 30 July 2017. Inclusion criteria were adult patients (>18 years of age) who underwent any spinal level of ESI (interlaminar vs transforaminal approach) at the VA and performed by the NIR service during this time period. Patients were excluded if there were no data after implementation of the EAGER protocol.
Patient involvement
Patients were not directly involved in the design of this study.
Implementation of appropriateness guidelines (EAGER)
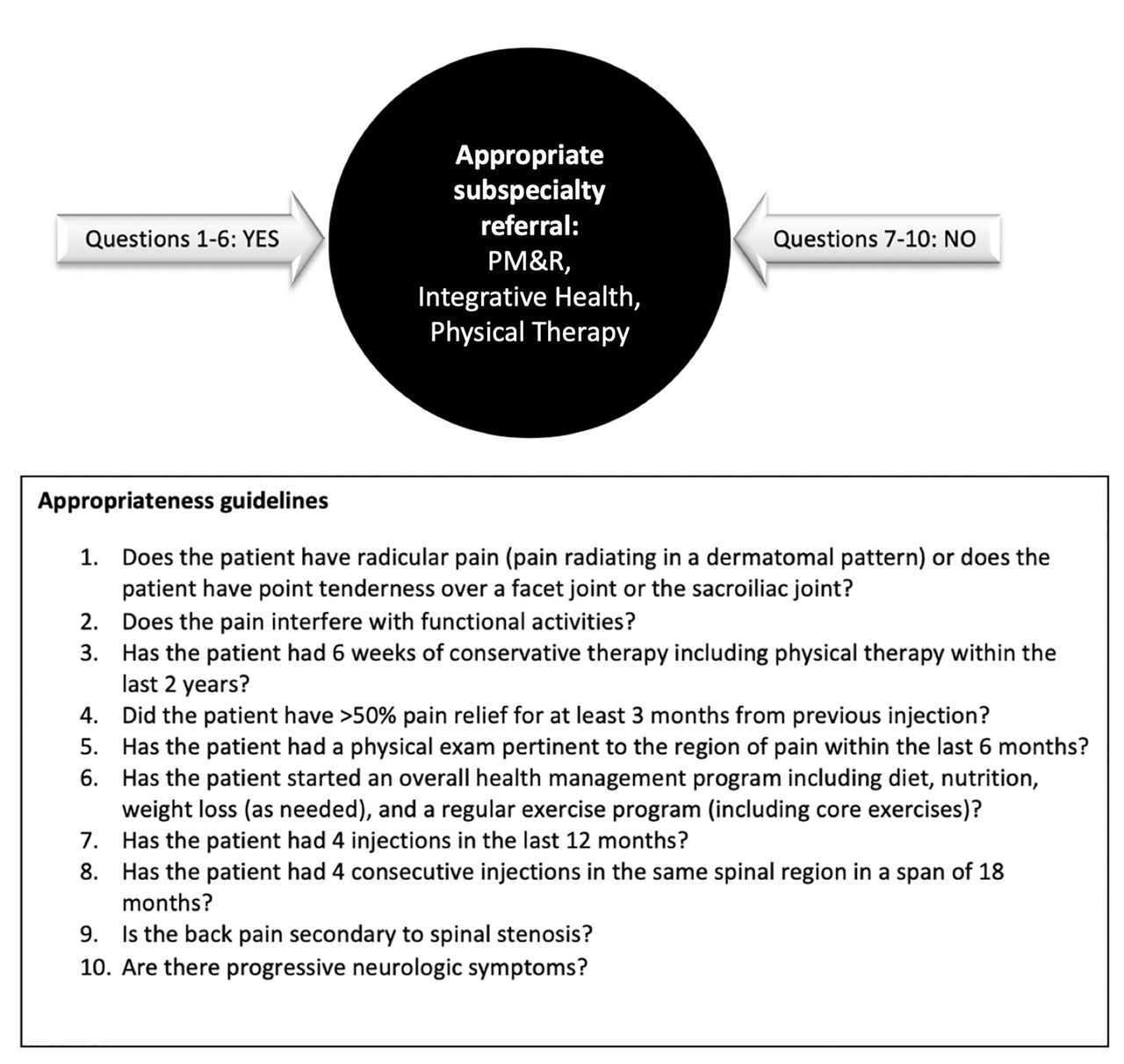
An evidence-based clinical decision support tool (EAGER protocol) was developed based on various systematic and meta-analyses on spine pain injections18–20 and was implemented in January 2014. The EAGER ‘intervention’ required that the clinical provider answer 10 questions as part of the ordering process for an ESI through the NIR service on their patients with back pain (figure 1). These questions were designed to have unambiguous ‘yes’ or ‘no’ answers that a clinician could assess in a few minutes during a routine office visit. An important rationale was to direct patients with a lower likelihood of long-term benefit from ESI, such as those with spinal canal stenosis (questions 1 and 9), a history of limited response to injections (questions 4, 7 and 8) or incomplete utilisation of more conservative interventions (questions 3 and 6), to other methods of management with potentially more and certainly complementary benefit. Patients who met the appropriateness criteria for an ESI were then treated by the NIR team.

The EAGER protocol. Answering ‘no’ to any of questions 1–6 would generate appropriate subspecialty referral (PM&R, pain anaesthesia, integrative health and/or physical therapy) for further evaluation. Answering ‘yes’ to any of questions 7–10 would also generate subspecialty referral. EAGER, Esi Appropriateness GuidElines pRotocol; PM&R, physical medicine and rehabilitation.
The referring providers, majority of whom are in primary care, as well as multispecialty physicians, fellows, residents and mid-level practitioners, were introduced to the EAGER protocol and the accompanying evidence-based rationale prior to implementation through institution-wide email and small group didactic sessions. The interventional group conducted inservice to the supportive staff (radiology nurses, technologists) at the beginning of the study in mid-2014 and provided reinforcement during protocolling at every opportunity. The ordering providers were given 30 min lectures biannually. The NIR support staff (eg, schedulers, nurses) were also briefed on EAGER. Each ESI request and the completed EAGER questions were reviewed by a neurointerventionalist prior to scheduling the procedure.
