Article Text

Abstract
Objective While disruptions in medications are common among patients who survive critical illness, there is limited information about specific medication-related problems among survivors of critical care. This study sought to determine the prevalence of specific medication-related problems detected in patients, seen after critical care discharge.
Design Consecutive patients attending an intensive care unit (ICU) follow-up programme were included in this single-centre service evaluation.
Setting Tertiary care regional centre in Scotland (UK).
Participants 47 patients reviewed after critical care discharge at an ICU follow-up programme.
Interventions Pharmacists conducted a full medication review, including: medicines reconciliation, assessing the appropriateness of each prescribed medication, identification of any medication-related problems and checking adherence.
Measurements Medication-related problems in patients following critical care discharge. Interventions and medication-related problems were systematically graded and risk factors were identified using an adapted version of the National Patient Safety Agency Risk Matrix.
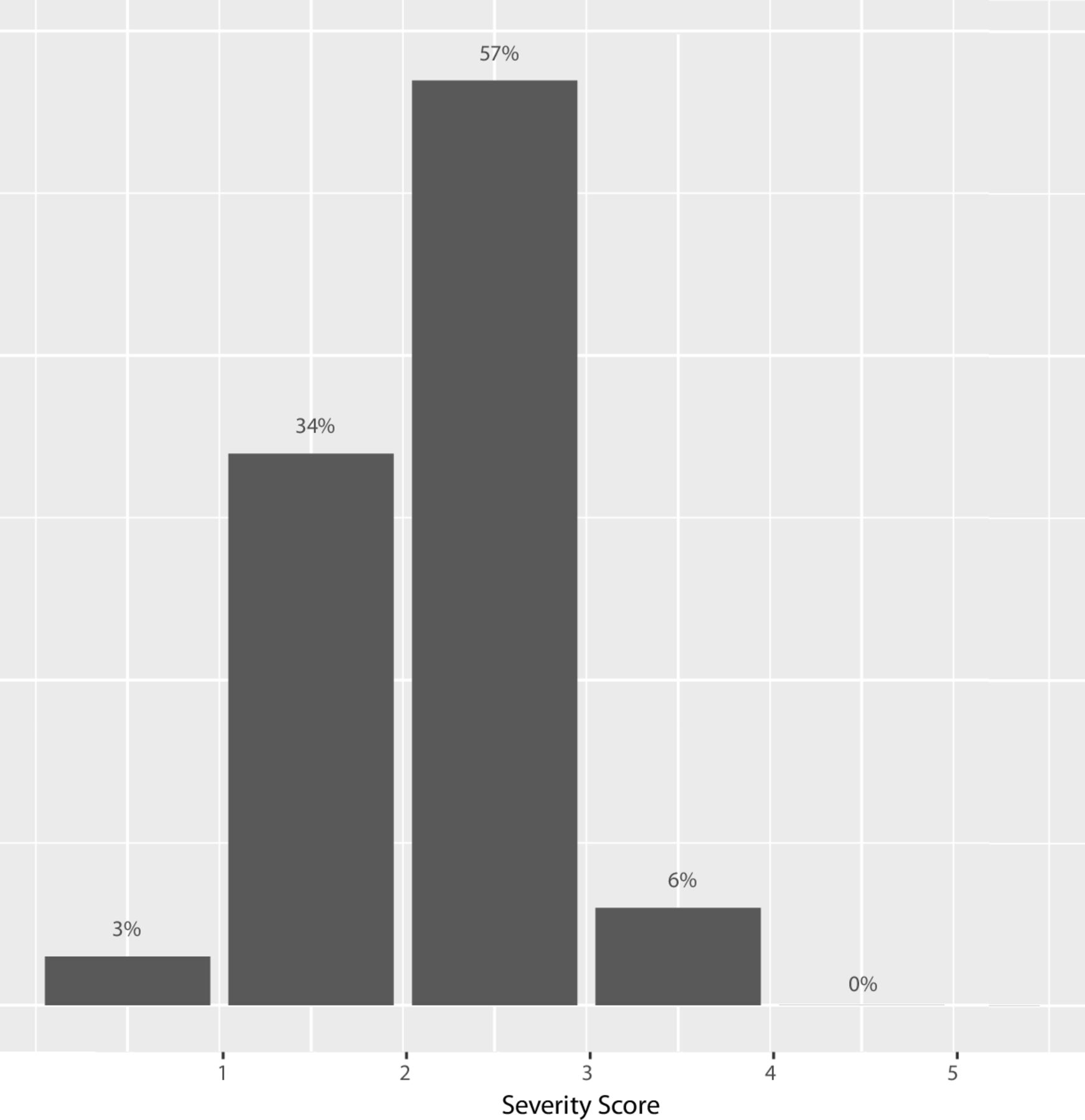
Main results 69 medication-related problems were identified in 38 (81%) of the 47 patients. The most common documented problem was drug omission (29%). 64% of the medication-related problems identified were classified as either moderate or major. The number of pain medications prescribed at discharge from intensive care was predictive of medication-related problems (OR 2.02, 95% CI 1.14 to 4.26, p=0.03).
