Article Text

Abstract
Background Changes are often made to medications at times of transitions in care. Inadequate reconciliation during admission, transfer and discharge causes medication errors and increases risks of patient harm. Despite well-established multidisciplinary medicines reconciliation (MR) processes at hospital admission, our MR process at discharge; however, was poor. The main errors included failure to recommence withheld medicines and lack of documentation explaining changes made to medications on discharge. Our objective was to develop an intervention that supports prescribers to follow a simple standardised MR process at discharge to reduce these errors.
Methods Working closely as a multidisciplinary team, we used improvement methodologies to design and test a process that reliably directs prescribers in surgery to use the inpatient prescribing chart as well as the MR on admission form as sources to create accurate discharge prescriptions. The project was segmented into testing, implementation, spread and sustainability.
Results The tested intervention helped the accuracy of discharge prescriptions steadily and quickly improve from 45% to 96% in the pilot ward. Following the successful implementation and sustainability in two separate pilot wards, the intervention was spread to the remaining eight wards producing a similar improvement.
Conclusions To improve patient safety, it is crucial to ensure that information about medicines is effectively communicated when care is transferred between teams. Although this can be challenging, we’ve shown that it can be done effectively and reliably if this responsibility is equally shared by healthcare professionals from all disciplines while being supported by safe systems that make it easy to do the right thing. Successfully implementing a standardised multidisciplinary MR process at discharge can also reduce the reliance on pharmacists therefore freeing them to undertake other clinical roles.
- medication reconciliation
- medication safety
- pharmacists
- quality improvement
- surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Defining the problem
Patients often receive new medications or have changes made to their existing medications at times of transitions in care. Although most of these changes are intentional,1 there is a substantial body of evidence that shows that when patients move between care providers there is a significant risk of miscommunication and unintended changes to medicines.2 Some reports have estimated that between 30 and 70 per cent of patients have either an error or an unintentional change to their medicines when their care is transferred.3 This inadequate reconciliation of patients’ medication information in transfer of care during admission, transfer and discharge causes significant medication errors4 which increase the risk of patient harm and puts an economic burden on health services.5 6 Although much work has been done and published in Scotland regarding improving medicines reconciliation (MR) on admission to hospitals, mainly as a result of the Scottish Patient Safety Programme which since its launch in 2008 had a very clear focus on improving MR across all care boundaries,7 very little work seems to have been done however in regards to MR on hospital discharge. It has been estimated that patients that have one or more medicines changed at the point of discharge have a 4.4% increased risk of an adverse drug event postdischarge.8 9 Patients with unintentionally omitted medicines on discharge have a much higher risk of an adverse drug event with 2.31 times the usual risk of readmission to hospital.10 It is also estimated that the likelihood that an elderly patient being discharged on the same medicines that they were admitted on is less than 10%11 meaning that patients over the age of 65 years and those who take several medicines have a significantly increased risk of medication errors.5 This is not a surprise considering that 28%–40% of medicines get discontinued during hospitalisation12 and 45% of medicines prescribed at discharge are new medicines.13
As members of the multidisciplinary team, ward based clinical pharmacists have always played a key role in improving the safety and quality of care delivered to patients through safer use of medicines. In our health board, one of the roles of the pharmacists is to review all the discharge prescriptions for clinical appropriateness and accuracy before sending them to the dispensary for dispensing and supply of any required medication. Despite having a well-established multidisciplinary MR process at admission, the anecdotal yet consistent feedback from the surgical pharmacists was that the MR process at discharge, reflected in the accuracy of the discharge prescriptions written by the junior doctors, was poor. The main errors identified by the pharmacists during their clinical review process were a combination of failure to recommence withheld medicines and lack of clear documentation explaining the clinical reasoning behind any medications stopped, changed or started during the current hospital admission. This practice was not only increasing the risk of harm because of the multiple prescribing errors but also causing significant waste because of unnecessary delays in patient discharge due to the additional time required by the pharmacists to amend these errors.