The PT, physical medicine and rehabilitation (PM&R), and integrative health referral patterns of patients treated by the NIR practice in the 4 years before (2010–2013) and in the 3.5 years after (2014–2017) EAGER implementation were tracked using VA clinic visit codes for the indication of spinal pain. The PT, PM&R and integrative medicine regimens are tailored to the individual patient.
Impact of the EAGER programme
For preliminary assessment of the effect of EAGER implementation at the individual level, we performed a subgroup analysis of 100 randomly selected patients from the NIR practice who had ESIs pre-EAGER and post-EAGER. These 100 random patients were selected due to the impracticality of reviewing every patient’s chart in detail, and the number was statistically robust enough for the purposes of this study. A study sample size of 100 (patient compared with himself) would achieve a power of 80% and a level of significance of 5% (two-sided) for detecting an effect size of 0.4 between pairs. Patient-level electronic medical record (EMR) data were only available dating to 2011, while older data were archived off-site and unavailable. The pre-EAGER period reviewed was 2011–2013 and the post-EAGER period was 2015–2016. The 2014 period was considered the transition period for the clinical providers to incorporate EAGER into their practices and therefore was not included in this subanalysis. The patient’s age at the time of the first ESI was recorded. The number of ESIs received by each patient in the years from 2011 to 2017 was determined from the electronic medical record. The median body mass index (BMI) and the average opioid dosage in the time period before 2014 were considered the baseline and were compared with the same variables after 2014, given the association of chronic LBP with elevated BMI7 and the epidemic of opioid use for chronic pain. The documentation of PT referral before and after EAGER implementation was recorded. The reports from the MRIs temporally close to the last ESI in each time period were reviewed. The MRI features were chosen based on their prevalence in symptomatic adults (eg, moderate/severe canal stenosis, moderate/severe foraminal narrowing, disc protrusion/extrusion, nerve impingement).27 Correlation of the MRI findings with the number of injections was performed.