Conclusions Medication problems are common following critical care. Better communication of medication changes both to patients and their ongoing care providers may be beneficial following a critical care admission. In the absence of highly effective communication, a pharmacy intervention may contribute substantially to an intensive care rehabilitation or recovery programme.
- clinical pharmacology
- critical care
- evaluation methodology
- healthcare quality improvement
- medical error, measurement/epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- clinical pharmacology
- critical care
- evaluation methodology
- healthcare quality improvement
- medical error, measurement/epidemiology
Introduction
Medication errors commonly occur in patients whose hospital stay includes an intensive care unit (ICU) admission.1 When patients are critically ill, their chronic drug therapies are frequently withheld in the ICU but are often, inappropriately, not restarted.2 3 Furthermore, new therapies are often commenced, which may be unnecessary in the long term, such as drugs prescribed for stress ulcer prophylaxis and antipsychotics prescribed for delirium.4 5 The care of the complex and dynamic physiology of these patients is made more challenging by frequent transitions in care across the healthcare system, and poor communication at the time of discharge.6 7
These medication problems may play a role in the development of Post Intensive Care Syndrome (PICS). PICS includes physical, social, cognitive and psychological problems for ICU survivors, in the months and years following hospital discharge.8–13 While risk factors for PICS are increasingly described, there have been few interventions to prevent PICS, and no interventions to treat PICS have demonstrated unequivocal positive benefits.14–20
While population-level data on ICU-associated disruptions of some medications are available, few data are available to understand what specific problems ICU patients have with their medications after discharge home, and how consequential those might be. Only a single-centre study is available from the American health system; no data are available from integrated health systems such as the National Health Service.21 The purposes of this study, therefore, were to: determine specific medication-related problems among survivors of ICU; explore the changes made by a pharmacist in this context; and examine the potential risk factors for pharmacist-correctable medication errors.
Methods
Consecutive patients enrolled in a post-ICU programme between September 2014 and June 2015 were evaluated by a pharmacist as a part of that programme. This evaluation focuses on a pharmacy intervention set in the post-ICU follow-up clinic.
