Article Text

Abstract
Glasgow city has the highest cardiovascular disease (CVD) mortality rate in the UK. Patients with left ventricular systolic dysfunction after acute myocardial infarction represent a ‘high-risk’ cohort for adverse CVD outcomes. The optimisation of secondary prevention medication in this group is often suboptimal. Our aim was to improve the use and target dosing of ACE inhibitors (ACEI), angiotensin II receptor blockers (ARBs) and beta-blockers in such patients, through pharmacist-led clinics and cardiology multidisciplinary team collaboration. Retrospective audits characterised baseline care. Prospective pharmacist-led clinics were piloted and rolled out across seven hospitals and primary care localities over four Plan–Do–Study–Act cycles. ‘Hub’ and ‘spoke’ clinics utilised independent prescribing pharmacists with different levels of cardiology experience. Pharmacists were trained through a bespoke training programme—‘Teach and Treat’. Consultant cardiologists provided senior support and governance. Patients attending prospective pharmacist-led clinics were more likely to be prescribed an ACEI (or ARB) and beta-blocker (n=856/885 (97%) vs n=233/255 (91%), p<0.001 and n=813/885 (92%) vs n=224/255 (88%), p=0.048, respectively) and be on target dose of ACEI (or ARB) and beta-blocker (n=585/885 (66%) vs n=64/255 (25%), p<0.001 and n=218/885 (25%) vs n=17/255 (7%), p<0.001, respectively) compared with baseline. The mean dose of ACEI (or ARB) and beta-blocker was also higher (79% vs 48% of target dose, p<0.001% and 48% vs 33% of target dose, p<0.001, respectively) compared with baseline. Use of secondary prevention medication was significantly improved by pharmacist and cardiology collaboration. These improvements were sustained across a 4-year period, supported by a novel approach called ‘Teach and Treat’ which linked training to defined clinical service delivery. Further work is needed to assess the impact of the programme on long-term CVD outcomes.
- Pharmacist
- Evidence-Based Medicine
- Multidisciplinary Team
- Quality Improvement
- Professional Development
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
National Health Service (NHS) Greater Glasgow and Clyde is Scotland’s largest regional health authority, delivering primary, secondary and tertiary care to approximately 1.2 million residents. It encompasses seven local acute and ambulatory hospitals and six separate local council authorities. Three out of these six council authorities appear in the top 10 list of UK-wide authorities with the highest age-standardised death rates for cardiovascular disease (CVD), with Glasgow City having the highest overall rate with approximately 400 age-standardised deaths per 100 000 population.1 Scotland also has amongst the highest prevalence of coronary heart disease across the UK.1 Despite declining case fatality rates from myocardial infarction (MI) across the UK,2 3 patients have worse outcomes than those from comparable European countries.4
The optimisation of secondary prevention medication is crucial in improving outcomes for post-MI patients, especially in those with left ventricular systolic dysfunction (LVSD).5–7 ACE inhibitors (ACEI), or angiotensin II receptor blockers (ARB) if the patient is intolerant, and beta-blockers are first-line agents for such patients and should be prescribed in all patients unless contraindicated.7 These medications should be optimised early in the postdischarge phase, ideally utilising non-medical prescribers.7 8
Within NHS Greater Glasgow and Clyde, baseline acute MI care involved patients being initiated on ACEI (or ARB) and beta-blocker during their admission. These medications were then reviewed postdischarge by cardiac rehabilitation nurses and recommendations were made to general practitioners (GPs) about medication optimisation goals as part of a broader review. Cardiologist outpatient clinic follow-up typically took place 6–12 months postdischarge. Patients with post-MI LVSD without overt clinical heart failure (HF) were not routinely reviewed by HF nurses.
At cardiologist-led clinic follow-up visits, it was noted that many patients were not being prescribed evidence-based therapy at fully optimised doses. Therefore, a baseline audit of care data was conducted in two local hospitals to characterise care—Royal Alexandra Hospital and Vale of Leven. Data were collected through retrospective audit of the cardiac rehabilitation databases and electronic patient records for all consecutive patients with incident acute MI and moderate or severe LVSD on echocardiography over 12 months (1 September 2012–31 August 2013). The endpoints were: the percentage of patients treated with, mean percentage of European Society of Cardiology target dose5 achieved and percentage of patients on full target dose of ACEI/ARB and beta-blocker at the end of the formal cardiac rehabilitation programme. The target daily doses used were: ramipril 10 mg, enalapril 20 mg, lisinopril 20 mg, candesartan 32 mg, losartan 150 mg, valsartan 320 mg, bisoprolol 10 mg, carvedilol 50 mg and nebivolol 10 mg.