Statistical analysis
To test for an effect from the EAGER quality improvement intervention, we aggregated the referral data from patients treated by the NIR practice and the hospital-wide referral practice into yearly proportion of the time in which spine procedures were ordered before (2010–2013) and after (2014–2017) the EAGER intervention. We analysed these yearly proportions using interrupted time series analysis.28 The two general approaches to interrupted time series analysis are autoregressive integrated moving average models29 and ordinary least squares models designed to adjust for autocorrelation.30 We used an ordinary least squares model because it offered more flexibility in an interrupted time series context than autoregressive integrated moving average models.31 32 To adjust for autocorrelation, we fit an ordinary least squares model with Newey-West SEs, which assume the error structure to be heteroskedastic and possibly autocorrelated up to some lag.33 After fitting our model, we checked if the number of lags we included in the model to account for autocorrelation was correctly specified, and adjust accordingly using the Cumby-Huizinga general test for autocorrelation.34
In the individual subgroup analysis, for group comparisons, categorical variables were compared using χ2 test or Fisher’s exact test, as appropriate. For continuous variables (pre-EAGER and post-EAGER number of injections, BMI and prescribed opioids), Student’s t-test was used. All data were analysed using two-tailed tests, and a p value of <0.05 was considered significant. Linear regression model was used to obtain the mean number of injections for each of the ‘key’ MRI findings while adjusting for covariates. Statistical analysis was performed using Stata V.15.
Results
NIR patient cohort referral pattern analysis
From January 2010 to July 2017, there were 4470 ESIs on 2294 individual patients through the NIR service. The referral patterns in this patient cohort changed after EAGER implementation as follows (figure 2).

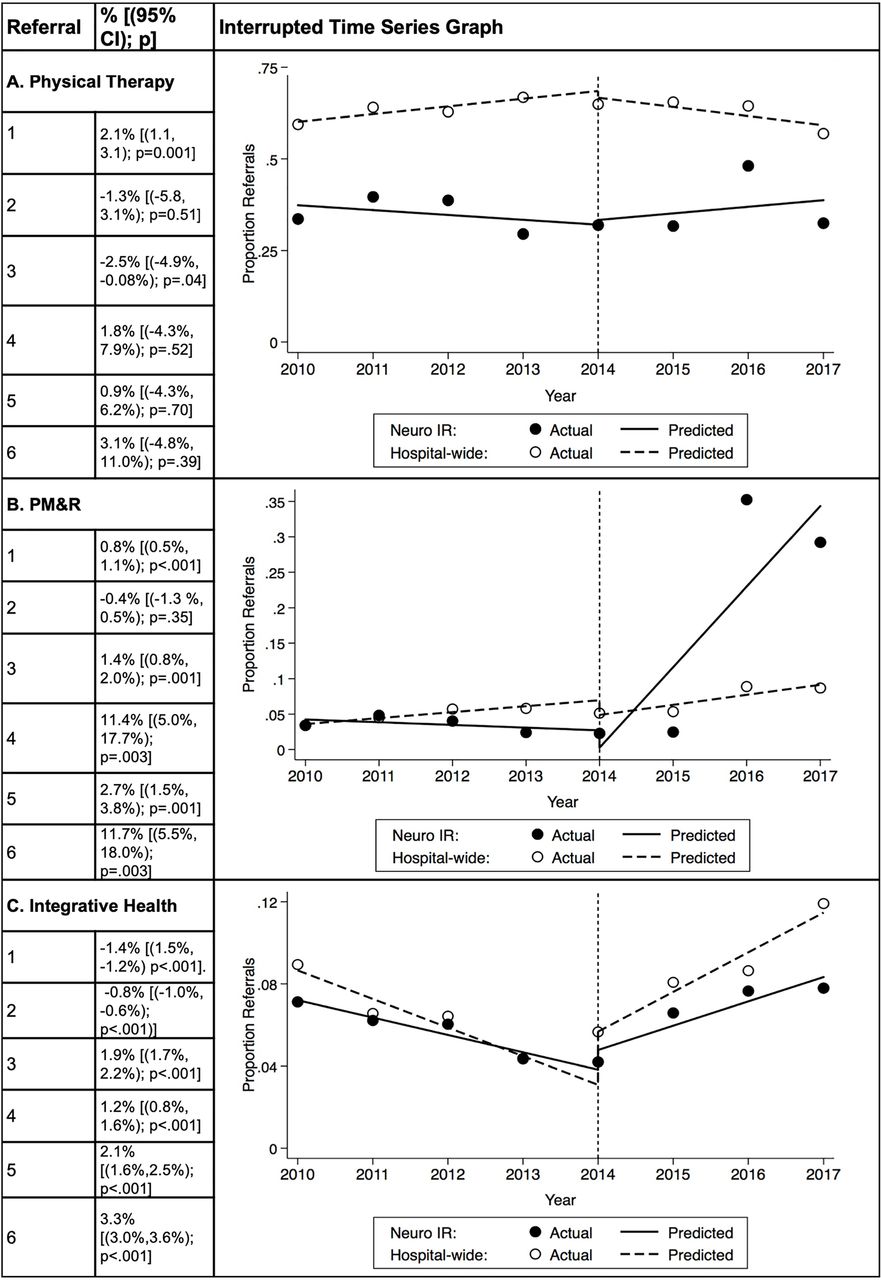
