Article Text

Abstract
Congestion at the emergency department (ED) is associated with increased wait times, morbidity and mortality. We have identified prolonged wait time to admission as a significant contributor to ED congestion. One of the main contributors to prolonged wait time to admission was due to rejections by ward staff for the beds allocated to newly admitted patients by the Bed Management Unit (BMU). We have identified this as a systemic issue and through this quality improvement effort, seek to reduce the incidence of bed rejections for all admitted patients by 50% from 9% to 4.5% within 6 months. We used PDSA (Plan, Do, Study, Act) cycles to implement a series of interventions, such as updating legacy categorisation of wards, instituting a ‘no rejects’ policy and performing ward level audits. Compared with baseline, there was reduction in rejected BMU allocation requests from 9% to 5% (p<0.01). The monthly percentage of patients with at least one rejection dropped from an average of 7% to 4% (p<0.01). With reduction in the number of rejections, the average wait time to the final request acknowledged by the ward for all admission sources decreased from 2 hours 19 min to 1 hour (p<0.01), thereby allowing the overall wait time to admission to decrease by 68 min, from 5 hours 13 min to 4 hours 5 min. Improvements in the absolute duration and variance of wait times were sustained. Although the team’s initial impetus was to improve ED wait times, this hospital-wide effort improved wait times across all admission sources. There has been a resultant increase in ownership of the admissions process by both nursing and BMU staff. With the conclusion of this effort, we are looking to further reduce the wait time to admission by optimising the current bed allocation logic through another quality improvement effort.
- emergency department
- quality improvement
- efficiency, organizational
- PDSA
- efficiency
- organisational
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Emergency department (ED) congestion is associated with increased morbidity and mortality.1–3 ED congestion is a product of patient arrivals, patient complexity, processes and supply of inpatient beds.4 During our prior efforts to reduce the wait time to consultation at the ED,5 6 we have identified ED congestion as one of the contributing factors to prolonged wait times to consultation. During periods of congestion, ED staff are often called away from their primary roles to manage increased patient load, leading to a cascading cycle of interrupted care and further prolonged wait times.7
We analysed processes affecting ED congestion and found out that patients who were admitted from the ED were waiting up to 5 hours before their transfer to the inpatient ward. Unscheduled ED admissions form a significant number of unplanned admissions to the hospital. In our system, the process of transport of admitted ED patients to their inpatient bed is preceded by the need to allocate a suitable bed by the Bed Management Unit (BMU) of the Admitting Services department, and the confirmation of acceptance of that bed allocation request by the inpatient ward nurses.
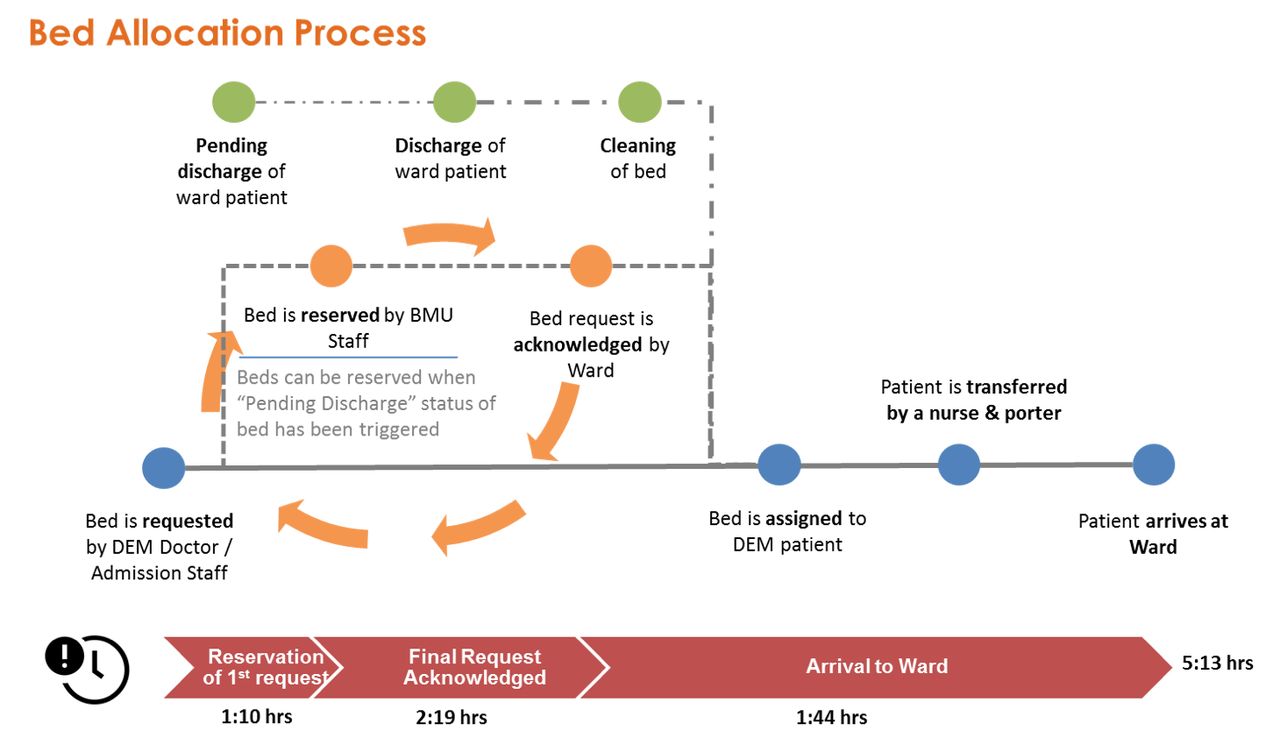
For patients who are admitted, a bed request from the admission source is raised. Based on the bed request for admission, patients are allocated by BMU to an inpatient bed which is either currently empty or is currently holding a patient planned for discharge on the same day. The bed allocation would be confirmed, once the inpatient ward staff acknowledges the BMU allocation request. The inpatient bed would be cleaned prior to being tagged as ready (cleaned). The patient would be then transferred from their admission location to the ready inpatient bed.