Fifty-seven patients with moderate or severe post-MI LVSD were identified. Baseline overall use of ACEI (or ARB) was 89% (n=51/57). The mean percentage of ACEI (or ARB) target dose was 44%, with 21% (n=12/57) of patients achieving the full target dose. Baseline use of beta-blocker was 82% (n=47/57). The mean percentage of beta-blocker target dose was 31%, with 7% (n=4/57) of patients achieving the full target dose.
The Specific Measurable Achievable Realistic Time-limited aim of our programme was to improve the use and target dosing of ACEI (or ARB) and beta-blocker in all patients with LVSD secondary to incident acute MI across a large regional health authority by the end of a patient’s cardiac rehabilitation programme, typically within 4 months of discharge from hospital, through pharmacist-led clinics and cardiology multidisciplinary team collaboration.
Background
The development of LVSD independently predicts mortality in patients after acute MI and, therefore, identifies a ‘high-risk’ cohort.9 LVSD increases the risk of both future HF and sudden cardiac death.9
Disease registry data shows us that the optimisation of secondary prevention medication is known to be suboptimal across many healthcare systems.9 Improving HF and MI outcomes are key areas for service improvement across the UK.10 11 Heart disease management and rehabilitation are also key priorities for Scottish Government.12
Since 2006, pharmacists and nurses in the UK have been able to train as independent prescribers. A recent meta-analysis shows that such professionals can use these qualifications to deliver aspects of CVD management, such as systolic blood pressure and low-density lipoprotein cholesterol control, comparable with their medical colleagues.13 Trial evidence also shows that outcomes can be improved by incorporation of these professionals into the cardiology multidisciplinary team, especially in the field of HF and/or LVSD.14 15
Measurement
Endpoints
Percentage of patients treated with, mean percentage of target dose16 achieved of, and percentage of patients on full target dose of ACEI (or ARB) and beta-blocker at the end of the cardiac rehabilitation programme.
Data collection and analysis
Prospective data on medication optimisation from pharmacist-led clinics were collected on standardised clinic discharge forms and collated in a password-protected Microsoft Access database on NHS-encrypted computers.
Data on the prescribing of medication were summarised in percentages. Data on target doses of medication were summarised in percentage of patients on graded categorical thresholds (ie, 0%, 1%–24%, 25%–49%, 50%–74%, 75%–99% and 100% of target dose) and mean percentage of target dose achieved across all patients. The χ2 tests and t-tests were used to test for differences in the endpoints at the end of the programme compared with baseline.
Design
In collaboration with consultant cardiologists, pharmacist-led post-MI LVSD clinics were designed to improve medication optimisation. Prospective patients were identified during acute MI admissions by cardiac rehabilitation nurses and electronically referred at hospital discharge to the pharmacist-led clinic in addition to all aspects of usual care, including cardiac rehabilitation and cardiologist follow-up. The pharmacists delivering the clinics prescribed in line with guidelines.5 6 16 Consultant cardiologists provided senior medical support and associated clinical governance. Patients were vetted to confirm suitability before being invited to attend. Patients were phoned to attend by a service administrator and sent a letter confirming the appointment. Patients not contactable by phone were appointed by letter only. Appointment slots were 15 min and medical records staff supported clinic administration tasks. Hand-written prescriptions were issued directly from clinics and patients were typically reviewed at 2 weekly intervals until medications were judged to be optimised. Letters to GPs were written within three working days of each clinic, documenting all changes in prescribing. Letters were automatically uploaded to electronic medical records, which were available to all primary and secondary care clinicians.
Ethics
Ethical approval was not required for this service development project.
Patient and public involvement
No patients were involved at the design stage. A qualitative patient experiences study has been completed and awaits publication.
Strategy
The service was sequentially rolled out and evaluated over four Plan–Do–Study–Act (PDSA) audit cycles.
PDSA Cycle 1 (1 September 2013–31 August 2014)
PLAN: Clinics were piloted in two hospitals: Royal Alexandra Hospital and Vale of Leven. This pilot concentrated on patients with moderate or severe LVSD and was supported by funding from NHS Education for Scotland.
DO: Two pharmacists (NHS Agenda for Change (AFC) Band 8a) with between 5 and 9 years of cardiology experience, who were already qualified independent prescribers and trained in clinical examination and venepuncture, delivered the clinics in an outpatient setting.