Interrupted time series for referral to (A) physical therapy, (B) PM&R and (C) integrative health. (1) Pre-EAGER referrals per year in the hospital-wide group. (2) Pre-EAGER referrals per year in the NIR group. (3) Post-EAGER referrals per year in the hospital-wide group. (4) Post-EAGER referrals per year in the NIR group. (5) Difference in referrals per year between the pre-EAGER and post-EAGER time periods in the hospital-wide group. (6) Difference in referrals per year between the pre-EAGER and post-EAGER time periods in the NIR group. EAGER, Esi Appropriateness GuidElines pRotocol; IR, interventional radiology; NIR, neurointerventional radiology; PM&R, physical medicine and rehabilitation.
Physical therapy
PT is part of the standard conservative treatment of LBP, before and in conjunction with ESIs. In the 4 years before intervention, the NIR cohort referrals to PT decreased 1.3% (p=0.51) per year. In ~3.5 years after intervention, NIR cohort referrals to PT increased 1.8% (p=0.52). The NIR cohort showed a 3.1% (p=0.39) increase in referral per year to PT compared with the hospital-wide practice post-EAGER implementation as compared with the pre-EAGER time period (figure 2).
Physical medicine and rehabilitation
In complicated cases, referral to PM&R allowed a more comprehensive physical exam, and in some cases the use of non-imaged-guided treatments (eg, trigger point injections). In the 4 years before intervention, NIR cohort referrals to PM&R decreased 0.4% (p=0.35) per year. In ~3.5 years after intervention, NIR cohort referrals to PM&R increased 11.4% (p=0.003). The NIR cohort showed an 11.7% (p=0.003) increase in referrals per year to PM&R post-EAGER implementation compared with the hospital-wide practice (figure 2).
Integrative health
In the 4 years before intervention, the NIR cohort referrals to integrative health decreased 1.4% (p<0.001) per year. In ~3.5 years after intervention, the integrative health referrals increased for the NIR cohort (1.2%, p<0.001). The NIR cohort showed a 2.1% (p<0.001) increase per year in referral to integrative health compared with the hospital-wide practice post-EAGER implementation (figure 2).