The duration from the initiation of bed request for admission to the time of acknowledgement of the final BMU allocation request was found to contribute to most of the wait time to admission. Data also showed that besides the underlying parameters of the bed allocation algorithm, the rejections by inpatient staff of beds allocated by BMU was a major cause of delays.
A subsequent extended audit done on patients admitted from all sources (which admitted ED patients form a subset of) showed that the problem of rejection of allocated inpatient beds was a consistent problem across all admission sources. The sources examined, apart from the ED, include patients admitted for Same Day Admission (SDA), elective admissions and patients admitted directly from specialist outpatient clinics (SOC).
Background
Singapore General Hospital (SGH) is the largest public hospital in Singapore, with 1600 inpatient beds. SGH provides tertiary care to a large proportion of the overall Singapore population, with specialty centres serving patients with oncological, ophthalmological, neurological and cardiac-related conditions. It also sees a significant number of patients with complex haematological and renal diseases. The Department of Emergency Medicine (DEM) sees more than 125 000 patients annually.
The proportion of all patients admitted to inpatient wards are 54%, 20%, 13% and 13% from DEM, SDA, electives and SOC admissions, respectively. Apart from managing patient admissions, the BMU coordinates intraward inpatient bed transfers secondary to patients stepping up from general ward to higher acuity care level wards (high dependency (HD) wards, intermediate care areas (ICAs), intensive care units (ICUs) and vice versa, and for interhospital transfers.
The wait time to admission, defined as wait time from disposition (initiation of bed request) to arrival at final allocated inpatient ward bed, is an institutional key performance indicator tracked by the Ministry of Health of Singapore. With rejections of allocated beds being a major reason contributing to the increase in wait time to admission, we sought to reduce the incidence of rejections of allocated beds for admitted patients from all admission sources by 50% from an average of 9% to 4.5% within 6 months.
We embarked on a root cause analysis to identify the pertinent reasons for rejections of allocated inpatient beds. Four major causes were identified, after examination of the bed allocation logic and feedback from ground staff from DEM, BMU and the inpatient wards.
The first major cause identified was a mismatch in the demand for and the supply of inpatient specialty beds.8 Individual inpatient specialties are allocated inpatient wards. The wards may also be shared between specialties. From purposes of bed allocation, wards were classified as Parent Wards for the primary specialty covering a specific ward.
When Parent Ward beds are unavailable, patients of the said specialty would overflow to Preferred Overflow Wards, and subsequently the Non-Preferred Overflow Wards. We found an increased number of bed rejections by Non-Preferred Overflow Wards. We identified specialties where the number of inpatients outgrew their Primary Ward capacity, and the associated increase in rejections for such specialties.
The second root cause identified was the lack of visibility of local ward arrangements to BMU. Due to legacy practice and existing software system design, the allocation of higher acuity care level beds was performed primarily by ward staff. This meant that they often made reservations of local general ward beds for step-down transfers of patients deemed fit for transfer from higher acuity care to general care beds.