Patients were drawn from a 20-bed mixed surgical/medical critical care unit in Glasgow Royal Infirmary (GRI). GRI is a tertiary referral centre for burns and pancreatic care. This pharmacy intervention was undertaken during a 5-week programme for ICU patients and their caregivers. Intensive Care Syndrome: Promoting Independence and Return to Employment (InS:PIRE) is a multidisciplinary, peer-supported, rehabilitation programme. Participants of working age (18–64) were invited to take part between 6 and 20 weeks after hospital discharge. However, there were some participants who had been discharged for longer (up to 3 years) who requested to take part in the programme. Caregivers were also encouraged to attend with patients. Patients were eligible for the InS:PIRE programme if they received mechanical ventilation for greater than 72 hours or had a high dependency unit stay of greater than 2 weeks. The InS:PIRE programme involved individual sessions for patients and their caregivers with a pharmacist and physiotherapist along with interventions from medical, nursing, psychology and community services. A full description of the InS:PIRE intervention and the outcomes of this complex intervention pilot have been published previously.22 23
The local Caldecott Guardian also reviewed the proposal (Clinical Governance structure within the UK). Data were collected between September 2014 and June 2015. We used the Standards for Quality Improvement Reporting Excellence 2.0 to structure reporting (online supplementary material S1).24
Supplemental material
Patient and public involvement
To ensure that this intervention was person centred and appropriate for the population, the team held a Patient and Family Advisory Council which fed directly into the programme. Ten to 12 patients and caregivers met every 2 weeks for a year and coproduced the service with the staff involved in InS:PIRE. The Council looked at all aspects of the programme including the content and outcome measures used. All results of the study have been disseminated to patients and caregivers during a patient and family day which was held within our ICU. If participants requested, written results were also available.
Measures
Pharmacy intervention
During the ICU follow-up programme (InS:PIRE) a full medication review was performed by the pharmacist. This included: medicines reconciliation, assessing the appropriateness of each of the prescribed medications, identification of any medication-related problems and checking adherence. The pharmacist recorded the patient’s prescribed medication prior to their admission to ICU, on discharge from ICU and at hospital discharge, and compared this with the medication prescribed when the patient attended InS:PIRE. Data for the above were available to the pharmacist from the hospital’s electronic healthcare system, primary care prescription information, patient, caregiver (if present) and community pharmacist if appropriate. All patients had medicines reconciliation performed within 24 hours of admission to the ICU; these data were also available to the pharmacist reviewing the patient. Patients were generally seen between week 1 and week 3 of InS:PIRE. However, if required, patients could be seen on more than one occasion (usually for safety reasons).
Medication-related problems which were identified during the pharmacy review were categorised according to the Hepler and Strand framework.25 This framework includes: clarification of any drug omissions, drug dose adjustment if necessary (according to disease severity, clinical guidelines and adverse effects), review of the duration of a drug treatment, new drug recommendations, education regarding a specific drug to enhance efficacy or improve safety, review of any incorrect or ineffective drugs prescribed and, lastly, an adverse drug reaction report if appropriate.24 For the purpose of analysis, we categorised drugs according to the British National Formulary classification.26
All the interventions were classified by the primary pharmacist at the InS:PIRE clinic. This review was then externally validated by a senior pharmacist in the acute hospital setting. There were a small number of discrepancies (n=4) regarding the potential significance of the interventions. These were discussed, and an outcome agreed between the two reviewers.
The significance of the interventions was classified on a severity scale of 1–5. This scoring system was adapted from the National Patient Safety Agency Risk Matrix.27 A score of 1 indicates an intervention that is not likely to be of clinically significant impact and a score of 5 indicates an intervention which could potentially prevent an organ or life-threatening event (table 1). Clinical examples of different levels of severity are reported in online supplementary material S2.
