Article Text

Abstract
Interactive patient portals are a valuable tool for engaging patients in their healthcare, with various functionalities including viewing laboratory results, refilling prescriptions and communicating directly with nurses, physicians and other healthcare providers via electronic messaging. The utility of patient portals is limited primarily from lack of patient uptake and enrolment due to a variety of factors including lack of awareness, low health literacy, poor technology mastery, lack of availability of a smartphone or computer and distrust of the security of their personal health information. We aimed to increase enrolment in the Epic (O2) MyChart patient portal among patients receiving HIV care through our Infectious Diseases clinic via a standardised sign-up protocol during their clinic visits. This intervention resulted in a modest increase in enrolled patients. However, the factors preventing a more dramatic increase in patient uptake remain unclear.
- continuous quality improvement
- ambulatory care
- communication
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Health information technology (HIT) and interactive patient portals have an ability to engage patients in their own healthcare like never before. While Meaningful Use criteria set a minimum standard for the adoption of HIT, patient portals have increasing value through their various functionalities. Patients who use patient portals have cited the ability to schedule appointments, receive appointment reminders, visualise bills and medication lists and request prescription refills as the main benefits to enrolling.1 While further research on the benefits of patient portals in healthcare outcomes is necessary, one study found that use of a patient portal can improve control of chronic disease and medication adherence2 while another discovered that patients enrolled in the patient portal had reduced rates of hospital admissions and emergency room visits.3 The Epic (O2) MyChart patient portal has been established in outpatient clinics in our healthcare system. Among 527 HIV-positive patients actively following in the Infectious Diseases clinic, only 54% (289 patients) were enrolled in MyChart. The aim of this study was to increase MyChart enrolment among HIV-positive patients receiving care within Infectious Diseases clinic by 15% in 3 months with education efforts and a standardised protocol for enrolment.
Methods
Pre-implementation MyChart enrolment status was extracted and tabulated from Epic (O2) Electronic Medical Record of HIV-positive patients who were actively receiving HIV care through our Infectious Diseases outpatient clinic. A standardised protocol for enrolment of HIV-positive patients was initiated for a 3-month study period enacted during routine clinic visits. At the time of rooming, nursing staff reviewed the patient’s MyChart enrolment status. For patients not yet enrolled in the portal, after the nurse completed the rooming process he/she launched the MyChart sign-up via the MyChart Administration tab within Epic. This generated an enrolment code for the patient who would then complete the sign-up on the computer in the room. Once the provider entered, the patient was asked to install the MyChart mobile application if they owned a smartphone. MyChart enrolment data for the clinic HIV patients was extracted from Epic at 3 and 7 months following implementation of the intervention. The study protocol was disseminated to clinic staff via email, and pictorial instructions demonstrating the enrolment process were posted in clinic. Reminder stickers were placed on room computers. Patients had the ability to refuse MyChart enrolment at any time during the sign-up process or un-enrol at any time.
Results
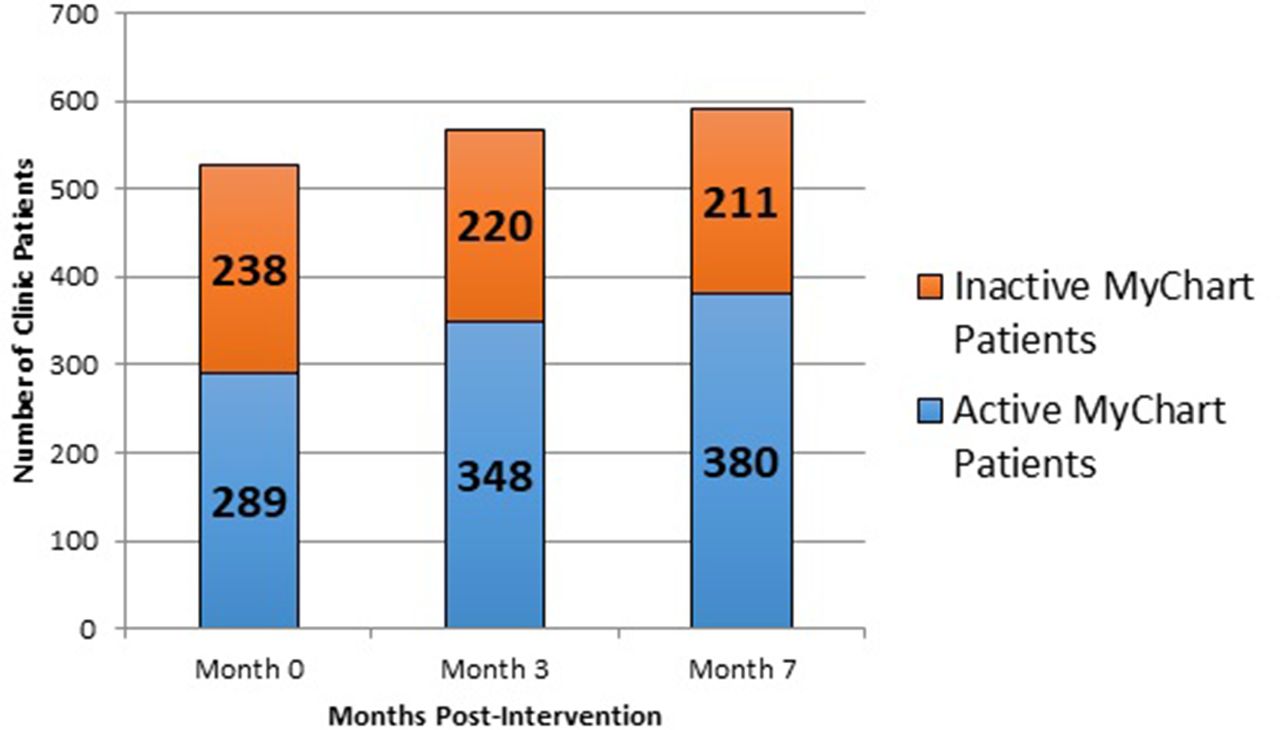
All HIV-positive patients following in the Infectious Diseases clinic were included in the study to assess the overall improvement in MyChart enrolment following protocol implementation. Well-controlled HIV-positive patients are routinely scheduled in clinic every 6 months; poorly controlled patients are seen more frequently at the discretion of their physician. Figure 1 summarises the total MyChart enrolment shifts during our study sample. Over the initial 3-month study period, there was a rise in total HIV clinic patients from 527 to 568. In this time frame, actively enrolled patients increased by 6.4%. At 7 months, the total HIV clinic patients were 591, and there was an increase in patient portal enrolment of 9.5% compared with the pre-intervention percentage (figures 1 and 2).