Subgroup analysis of individual patients
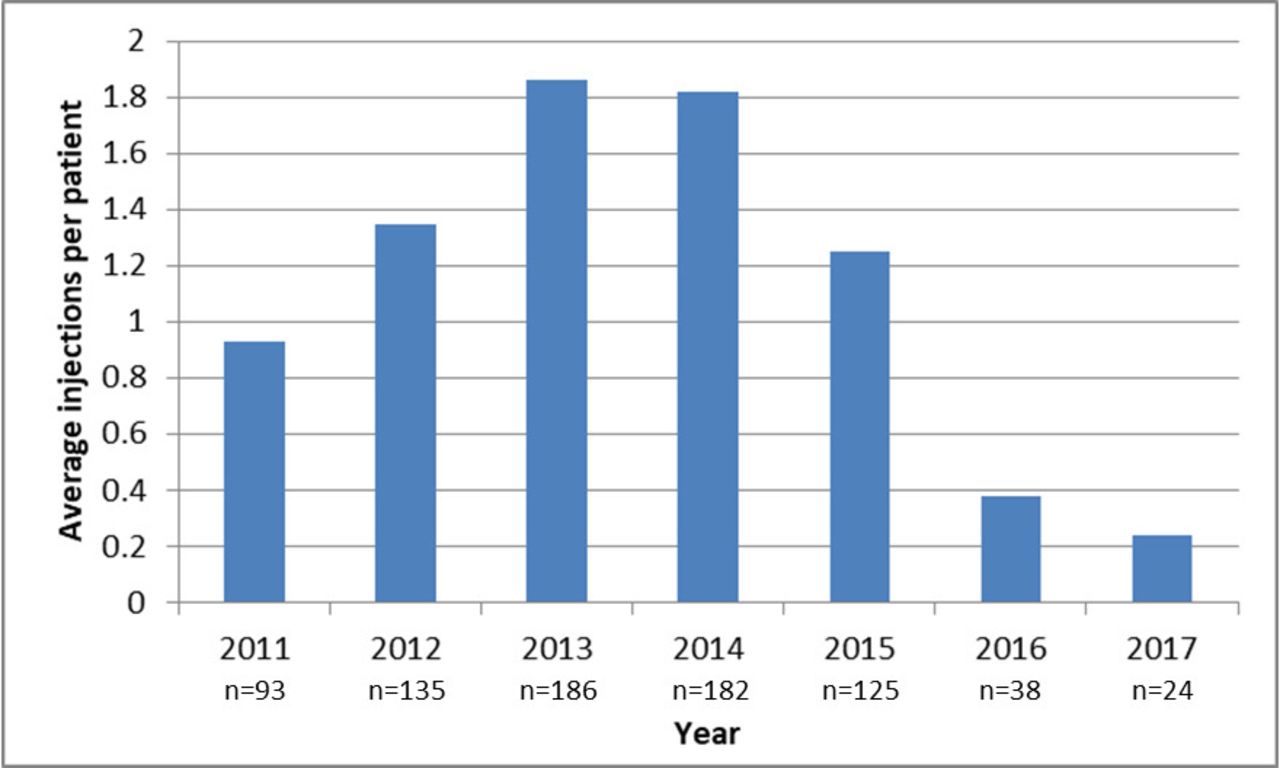
Of the 100 randomly selected patients who underwent ESI by NIR both before and after EAGER implementation, and were therefore presumed to have chronic (>3 months’ duration) LBP, 95 were male with a mean age of 58.9 years (SD±12.4). The mean number of injections pre-EAGER was 1.76 (95% CI 1.48 to 2.05), while post-EAGER was 0.73 (95% CI 0.57 to 0.90) (p<0.001). The number of yearly injections from 2011 to 2013 was trending higher but steadily decreased from 2014 to 2017 (figure 3). The mean BMI decreased from 31.57 (95% CI 30.38 to 32.76) in the pre-EAGER period to 30.22 (95% CI 29.05 to 31.39) (p<0.001) in the post-EAGER period. Seventy-two per cent of the patients in the pre-EAGER period were prescribed opioids as part of their pain control regimen. Non-opioid-only pain control regimens were prescribed in 28% of patients pre-EAGER but increased to 51% of patients in the post-EAGER period (p<0.001). Among the subset of patients still using opioids post-EAGER, 27% decreased their use, 53% did not change and 20% increased their use. Pre-EAGER, 35% of patients underwent PT, while 59% underwent PT post-EAGER (p=0.57).