Supplemental material
Intervention severity scale
Patients and their caregivers were asked if they were given enough information about their medication during their hospital stay and if they were made aware of the changes that had been made when they were discharged from hospital. They were also asked if they had any concerns about their medication. Finally, patients were asked if they would like a Medication Passport as a record of their current medication. Individualised, patient-held medication records have been used in specific patient groups, such as palliative care and diabetes, and have been shown to help support self-management, adherence, and improve communication surrounding the patient’s mediation.28 29 The Medication Passport (http://clahrc-northwestlondon.nihr.ac.uk/resources/mmp) which was designed by patients has been found to be a useful tool when initiating conversations with healthcare professionals.30
Demographic measures
To understand comorbidities and their impact in this group, the Charlson Comorbidity Index, which is a method of categorising comorbidities of patients based on the International Classification of Diseases, was used.31
The Scottish Index of Multiple Deprivation (SIMD) is the Scottish Government’s tool for identifying those geographical areas in Scotland suffering from deprivation. Within a research context, the SIMD data are split into quintiles, deciles or vintiles. For the purpose of this evaluation, deciles were used, with decile 1 being the most deprived and decile 10 being the most affluent.32
Statistical analysis
We reported the total number of specific medication problems at different time points in the patient journey. Logistic regression using the statistical package R (V.3.3.0)33 was performed to determine if age, ICU length of stay, Acute Physiology and Chronic Health Evaluation II (APACHE II) score, requiring cardiovascular support, renal replacement therapy and number of medicines on admission or ICU discharge were associated with the number or severity of medication-related problems. We also examined the influence of comorbidities and deprivation on the number and severity of medication-related problems using the Charlson Comorbidity Index and the SIMD. Finally, as the most common drugs requiring an intervention were those associated with respiratory, cardiovascular and pain medications, we examined whether being prescribed these classes of medication was predictive of a medication-related problem or severity of the problem.
Results
Patients
Eighty-nine patients were invited to attend InS:PIRE, 49 (55% of those invited) attended over the 1-year evaluation. Forty-seven were reviewed by the pharmacist. The two patients who did not receive the pharmacy intervention did not attend the week it was due. Baseline demographics for the patients who received the pharmacy intervention are shown in table 2. The median age of those who received the pharmacy intervention was 52 years (IQR 43–57), with a median APACHE II score of 23.19–27
Baseline demographics for patients who were reviewed by the pharmacist
Medications prescribed
The median number of pharmacy interventions per patient was 1 (IQR 1–2). The median number of drugs prescribed per patient before their ICU admission was 6 (IQR 2–9). The median number of drugs prescribed per patient at ICU discharge was 6 (IQR 4–8); this increased to 7 (IQR 4–10) at hospital discharge. At the InS:PIRE clinic the median number of drugs each patient was prescribed had increased to 8 (IQR 5–11).
Changes to medication
Of the 47 patients, 26 (55%) reported that they were not made aware of changes to their medication when they were discharged from hospital, 28 (60%) of patients had concerns about their medicines at their clinic visit and 34 (49%) patients requested a Medication Passport.
Medication-related problems
Medication-related problems were identified in 38 (81%) of the 47 patients. Medication-related problems were identified with 69 (18.6%) of the medications patients were prescribed at the time of the pharmacy intervention. The most common documented problem was drug omissions accounting for 20 (29%) of the 69 identified (figure 1). This was followed by a suggested dosage adjustment on 13 (19%) occasions then duration of treatment clarification 12 (17%) times. The potential significance of these problems was classified by the InS:PIRE pharmacist. Forty-four (64%) of the medication-related problems were classified as severity score ≥3 (figure 2). The classes of drugs most commonly associated with requiring an intervention were cardiovascular 18 (26%), analgesic 15 (22%) and respiratory medicines 7 (10%). The medication-related problems identified by the pharmacists were also shared with the wider multidisciplinary team.