PDSA Cycle 2 (1 September 2014–31 August 2015)
PLAN: Clinics were rolled out to two further hospitals: West Glasgow Ambulatory Care Hospital and Glasgow Royal Infirmary. Retrospective baseline data were collected from Glasgow Royal Infirmary for the 6 months preceding initiation of the clinic to ensure that there was a similar requirement for the clinic. No baseline data were collected in West Glasgow Ambulatory Care Hospital, as the original site of this hospital closed during this period making consecutive patient data collection impossible. To support the roll-out and criteria widening (to all grades of LVSD), the model was developed into ‘hub’ and ‘spoke’ clinics. Pharmacist independent prescribers with different levels of cardiology experience were recruited to deliver stratified clinics depending on the risk profile of the patient. The risk profile was assessed by the experienced PDSA Cycle 1 pharmacists at the point of vetting. In each hospital site, specialist cardiology pharmacists were used to deliver a ‘hub’ clinic for patients with moderate or severe grades of LVSD, or those with additional risk factors (eg, signs and symptoms of ischaemia, significant residual coronary heart disease or complex comorbidities). In surrounding primary care localities, such as local health centres, General Practice (GP)-based pharmacists were used to deliver ‘spoke’ clinics for patients with mild LVSD. GP-based pharmacists were general clinicians and were peer supported remotely by specialist cardiology pharmacists. This phase of the project was supported by funding from NHS Education for Scotland.
DO: Two additional specialist pharmacists were used, both already experienced prescribers with 9–25 years of cardiology experience (AFC Bands 8a and 8b). An additional nine generalist GP-based pharmacists (AFC Band 8a) were trained to deliver primary care clinics through a bespoke local education and training programme—‘Teach and Treat’. This programme included experiential learning, taught lectures, online webinars, links to national guidelines, physical examination training (including blood pressure/pulse measurement, pitting for oedema and chest auscultation) and venepuncture. At the end of the training, all pharmacists sat a multiple-choice examination and an objective structured clinical examination, developed in partnership between the experienced PDSA Cycle 1 pharmacists and a consultant cardiologist, to assess competence before commencing autonomous clinic work.
PDSA Cycle 3 (1 September 2015–31 August 2016)
PLAN: Clinics were rolled out to two further hospital sites: New Victoria Infirmary and Queen Elizabeth University Hospital. As before, retrospective baseline data were collected from both sites for the preceding 12 months. The Queen Elizabeth University Hospital opened during this time period but baseline data were able to be characterised from its predecessor, the Southern General Hospital. Unlike the other sites, the Southern General Hospital provided a consultant cardiologist-led post-MI clinic approximately 1 month postdischarge at baseline.
DO: An additional specialist pharmacist IP (AFC Band 7), with 14 years of cardiology experience, was trained and deployed in one of the ‘hub’ clinics. The other new specialist ‘hub’ clinic was delivered by an existing service pharmacist. An additional two generalist GP-based pharmacists (AFC Band 8a) were trained to deliver primary care clinics. All were independent prescribers.
PDSA Cycle 4 (1 September 2016–31 August 2017)
PLAN: Clinics were rolled out to the final hospital site: Inverclyde Royal Hospital. Baseline data were not available from Inverclyde Royal Hospital due to a lack of a baseline cardiac rehabilitation database.
DO: Two additional specialist pharmacists (AFC Bands 7 and 8b), with 6 and 19 years of cardiology experience, respectively, and two additional generalist GP-based pharmacist (AFC Band 8a) were recruited to deliver ‘hub’ and ‘spoke’ clinics, respectively. All pharmacists were trained as described above and were independent prescribers.