Background
Medicines reconciliation (MR), or ‘Med Rec’ as it has come to be known, is a formal process for identifying and correcting unintended medication discrepancies across transitions of care and is now widely endorsed and mandated by many healthcare regulatory bodies as an important component of patient safety.6 MR aims to eliminate undocumented intentional discrepancies and unintentional discrepancies in a patient medication history, at all interfaces of care, by encouraging the clinicians to follow a standardised process that ensures a comprehensive medication history is obtained and is verified by more than one source. The verified information is then transferred to the next care provider and also given to the patient or carer. At least two sources of information should be used to obtain and verify the information, one of them being the patient, whenever possible, especially at the point of admission. Engaging the patient is one of the best strategies to ensure a patient-centred approach to MR and also prevent errors. Numerous studies and large-scale national initiatives have shown that MR significantly reduces medication errors and adverse events.5
With 60% of patients having three or more medicines changed during their hospital stay,8 the aim of MR on discharge is therefore to communicate a complete list of the patient’s medication to the next care provider when a patient is referred or transferred to another setting outside the organisation1 in order to improve patient safety and contribute to a reduction in avoidable medicines-related admissions and readmissions to hospital.2
Implementing a formalised MR process at discharge can significantly reduce prescribing errors including inadvertent omission of therapy, failure to recommence withheld medicines and duplication of therapy after discharge.5 This is achieved by encouraging clinicians to follow a standardised process that ensures that at the end of each episode of care a comprehensive medication history is obtained that includes a thorough history of all regular medications used and any changes made to the medicines during this episode of care. The information is then verified and transferred to the next care provider and also given to the patient or carer. This process is based on the safety principle of independent redundancies—having independent checks, generally by different providers, for key steps in the process.14
Aim
The primary aim of this project was to improve the quality and safety of the discharge communications produced by junior doctors when surgical patients are transferred from secondary care back to primary care. This was achieved by ensuring a standardised process was in place to support the junior doctors produce discharge prescriptions that provided both an accurate list of medications that are clinically appropriate for the patient at the point of discharge and also clear documentation explaining the clinical reasoning behind any medications stopped, changed or started during the current hospital admission.
Methodology
Context
The surgical department at Ninewells University and Teaching Hospital has 10 wards and more than 260 inpatient beds. This covers a range of disciplines including urology, upper and lower gastrointestinal surgery, vascular surgery and orthopaedics and has a team of six pharmacists and two pharmacy technicians who are well integrated into the multidisciplinary team to provide patient-centred, safe and effective pharmaceutical care. Within our board, medications from a paper-based inpatient prescribing and administration chart are transcribed by the discharging junior doctor to an electronic system to populate a discharge document. Pharmacists then check these electronic discharge prescriptions to ensure that the medication section is both accurate and clinically appropriate before releasing the discharge document to the dispensary for the dispensing and supply of any medication required by the patient prior to leaving the hospital. Once the patient is discharged, the record is locked and transferred electronically to the patient’s general practitioner (GP) and also made available to the rest of the primary care team, including the patient’s community pharmacist, via remote access to a central clinical portal.
The quality improvement project was initially conducted on the 30-bed upper gastrointestinal surgery ward from October 2013 to June 2014, before being spread to the other wards.
The ward is covered by three junior doctors who rotate every 4 months starting from August each year and one permanent clinical pharmacist who is also responsible for providing care to two other surgical wards. The pharmacist provided clinical services to the ward only during the working hours of a traditional working week; Monday to Friday 08:00–16:00.
Baseline measurement