{kind=link}
{kind=link}
{kind=link}
Average injections per patient by year within the subgroup of 100 randomly selected patients (n=absolute number of injections per year).
Eighty-four patients had MRIs pre-EAGER and 54 patients had MRIs post-EAGER. In the pre-EAGER period, all MRI categories (moderate/severe canal and foraminal stenosis, disc extrusion and nerve impingement) were associated with injections. In the post-EAGER period, foraminal narrowing (moderate, p=0.009; severe, p<0.001), disc extrusion (p=0.02) and nerve impingement (p<0.001) were significantly associated with the number of injections, whereas the presence of moderate/severe canal stenosis was not (table 1).
Association of MRI findings and the number of ESIs
Discussion
In this study, we developed and implemented evidence-based appropriateness guidelines for ESIs and determined the effects on referral patterns after implementation. In this observational practice quality improvement study, we found that incorporating such a decision support tool for providers as part of the ordering process for ESIs promoted appropriate first-line conservative therapy for chronic/subacute LBP prior to ESI and encouraged comprehensive evaluation that affected referral patterns. By evaluating referral patterns in the cohort of patients treated by NIR during that time period, we showed an increase in multidisciplinary referral for the management of LBP in the post-EAGER period. The NIR cohort showed significant increase in referrals to PM&R (11.7%, p=0.003) per year post-EAGER implementation compared with the hospital-wide practice, and significant increase in referrals to integrative health (2.1%, p<0.001) per year compared with the hospital-wide practice post-EAGER implementation. The PT referrals showed a 3.1% (p=0.39) increase per year to PT compared with the hospital-wide practice post-EAGER implementation as compared with the pre-EAGER time period. The lack of statistical significance may reflect that there may have been previous PT referrals. As well, many of the patients may have undergone outside network PT closer to home, which might not be readily apparent in the EMR.
Importantly, at the individual patient level, there was a decrease in mean BMI and in mean opioid use post-EAGER as compared with pre-EAGER. The mean PT referrals post-EAGER also increased, which was interpreted as increased improvement in the overall conservative management. The increasing number of injections in the 3 pre-EAGER years and the decrease in the number of injections post-EAGER illustrate the effects of EAGER, without the confounding effects of ESIs or symptomatic improvement over time. Pre-EAGER, all MRI categories were associated with injections. However, post-EAGER, the MRI features that typically result in the radicular symptoms, which the protocol aimed to target, were statistically associated with the number of injections, while spinal stenosis, which has been shown to receive less benefit from ESI than radicular LBP,35 36 was not correlated with the number of injections. Our results demonstrate the effectiveness of using an evidence-based clinical decision support tool to help select patients with LBP who are most likely to benefit from ESI treatment and to foster multidisciplinary care in the chronic LBP population.