Results
PDSA Cycle 1
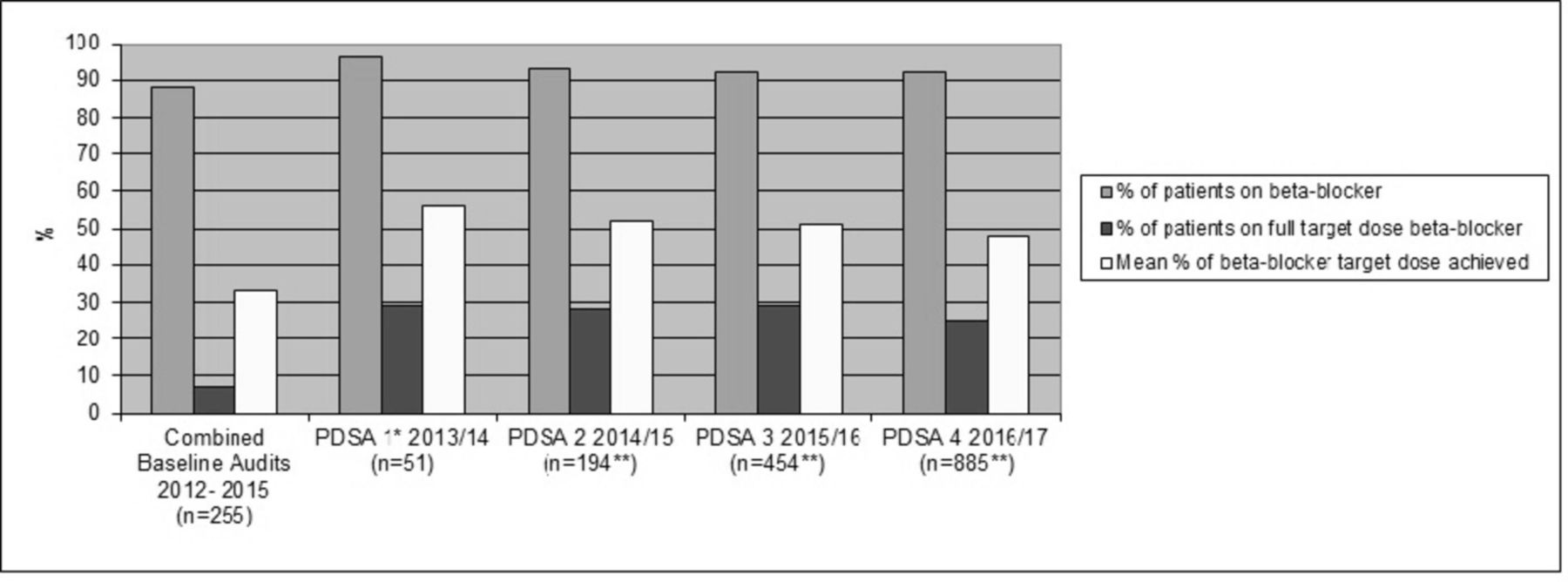
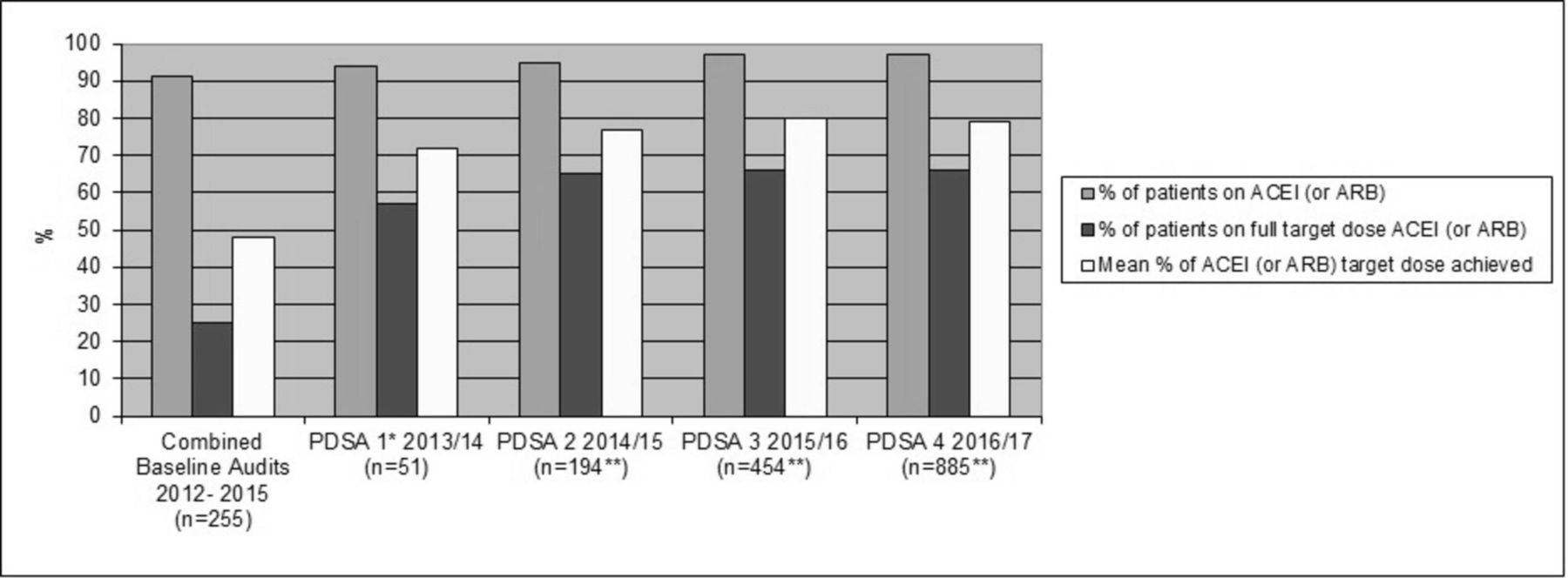
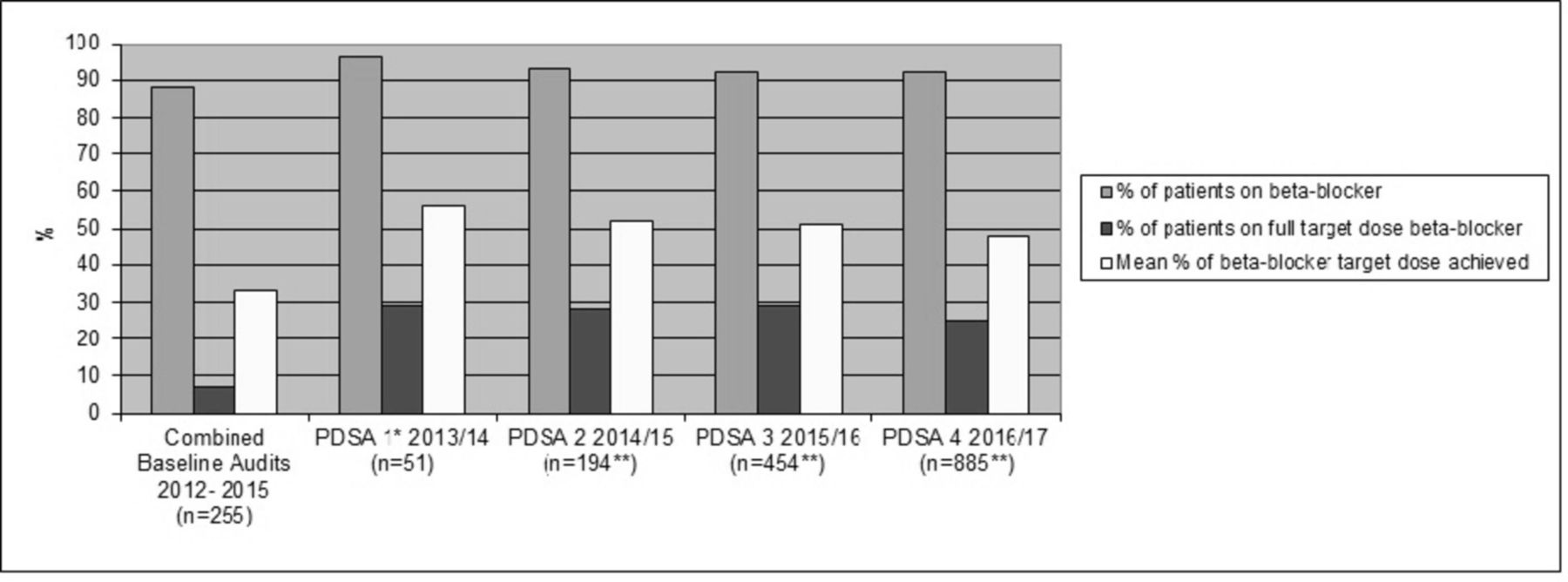
STUDY: 51 patients were reviewed in the pharmacist-led clinic during the first year of the project. The use of ACEI (or ARB) increased from 89% in the baseline audit (n=51/57) to 94% (n=48/51). The mean percentage of ACEI (or ARB) target dose also increased from 44% in the baseline audit to 72%, with 57% (n=29/51) patients achieving the full ACEI (or ARB) target dose compared with 21% in the baseline audit (n=12/57). The use of beta-blockers increased from 82% in the baseline audit (n=47/57) to 96% (n=49/51). The mean percentage of beta-blocker target dose also increased from 31% in the baseline audit to 56%, with 29% (n=15/51) of patients achieving the full beta-blocker target dose, compared with 7% (n=4/57) in the baseline audit. The results were published in abstract form.17
ACT: The service steering group in collaboration with the local strategic cardiology planning committee endorsed a plan to roll the clinics out across all hospital sites in the health authority and to widen the inclusion criteria to include all grades of LVSD post-MI.