Due to limits in user interaction design of current bed management software, BMU staff were often blind to such local arrangements, which meant that rejections could occur due to double booking of beds, where different patients were allocated to the same general ward bed by both ward staff and BMU.
Aside from ward staff rejecting bed allocation requests due to double booked beds, other common reasons include a change in patient’s condition, and specific subspecialty care required which was not available in the allocated ward. The third root cause identified was that of ward staff being able to reject requests arbitrarily. We received feedback from ground staff within different admission sources and BMU highlighting that it was not uncommon occurrence.
The fourth root cause identified was related to the practice of allocating the beds of incoming newly admitted patients to that of current inpatients who were planned for discharge on the same day. These current patients were physically in the ward and had not vacated their inpatient bed at the point of allocation of their bed to the newly admitted patient.
This meant that whenever there was any change in the discharge plans of the existing patient in the ward, a rejection to the bed allocation had to be made to allow for the newly admitted patient to be matched to another available bed.
Baseline measurement
From April 2017 to May 2018, data from 65 000 admissions from all sources (ED, SDA, electives, SOC) were collected and analysed. 9% of all BMU allocation requests made for admitted patients were rejected by the wards for various reasons. On average, 7% of all admitted patients had at least one rejection, with some patients having multiple rejections for the same admission. Based on admission time stamps, the data showed that with every rejection, the patient’s wait time to admission increased by an additional 45 min.
We found the wait time to admission to average 5 hours and 13 min within this baseline period (figure 1), for which the wait time for the patient’s final BMU allocation request to be acknowledged by the ward made up to 44% of the total duration (2 hours and 19 min).
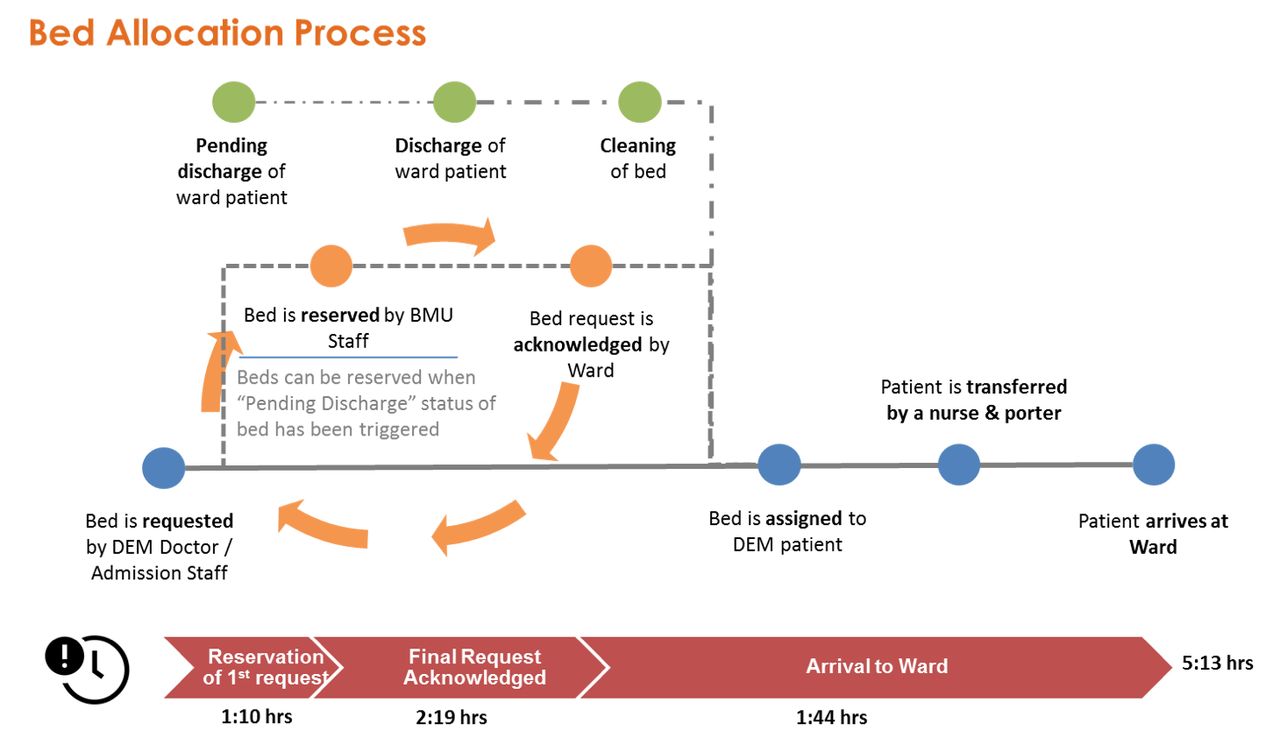
Bed allocation process. BMU, Bed Management Unit; DEM, Department of Emergency Medicine.