MyChart patient enrolment in HIV-positive patients seen in the clinic during intervention period.

{kind=link}
{kind=link}
Overall percentage of enrolled patients over the study period.
Discussion
Despite reported benefits of patient portals, uptake and use of these services remain an issue. Low enrolment is most common in some of the most vulnerable patient populations, with ethnic minorities, those with lower completed education levels and those with lower income being less likely to register. Non-users cited a lack of knowledge about the portal as the main reason for not enrolling.1 We aimed to overcome this barrier by describing the portal and enrolling patients face-to-face during their clinic visits. Informational brochures were also offered to patients. In another study of urban adults, lack of health literacy and problems with technology use were other limitations to enrolment.4 While this may have affected enrolment in our study, we attempted to mediate this by loading and demonstrating the MyChart cell phone application to willing patients while they were present in clinic. Although a modest increase in patient portal enrolment was seen after our intervention, other unaccounted factors may have dampened a more dramatic increase in enrolment. Given the potential for patient portals to improve control of chronic diseases such as HIV and support better medication adherence, which is of particular concern in lack of viral load suppression in HIV, more research is needed on methods of engaging patients to enrol and regularly use interactive patient portals.
Footnotes
Contributors Contributorship Statement: JN planned the study, implemented study, wrote the manuscript and is content guarantor. AL implemented the study. RK wrote the manuscript, edited, and implemented. RS wrote manuscript and edited.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This quality improvement project was approved by the University of Kansas Health System institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.