PDSA Cycle 2
STUDY: 58 patients with any grade of LVSD post-MI were identified in the baseline Glasgow Royal Infirmary audit. Ninety-one per cent (n=53/58) of Glasgow Royal Infirmary patients were prescribed an ACEI (or ARB). The mean percentage of ACEI (or ARB) target dose was 48%, with 24% (n=14/58) of patients achieving the full target dose. Ninety-one per cent (n=53/58) of Glasgow Royal Infirmary patients were also prescribed beta-blockers. The mean percentage of beta-blocker target dose was 33%, with 7% (n=4/58) of patients achieving the full target dose.
A further 143 patients were reviewed at the pharmacist-led clinics during the second year of the project, making the running total 194 patients. The use of ACEI (or ARB) was 95% (n=185/194). The mean percentage of ACEI (or ARB) target dose increased from 72% in PDSA Cycle 1 to 77%, with 65% (n=126/194) of patients achieving the full ACEI (or ARB) target dose. The use of beta-blockers dipped slightly from 96% in PDSA Cycle 1 to 93% (n=180/194). The mean percentage of beta-blocker target dose decreased slightly from 56% in PDSA Cycle 1 to 52%, with 28% (n=54/194) patients achieving the full beta-blocker target dose.
ACT: The service steering group endorsed the plan to continue sequential roll-out across the regional health authority.
PDSA Cycle 3
STUDY: 76 patients with any grade of LVSD post-MI were identified in the baseline New Victoria Infirmary audit and 64 patients were identified in the Southern General Hospital audit. 88% (n=67/76) of New Victoria Infirmary patients and 97% (n=62/64) of Southern General Hospital were prescribed an ACEI (or ARB). The mean percentage of ACEI (or ARB) target dose was 42% for New Victoria Infirmary and 61% for Southern General Hospital, with 18% (n=14/76) of patients achieving the full target dose at New Victoria Infirmary and 38% (n=24/64) at Southern General Hospital. Eighty-eight per cent (n=67/76) of New Victoria Infirmary patients and 89% (n=57/64) of Southern General Hospital were prescribed beta-blockers. The mean percentage of beta-blocker target dose was 28% at New Victoria Infirmary and 41% at Southern General Hospital, with 3% (n=2/76) of New Victoria Infirmary patients and 11% (n=7/64) of Southern General Hospital patients achieving the full target dose. Baseline medication optimisation in the Southern General Hospital was higher than other sites, potentially due to the baseline consultant cardiologist-led post-MI clinic.
A further 260 patients were reviewed at the pharmacist-led clinics during the third year of the project, making the running total 454 patients. The use of ACEI (or ARB) was 97% (n=440/454). The mean percentage of ACEI (or ARB) target dose increased from 77% in PDSA Cycle 2 to 80%, with 68% (n=307/454) patients achieving the full ACEI (or ARB) target dose. The use of beta-blockers was 92% (n=416/454). The mean percentage of beta-blocker target dose was 51%, with 29% (n=130/454) patients achieving the full beta-blocker target dose.
ACT: The service steering group endorsed the plan to continue sequential roll-out to the final hospital site.
PDSA cycle 4
STUDY: A further 431 patients were reviewed at the pharmacist-led clinics during the fourth year of the project, making the running total 885 patients. Overall use of ACEI (or ARB) was 97% (n=856/885). The mean percentage of ACEI (or ARB) target dose was 79%, with 66% (n=585/885) patients achieving the full ACEI (or ARB) target dose. The use of beta-blockers was 92% (n=813/885). The mean percentage of beta-blocker target dose dipped slightly from 51% in PDSA Cycle 3 to 48%, with 25% (n=218/885) patients achieving the full beta-blocker target.
ACT: The service steering group planned to consolidate the clinic within each hospital site, embedding it in routine care delivery, without any immediate plans for further expansion within the health authority. Discussions were undertaken with Scottish Government about rolling the clinics out to other Scottish health authorities and funding was secured from NHS Education for Scotland to allow sequential national expansion of the ‘Teach and Treat’ programme.