Design
Carrying on from prior quality improvement efforts, the team was helmed by an emergency physician, two analysts from the hospital’s Organisation Planning & Performance department and leaders from BMU and nursing. Members of the senior management were engaged early. With their support, many of the broad-based interventions could be executed expediently.
Due to the complexity of this effort, focused group sessions were held with individual groups of key stakeholders (nursing, BMU, management) to directly get buy-in and address data and issues peculiar to their local practice. As the effort matured with local issues managed, the different stakeholders coalesced around regular common meetings as a larger team. The meetings were designed to be targeted, with all points of discussion and action backed by actual analysed data. Feedback was sought from all stakeholders and ground staff, through every step of the effort.
Through reducing the number of rejections of allocated inpatient beds, we hoped to improve patient experience by reducing their overall wait time to admission. We focused on the following areas for improvement and used rapid PDSA (Plan, Do, Study, Act) cycles to execute interventions.
Strategy
PDSA cycle 1
Despite having identified fundamental mismatches in the actual demand for and supply of inpatient beds by specialty, a wholesale reallocation of specialty bed supply to patient demand was deemed to be not executable within the envisioned period of this effort. Instead, to achieve actionable outcomes in the near to medium term, in April 2018 we initiated detailed discussions with inpatient nursing leaders and ward nurses on the ground to increase the ability of wards to cross-cover, especially when non-primary specialty patients overflow.
The legacy categorisation of wards to specific specialties was relooked and updated with inputs from ward nurse managers and their ground staff. Nursing directors further streamlined the criteria, leading to an increase in the number of Parent Wards and Preferred Overflow Wards within the same medical or surgical division. More existing wards were labelled as Parent Wards and Preferred Overflow Wards, as they were deemed (with consensus from the ground) to have the requisite capability to manage patients.
Nursing staff from all inpatient wards were involved in this exercise, and discussions and conclusions were drawn after a period of 2 months, before being formalised, summarised and communicated to BMU. The new categorisation of wards was formally implemented at the beginning of June 2018 for easier coordination operationally between BMU and the wards. Through this engagement, nursing staff acknowledged the purpose of our efforts, which allowed us to implement further PDSA cycles more easily.
PDSA cycle 2
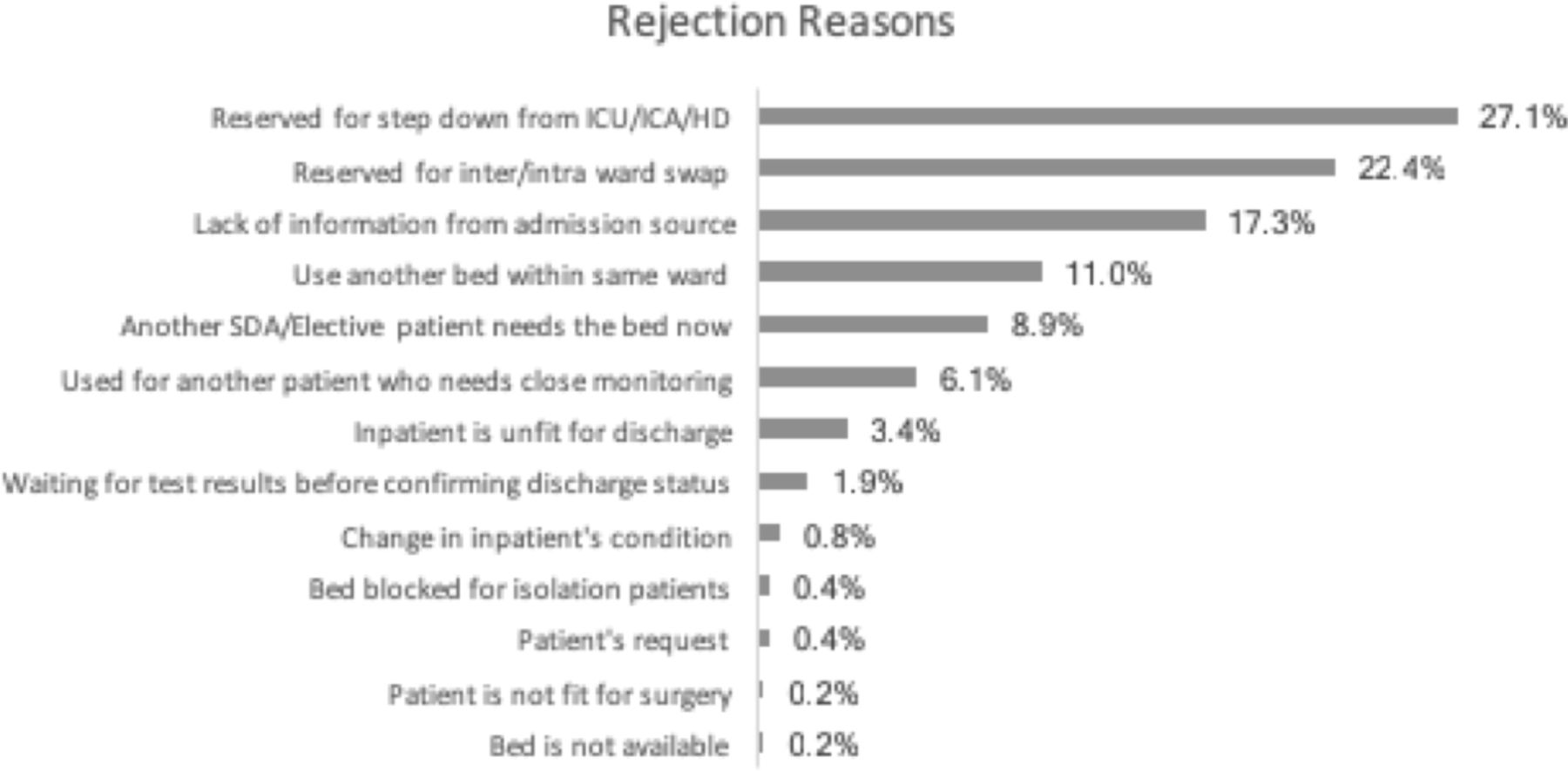