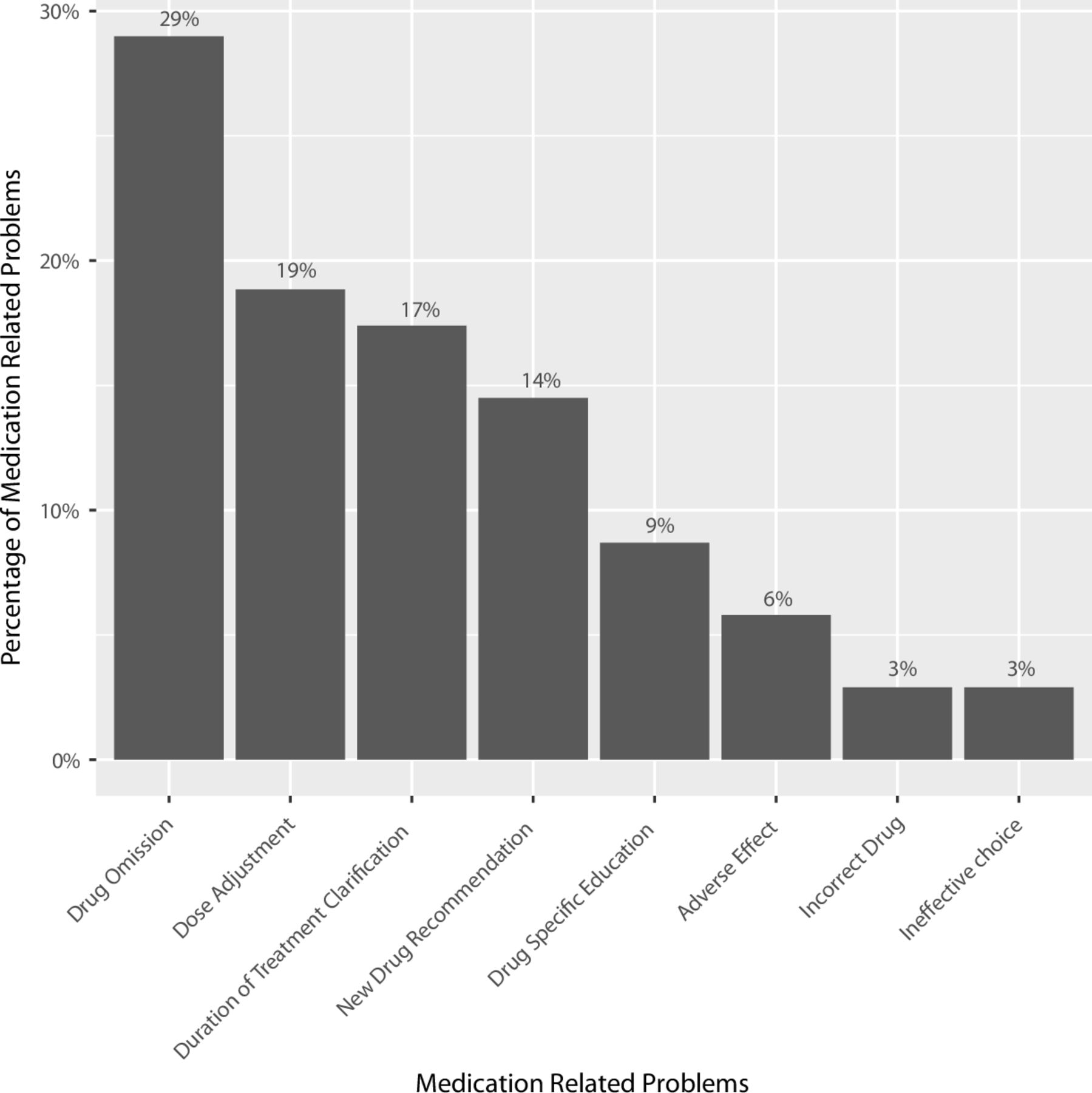
Incidence of medication-related problems.
{kind=link}
{kind=link}
Severity of medication-related problems.
Predicting patients most at need
We predicted two sets of events: one examining if a patient had a medication-related problem, then second if a patient had a medication problem of severity ≥3 (clinically significant). Patient demographics such as gender, age, ICU length of stay, APACHE II score, number of home medications prior to ICU admission, receiving renal replacement therapy or cardiovascular support, number of medications prescribed at ICU discharge and, more specifically, the number of cardiovascular, analgesic or respiratory medications prescribed at ICU discharge and none were significantly associated with the presence of any medication-related problem (table 3).
Logistic regression results
The only factor predictive of a clinically significant medication-related problem (severity ≥3; OR 2.02, 95% CI 1.14 to 4.26, p=0.03) was the number of pain medications prescribed at discharge from ICU (table 3).