The table 1 summarises the baseline audits and four PDSA cycle results. The figures 1 and 2 show medication optimisation over the length of the programme compared with the combined baseline audits across the five hospitals.
Comparison of ACEI (or ARB) and beta-blocker optimisation in baseline audits versus pharmacist-led clinics

{kind=link}
{kind=link}
Patients in the pharmacist-led clinics were statistically more likely to be prescribed ACEI (or ARB) and beta-blocker compared with patients in the combined baseline audits (n=856/885 (97%) vs n=233/255 (91%), p<0.001 and n=813/885 (92%) vs n=224/255 (88%), p=0.048, respectively). Patient’s in the pharmacist-led clinics were also more likely to be on full target dose ACEI (or ARB) and beta-blocker compared with baseline (n=585/885 (66%) vs n=64/255 (25%), p<0.001 and n=218/885 (25%) vs n=17/255 (7%), p<0.001, respectively). The mean dose of ACEI (or ARB) and beta-blocker was also higher compared with baseline (79% vs 48% of target dose, p<0.001% and 48% vs 33% of target dose, p<0.001, respectively).
Lessons and limitations
Significant improvements in the important clinical surrogate marker of secondary prevention prescribing were seen over this 4-year programme. Patients with LVSD as a result of an acute MI need to be aggressively managed, as adverse cardiac remodelling can rapidly develop in the post-acute phase of the myocardial insult.18 19 Evidence shows that early pharmacological optimisation can impact favourably on such adverse remodelling.19 Thus, early optimisation of medication in this programme gives patients the best chance of left ventricular recovery and the prevention of HF.
Suboptimal uptitration of secondary prevention medication following acute MI is not a problem unique to NHS Greater Glasgow and Clyde. Evidence from the UK and international healthcare systems highlights the need for further work.20–27 The optimisation of ACEI (or ARB) and beta-blocker seen in this programme is superior to that described in previous studies and, therefore, some of the learning may be applicable to other areas.25–27
The involvement of pharmacist independent prescribers as care providers in cardiac rehabilitation programmes is a growing role globally.21 28 29 It is recognised from within pharmacy that for such interventions to succeed they need to be collaborative and multidisciplinary in nature, rather than standalone systems.15 Multidisciplinary models of care, anchored by senior medical leadership, are accepted standards of care,5–8 and such working within our programme delivered a clearly defined and robust clinical governance structure, generating widespread trust and confidence in all staff members.
This project was supported by initial NHS funding, designed to support the Scottish Government pharmacy strategy.30 Without this funding, senior local strategic pharmacy support and the underpinning government policy, this service would not have been sustainable. Commitment of the pharmacy teams involved was also supported by a redesign in workload, including utilising better skill mix and rationalising the necessity of historic tasks.
Strengths
This is the first UK programme to systematically describe the post-discharge optimisation of secondary prevention in patients with post-MI LVSD across a large regional health authority. In doing so, it sets a benchmark for comparison for future clinicians and researchers.
The delivery and evaluation of complex interventions is notoriously difficult.31 This quality improvement programme delivered lasting change over Scotland’s largest health authority, utilising multiple different healthcare professionals across primary and secondary care. The collaborative ‘hub’ and ‘spoke’ model used, incorporating both generalists and specialists, has the potential to be replicated by others.
Across Scotland, independent prescribing qualifications are underutilised by pharmacists; this represents an untapped resource.32 The ‘Teach and Treat’ model was implemented as a means of supporting clinical supervision for this group to improve competence and confidence in autonomously managing patients. This type of project, where targeted at measurable public health problems and supported by appropriate governance structures, has the potential to improve clinical outcomes and frontline service delivery. As such, this project is now cited in the Scottish Government strategy for pharmacy as a potential future model of care for the profession.30
The work burden for medical staff, including consultants and GPs, is growing.33 34 The ageing population and increasing multimorbidity is likely to worsen this problem. This model has the scope to spread prescribing and medication optimisation roles, traditionally delivered by medical staff, across other disciplines.
Limitations
Some of the limitations of the baseline model of care may not be applicable to other regions. For example, our baseline cardiac rehabilitation model of care did not involve nurse-led prescribing, as seen in some other authorities. Therefore, our findings may not be the best solution in such areas.