From April 2018, we started examining the reasons for rejections (figure 2). Data were drawn from the bed admissions system and matched to manually captured feedback by BMU staff. The analysis indicated a range of rejections by ward staff, with the reasons of ‘Reserved for step down patients from ICU/ICA/HD’, ‘Reserved for inter/intra ward swap’ and ‘Lack of information from admission source’ being the most common reasons for rejection. Also, feedback from ground staff from the various admission sources and BMU revealed that it was not uncommon that ward staff may reject requests arbitrarily.

List of common reasons for bed rejections. (ICU, intensive care unit; ICA, intermediate care area; HD, high dependency unit; SDA, same day admission.)
The findings were communicated to the nursing leadership. With the consensus from inpatient nursing staff that categorisation of wards was updated and appropriate, a policy of no rejections by ward staff for allocated inpatient beds was instituted at mid-June 2018, disallowing arbitrary rejections.
Regular audits of rejections made were carried out and the impact of rejections on patient experience and wait times were communicated to staff. Such communication was done in tandem with the nursing leaders, which helped ensure sustained compliance to the ‘no rejection’ policy. Nonetheless, ‘legitimate’ rejections were still accepted. We continued to conduct analysis of the rejection reasons to understand their root causes and addressed them in PDSA cycle 3.
PDSA cycle 3
With PDSA cycle 2 ongoing for 5 months, regular audits performed showed general, sustained improvement in the rejection situation. To further reduce rejections in a targeted manner, ward level audits of rejections and their reasons were performed from December 2018.
We assessed the frequency of rejections by individual wards and considered the specific reasons for the rejections. We found out that there were issues of different nature, with regards to each ward’s rejections. The two most common groups of reasons were related to the lack of visibility of local ward arrangements to BMU, causing inpatient ward beds to be double-allocated, and non-Parent Ward rejections arising from patients requiring subspecialised nursing care (chemotherapy regimen related, flap wound management, etc). A separate workgroup to address software system-related updates required to allow BMU visibility of local ward arrangements was set up to address the matter.
For the group of patients requiring subspecialised care which was only available at Parent Wards, data revealed that 90% of such patients were planned admissions via the SDA route. We held focused discussions together with the affected subspecialty nursing staff and BMU and came up with an arrangement, where BMU would be notified of the SDA patients requiring Parent Ward placement, prior to the new patient’s admission. This allowed BMU to pre-emptively reserve beds in the said Parent Wards for these patients and avoid rejections from inpatient ward staff.