We found that EAGER leads to an increase in a multifaceted approach to chronic LBP. Other studies that have shown that such care plans can lead to an increase in patients returning to work,23 improved range of motion, strength and Visual Analogue Scale scores,37 and reduction of disability.38 39 This markedly contrasts with ESI alone, which has not been found to be effective for long-term relief, to affect surgical rates significantly or to reduce opioid usage among patients with chronic LBP.14 While ESIs can be a useful short-term tool in the treatment of radicular pain related to discogenic causes, short-term pain relief has not been found to be a good predictor of long-term outcomes.40 It has also been found to be less effective for axial chronic LBP than radicular pain.41 It is generally acknowledged that patients with shorter duration of symptoms, radicular symptomatology, lesser disease burden and the absence of coexisting psychosocial pathology fare better with therapeutic interventions.42–46 Despite these limitations, ESI has seen a marked increase in prevalence.26
There is no universal definition of multidisciplinary care for LBP. While there is likely significant overlap in care defined as multidisciplinary, some specific interventions may be more useful than others. Those shown to be most effective in chronic LBP include strengthening exercises, aerobic fitness training and behavioural therapy.47 As patient populations may also vary between these studies, the techniques may show diverse degrees of effectiveness.48 A prospective observational study found that a multidisciplinary treatment programme had medium to high effect sizes in ameliorating pain, functional restoration and quality of life in patients with a long history of chronic back pain.49 This study also demonstrated that the impact of sociodemographic and pain-related parameters needs to be taken into account when including patients in an appropriate treatment programme.49 These studies reinforce using evidence-based guidelines to select patients that will most benefit from ESI in the multidisciplinary care setting, as ESI may be the best approach for diagnosis and treatment in some patients but not others. Although some interventional practices get referrals from multidisciplinary groups or specific requests from neurosurgeons or orthopaedic surgeons, we and others receive requests from mid-levels and general practitioners who are not necessarily versed in back pain and spine procedures. Also, as more mid-levels are challenged on the front line of back pain management, protocols such as EAGER need to be implemented.
Our study had several limitations. First, as this is a retrospective analysis of clinically implemented guidelines, we were only able to show correlation between implementation of the evidence-based guidelines and the observed effects, not causation. Although EAGER was implemented by the NIR service in January of 2014, as with any change to a practice, there was only gradual incorporation by referring providers into their practices. As such, the changes in referral patterns immediately after EAGER implementation are difficult to assess. Although we demonstrated that EAGER leads to improved secondary markers of spine health in a subgroup of randomly chosen patients from the NIR practice (ie, decreased opioid use and BMI) and greater utilisation of multidisciplinary care, which other studies have shown to improve outcomes in patients with chronic LBP,25 49 we did not specifically study the clinical effects of the intervention. Second, we were not able to control for several confounding factors that may affect the changes in our patient or provider population. For example, it is difficult to determine how much the increasing awareness of the opioid epidemic, and subsequent institutional initiatives to reduce their use, contributed to decreasing the opioid dosage of the average patient in our study. Importantly, the EAGER protocol helped to bring the increasing national awareness of the opioid crisis50 and studies reassessing the ESIs35 to the local and individual level (provider and patient). Also, although the majority of patients in the VA receive their care within the system, spine-related care outside the VA system was not included in the analysis. Pain outcomes (eg, Visual Analogue Scale) were not consistently recorded in the pre-EAGER period; therefore, an analysis of the effect of EAGER on changes in pain could not be analysed. While there was no age-matched control group with which to compare patient-level changes with EAGER, the patients served as their own controls in this subgroup analysis. Lastly, although we were able to assess changes in the referral rates to the various subspecialty services for the hospital-wide and the NIR practices, the results of EAGER implementation in this predominantly male VA population with chronic/subacute LBP may not be generalisable to every patient with LBP.
Conclusion
An evidence-based EAGER helps guide patients into a better LBP care pathway with multisubspecialty expertise providing a comprehensive approach to LBP management. Implementation of such guidelines also correlates with benefits at the individual patient level, such as decreased BMI, decreased or discontinued opioid usage, and increased PT referral. ESIs are useful, relatively safe interventions for short-term pain management in appropriately selected patients, and with a multidisciplinary, multifaceted approach those patients who will most benefit can be selected for ESI treatment.
Acknowledgments
The authors would like to acknowledge the neurointerventional staff at the George E Wahlen Veterans’ Administration Hospital, Salt Lake City, Utah, USA.
References
Footnotes
Contributors LS: concept, study design, data analysis, manuscript writing and editing. SMJ: data search, manuscript writing and editing. TH: concept, manuscript editing. MP, YA: manuscript editing. ER: data search. HCD: concept.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Institutional Review Board approved this retrospective cohort study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.