Discussion
In this cohort study of consecutive patients seen in a post-ICU programme, medication-related problems following an ICU admission were common, occurring in 81% of the patients studied. Of the interventions undertaken, just under two-thirds were likely to improve therapeutic benefit or avoid serious side effects. The pharmacist identified medication-related problems with 18.6% of the total medications reviewed at InS:PIRE. This is similar to the rate (16.1%) of medication-related problems identified in a recent UK study by pharmacists working within an ICU.34 We found the approach to identifying medication-related problems feasible and would recommend its adoption more widely in ICU follow-up clinics.
The most common medication-related problem found was omission of medicines for chronic disease states, which were withheld during the patient’s hospital stay and had not been restarted at their clinic review. This aligns with previous studies which have found that an ICU admission is associated with an increased risk of unintentional discontinuation of long-term medications.1–3 In one study, discontinuation of a statin or antiplatelet medication showed an increased risk of death, hospital admission and emergency department visit up to 1 year after hospital discharge.1 Medications commenced in ICU were also found to have been continued unnecessarily which is also consistent with previous studies.4 5
In this evaluation, 60% of patients reported they had concerns about their prescribed medication. Patient’s beliefs about their treatment influence their engagement and adherence with their management; concerns about their medicines can lead to intentional non-adherence and subsequent treatment failure.35 36 This is a modifiable problem. These concerns can be addressed; patients can be supported to make informed choices about their medicines using tools such as the Medication Passport. Such pharmacist engagement could improve mental health and emotional problems such as anxiety following critical care discharge for patients, by encouraging participants to be more engaged in their health.37 Given the challenges of resourcing such interventions in cost-restrained healthcare environment, the reduction in medication-related problems may help with long-term sustainable funding. More work is required to understand the overall impact of the intervention on patient safety and healthcare utilisation.
No single risk factor strongly differentiated patients who might benefit from a pharmacy intervention in this small study. However, it appears that patients who are on pain medications at ICU discharge are at particular risk of needing pharmacy input in the ICU recovery period. This risk factor is quite common, with chronic pain being reported in 44% of ICU survivors.38 Further work is needed to identify potential post-ICU clinic patients at greatest risk of medication-related problems, or conversely those who do not need the expertise of a pharmacist.
Strengths of this evaluation include its systematic approach to understanding pharmacy interventions and its rigour in categorising medication use, at all points in the patient journey. Limitations include that it was undertaken in a single centre with a small sample of patients. More work is required across a number of centres to understand if this is a problem isolated from this particular centre. We did not have data on those patients who did not attend the ICU follow-up programme. It is not clear whether patients attended because of pharmacy issues, therefore, these findings may not be representative of the entire population. Finally, patients were also seen at a variety of time points after ICU, which may have influenced the reported findings.
Conclusion
Medication problems are common following critical care. This study demonstrated that the number of pain medications prescribed at discharge from intensive care was significantly predictive of medication-related problems. In the absence of highly effective communication, a pharmacy intervention may contribute substantially to an intensive care rehabilitation or recovery programme. A further multicentre study is required to test changes in longer term patient or system-centred outcomes.
Acknowledgments
The authors thank all the patients involved in this evaluation and all staff in the InS:PIRE clinic.
References
Footnotes
Twitter @@pamelamactavish, @@jomcpeake22
Contributors Evaluation design: PM, CF, JM, TQ. Data collection: TQ, PM, RK, JM, HD. Data analysis: PM, JM, MS, TJI. Writing of article: all authors. Final review of article: all authors.
Funding PM, HD, TQ, JK, MD and JM were funded from the Health Foundation (UK) when undertaking this work. JM was funded by the CNO (Scotland). TJI's work was supported, in part, by the US Department of Veterans Affairs, Health Services Research and Development (IIR 13-079).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This evaluation was undertaken as part of a service evaluation initiative within the ICU. Ethics approval was sought and waived by our hospital research and development department as this was deemed to be a quality improvement initiative. Data were collected between September 2014 and June 2015.
Provenance and peer review Not commissioned; externally peer reviewed.