Results
From June 2018 to February 2019, after the implementation of PDSA cycles 1, 2 and 3, the monthly average for rejected BMU allocation requests reduced significantly from 9% to 5% (p<0.01). Correspondingly, the monthly percentage of patients with at least one rejection dropped from an average of 7% to 4% (p<0.01) (figure 3). That means an average of 170 more patients were successful in having their inpatient bed allocated with only a single request, instead of requiring multiple allocation requests during the preintervention period.

Run chart for rejections of bed requests. PDSA, Plan,Do, Study, Act.
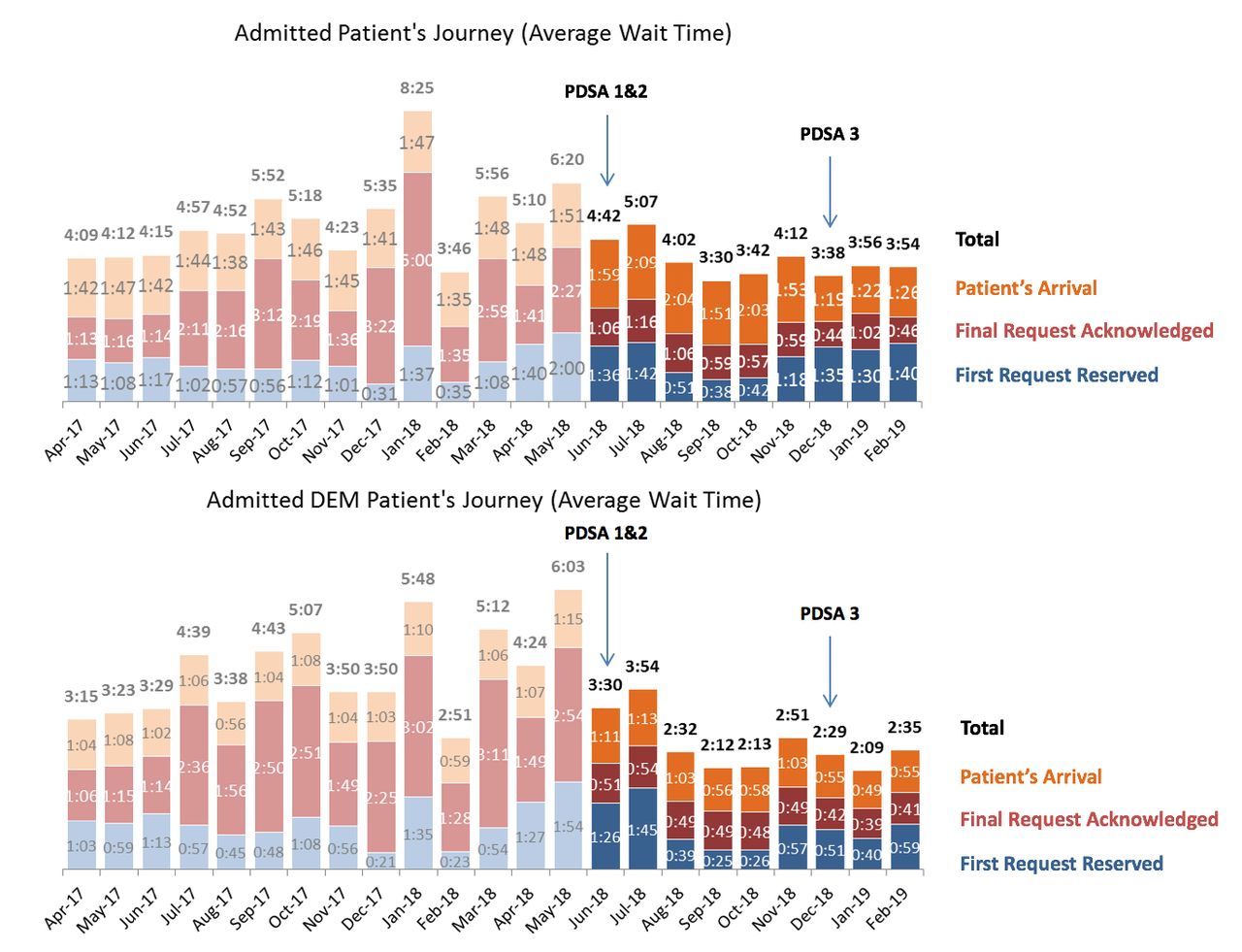