The ‘hub’ clinic model does require patients to attend pharmacist-led clinics at the hospital, in parallel to the conventional cardiac rehabilitation programme, and appointment burden is known to impact significantly on cardiac patients.35 A study of qualitative patient feedback has been completed to address these concerns and awaits publication. Evolution of the intervention across PDSA Cycles 2–4 also involved reviewing ‘lower risk’ patients closer to home, in local health centres, to partially address this issue and in keeping with Scottish Government health policy.36
As a complex intervention, the clinic model consists of multiple new components, including the introduction of pharmacists as caregivers, the direct prescribing of medications from clinics (rather than making recommendations to GPs) and an enhanced engagement model utilising phone calls in addition to letters. It is not possible to know the weight of influence of each of the components on the outcome.
As a quality improvement project, rather than a randomised controlled trial, this project is inherently at greater risk of confounding. For example, the patient characteristics in each of the baseline audits and PDSA cycles are likely to differ. This may be reflected in the slight changes in ACEI (or ARB) and beta-blocker prescribing seen over time. It is uncertain whether this is explained by the difference in the patient cohort over time, such as patients with more severe LVSD in the pilot phase having a higher sympathetic drive and hence tolerating slightly higher doses of beta-blocker. Alternatively, changes may reflect the challenges of involving more staff members with different levels of experience. There were also significant changes in our health authority over the time period of the intervention, including the closure of three older hospitals and the opening of a new state-of-the-art hospital to provide acute care to a large proportion of the population. Reasons for not achieving target doses were not available for both time periods, so are not described.
The pharmacists involved in clinic delivery also commonly impacted on mineralocorticoid receptor antagonist optimisation, as seen in the pilot.17 Complete data, including the presence or not of heart failure symptoms and diabetes, needed to compare these endpoints across the whole population were not available in all cardiac rehabilitation databases used for the baseline audits. All patients were also not eligible for these medications (eg, those with mild LVSD). Other clinical factors, including patient education, cardiac rehabilitation engagement, medicines reconciliation, lipid control and the requirement for reassessment of left ventricular function (where appropriate), were also commonly reviewed. Similarly, complete data were not available in the baseline audits in order to describe and compare these interventions, and some of these interventions were only appropriate in subsets of patients.
This paper only describes the prescribing outcomes of patients that were known to the local cardiology teams and engaged with the cardiac rehabilitation process after discharge. It is well known that many patients do not engage fully with cardiac rehab after discharge.37 The Inverse Care Law suggests that this group of patients may ultimately have the greatest unmet need.38
Next steps
This paper describes the short-term optimisation of ACEI (or ARB) and beta-blockers in patients with LVSD as a result of an acute MI. Future work is needed to describe the persistence of prescribing over time in these patients. The impact of this project on clinical outcomes is also unknown and requires appropriate evaluation. Plans are underway to deliver a sequential national roll-out of the model to other Scottish regional health authorities.
In parallel to this work, the pharmacy profession in Scotland are now systematically delivering frontline care in primary care.39 This paradigm change in the working model of the profession brings with it both opportunities and challenges for this project. Ultimately, this change will result in workforce-wide pharmacists delivering these types of interventions as part of routine practice. Plans to adequately train, support, ensure governance and evaluate these processes are vital to ensure success.
To support the delivery of these new advanced pharmacist roles within the cardiology multidisciplinary team, a competency framework for pharmacists has been developed40 and work is underway to accredit this with the Royal Pharmaceutical Society, in order to standardise the quality and consistency of this type of advanced practice.
Conclusion
The use of secondary prevention medication with prognostic importance was significantly improved by collaboration between pharmacists and the cardiology multidisciplinary team in patients with post-MI LVSD. These improvements were sustained across multiple sites over a 4-year period, as this service was sequentially rolled-out across a large regional health authority. This achievement was underpinned by a novel multidisciplinary approach called ‘Teach and Treat’ which linked education and training to defined clinical service delivery, including linking specialist and generalist pharmacy practice. Further work is needed to assess the impact of the programme on long-term cardiovascular outcomes.
References
Footnotes
Contributors PF, AW, FR and CM contributed to the concept/design. PF contributed to the data analysis and is the lead author. PF, LM, IS, SM and CM delivered staff training/teaching and contributed to the project planning. PF and CM contributed to the funding bid. PF, LM, IS and SM contributed to the intervention. LM, IS, SM, MR, AW, FR, CR and CM contributed to the manuscript revision. MR, AW and FR contributed to the strategic workforce support. AW and FR are the funders and contributed to the intervention planning. CR contributed to the pilot data. CM contributed to the clinical/academic supervision.
Funding NHS Education for Scotland (pilot and training).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.