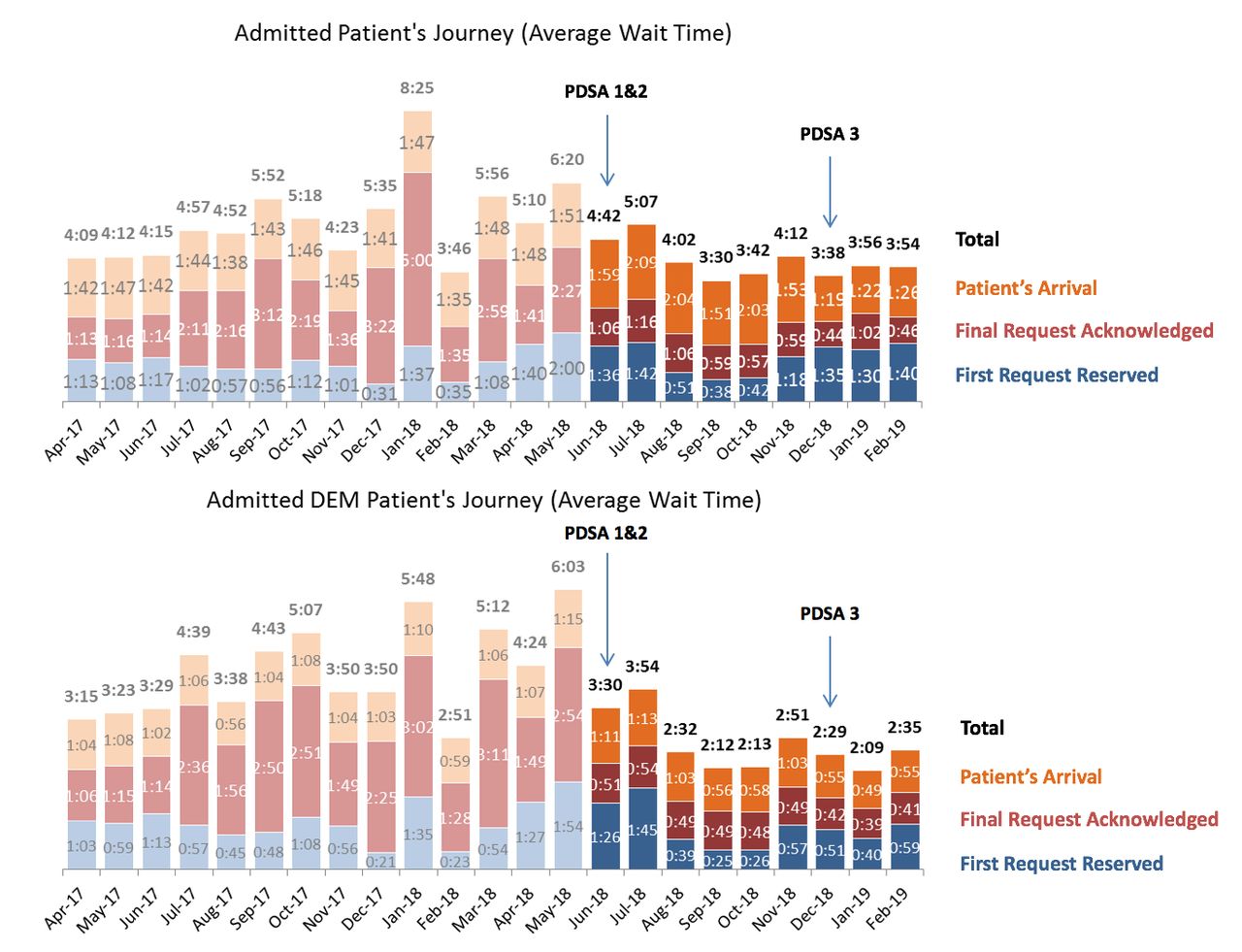
During analysis of the baseline state, we had earlier related that the patient’s wait time to admission increased by 45 min with every additional rejection. With reduction in the number of rejections, the average wait time to the final request acknowledged by the ward for all admission sources decreased from 2 hours 19 min to 1 hour (p<0.01), thereby allowing the overall wait time to admission to decrease by 68 min, from 5 hours 13 min to 4 hours 5 min (p<0.01) (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Reduction in monthly average wait times. DEM, Departmentof Emergency Medicine; PDSA, Plan,Do, Study, Act.
With the improvement in average wait time, we observed a decrease in the variance too, represented by the change in SD before and after implementation. The variance of the wait time of final request acknowledged decreased from 1 hour 13 min to 9 min, and for the overall wait time to admission decreased from 1 hour 11 min to 31 min.
There were improvements seen across all admission sources (figure 4). The biggest improvement seen was for ED admissions, where the average wait time to the final request acknowledged by the ward reduced from 2 hours 10 min to 47 min (p<0.01), with a corresponding reduction in variance from 44 min to 5 min. With acknowledgement of allocation requests expedited, the overall average wait time to admission for ED patients reduced from 4 hours 18 min to 2 hours 43 min (p<0.01), with the variance improving from 59 min to 36 min.
Lessons learned
Although the team’s initial impetus was to improve ED wait times, we realised that a systemic hospital-wide approach was necessary to solve this issue in a comprehensive manner. This resulted in significant improvements in both the absolute duration and variance of the wait time to admission for the ED and the rest of the hospital. This effort illustrated the interdependence between different parts of the hospital and how solving root causes at hospital-wide level can translate to outsized benefits for patients and staff at the ED.
Besides the broad involvement of multiple departments and divisions of the hospital in this effort, the depth of participation from all levels of nursing was extremely important, especially in PDSA cycle 1 where legacy ward categorisation was relooked and updated, and during PDSA cycle 2 where the nursing leadership had expediently instituted the ‘no rejects’ policy.
It was important that feedback and inputs were gathered from the ground and that ground staff were engaged from the start of the effort. Candid and focused discussions were held and pertinent data shared were shared with all members and stakeholders to inform decision-making. The transparent processes and data-driven decision-making allowed all parties to trust the steps the team was taking.
Decisions were not made arbitrarily, especially in the setting of multiple stakeholders with differing priorities and areas of responsibilities. When directing this effort, we realised that aligning all stakeholders to common goals of better patient care and patient experience allowed different parties to bridge differences and move the effort forwards.
Limitations
We were unable to address the issue of fundamental mismatch between bed demand and supply within the duration of this effort. This was mitigated somewhat by PDSA cycle 1 which allowed patients to overflow to more Preferred Overflow wards.
We believe that right siting of patients to their specialist wards is important and that even as patient demographics evolve with time and the hospital’s physical infrastructure remodels, relooking the supply of primary wards allocated to specialties regularly would be an important step to facilitate an efficient and effective bed allocation algorithm.9 We have updated the key stakeholders within the hospital with regards to our findings and a separate workgroup would be convened to address this issue.
We have demonstrated that bed rejections cause delays in the wait time to admission. However, there remains other factors, such as the underlying parameters of the bed allocation algorithm and the time required for physical transport, which contribute to delays too.10 Data gathered from this effort has allowed us to subsegment the patient journey and identify further possible areas of improvement. Optimising the current bed allocation algorithm is the next potential point of improvement to further reduce the wait time to admission.
Conclusions
Rejections of allocated inpatient beds for newly admitted patients contribute significantly to the overall wait time to admission. We have demonstrated how mitigating rejections at the hospital-wide level for patients from all admission sources led to outsized improvements in wait times at the ED.
This broad-based intervention required the buy-in and participation of multiple parts of the hospital and has resulted in increased ownership of the admission process by both nursing and BMU staff. With the conclusion of this effort, we are looking to further reduce the wait time to admission by optimising the current bed allocation logic through another quality improvement effort.
Acknowledgments
The authors acknowledge the following: Ho Ai Lian, Deputy Director, Nursing; Dr Png Hong Hock, Deputy Director, Nursing; Norhayati Bte Ahmad, Deputy Director, Nursing; Salimah Bte Mohd Ayoob, Deputy Director, Nursing; Lee Jiunn Kee, Deputy Director, Admitting Services; Low Seng Kee, Senior Manager, Admitting Services; Joseph Cheong, Senior Executive, Admitting Services; Jade Tan Yu Min, Assistant Manager, Admitting Services; Ivan Ng Kai Boon, Executive, Admitting Services; and Ryan Koh Zhao Yuan, Hospital Executive, OPP.
Footnotes
Contributors SY and LLH both contributed to the design and writing of this quality improvement report. SY and LLH both contributed to data collection and interpretation of the results of this study. SY was the main author of the submitted report. Both SY and LLH were involved in editing the report for clarity and details. SY submitted the report and takes responsibility for the overall content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.