The concerns raised by the ward pharmacists regarding the inaccuracy of MR on discharge, led to a 4-week prospective audit of all discharge prescriptions in the upper gastrointestinal surgery ward to explore the validity of this anecdotal feedback and help quantify the problem. The audit revealed that 55% of the discharge prescriptions clinically reviewed by the pharmacist during their working hours of the audit period were deemed inaccurate, requiring one or more amendments by the pharmacist before sending to the dispensary for dispensing. The main errors identified were a combination of failure to recommence withheld medicines and lack of clear documentation explaining the clinical reasoning behind any medications stopped, changed or started during the current hospital admission (figure 1).
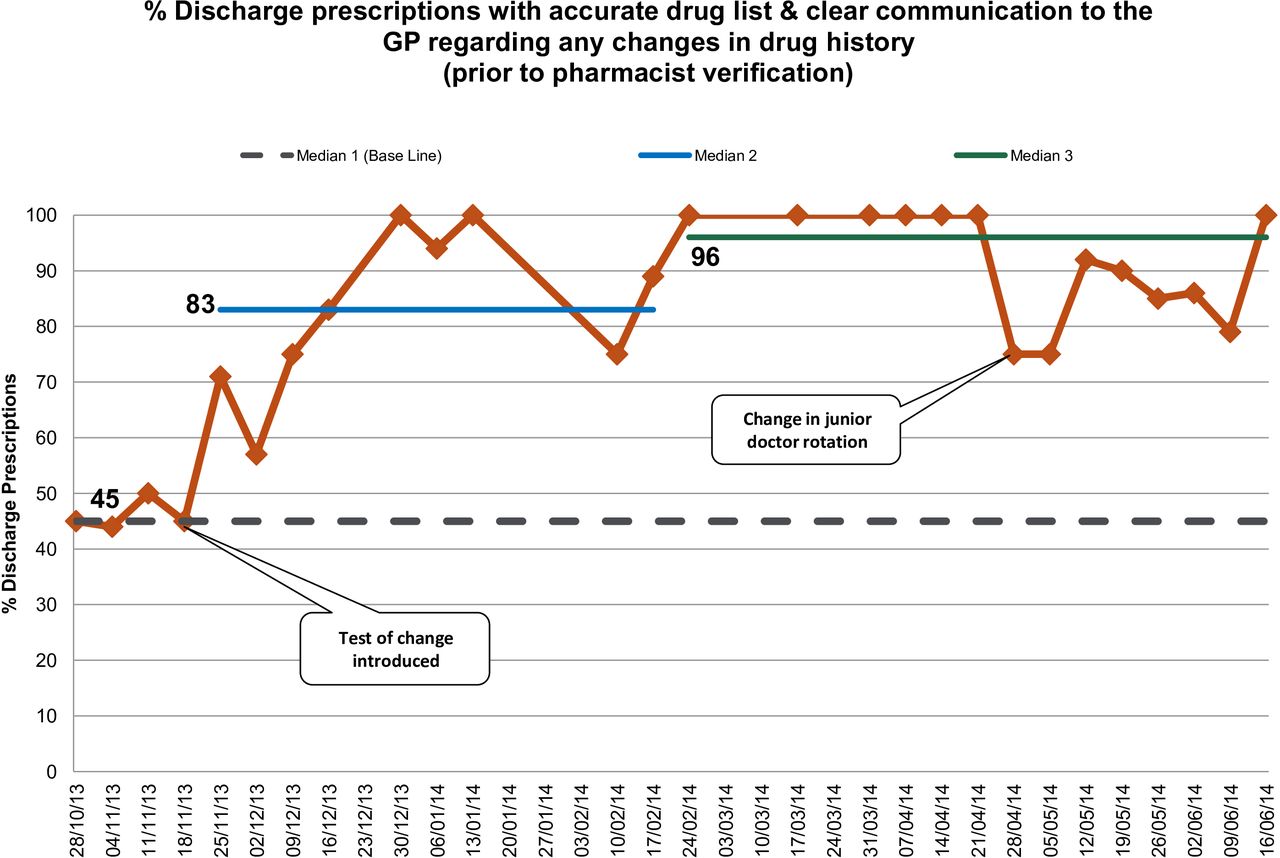
Percentage of discharge prescriptions with accurate drug list and clear communication to the general practitioner regarding any changes in drug history (prior to pharmacist verification). Run chart showing that once the intervention was introduced following the 4-week base-line period, the accuracy of discharge prescriptions steadily and quickly improved from 45% to reach a median of 83% for the first 3 months and continued to improve further to a median of 96% by the end of the 8 months of this first stage of the project.
Rationale
Our local MR policy clearly describes the standardised process that should be followed by the junior doctors in order to produce an accurate discharge prescription. This process requires the prescriber to reconcile the medicines the patient was taking prior to hospital admission, which is documented on the patient’s MR on admission form as part of their hard copy medical notes, and those medicines currently prescribed for them to use while in hospital on their inpatient prescribing and administration hard copy chart. Although the policy and its contents are routinely shared with all the junior doctors as part of their initial induction process when they start their surgical rotation block, the collective experience by the ward pharmacists is that this standardised process is not adhered to by many of the junior doctors. This was supported by feedback from the junior doctors on the pilot ward when asked, as part of this project, to describe the process they would follow to produce a discharge prescription. Two of the three junior doctors described a process where only the inpatient prescribing and administration chart is used as a source of information to populate the contents of the discharge prescription while the third said that he would sometimes refer back to the MR on admission forms. This practice would explain why one of the main errors identified during the base line data collection was failure to recommence withheld medicines.
Our objective was therefore to design, test and implement an intervention that would support the junior doctors comply with the requirements of the local MR policy and use both the inpatient prescribing and administration chart as well as the MR on admission form as sources of information to create an accurate discharge prescription.
The project’s aim was that by June 2014, 90% or more of the patients whose discharge prescriptions are reviewed by the ward pharmacist during their working week would contain an accurate list of medicines and clear communication to the GP regarding any changes in medication history, prior to any pharmacist input. A 90% aim, rather the usual 95%, was chosen because it was acknowledged by the team that this intervention would not prevent transcribing errors. Because it would be difficult to identify and exclude transcribing errors during data collection, it was therefore agreed that could be better accommodated for at the aim setting stage.
Improvement
Working closely with the junior doctors, we used the improvement methodologies15 to design and test the following process as a test-of-change following sequential plan-do-study-act (PDSA) cycles:
New patients admitted by medical team have their medicines reconciled and documented on the MR on admission form at point of admission as per current practice.
Ward pharmacist reviews the patient’s MR on admission form to verify the contents, as per current practice, and also attaches a green sticker to the MR form (figure 2). This green sticker will need to be completed by the doctor at the point of discharge.
At the point of discharge, the doctor will refer back to the patient’s medicine reconciliation on admission form as a source of information to help populate the contents of the discharge prescription alongside the inpatient prescription and administration chart as per local policy.
The doctors will annotate the green sticker attached to the MR on admission form to confirm that they have
Reviewed the patient’s list of medicines on admission and used it as a source to reconcile the contents of the discharge prescription.
Clearly communicated any changes in the patient’s medication history to the GP in the discharge document.
Discussed the contents of the discharge prescription with the patient.
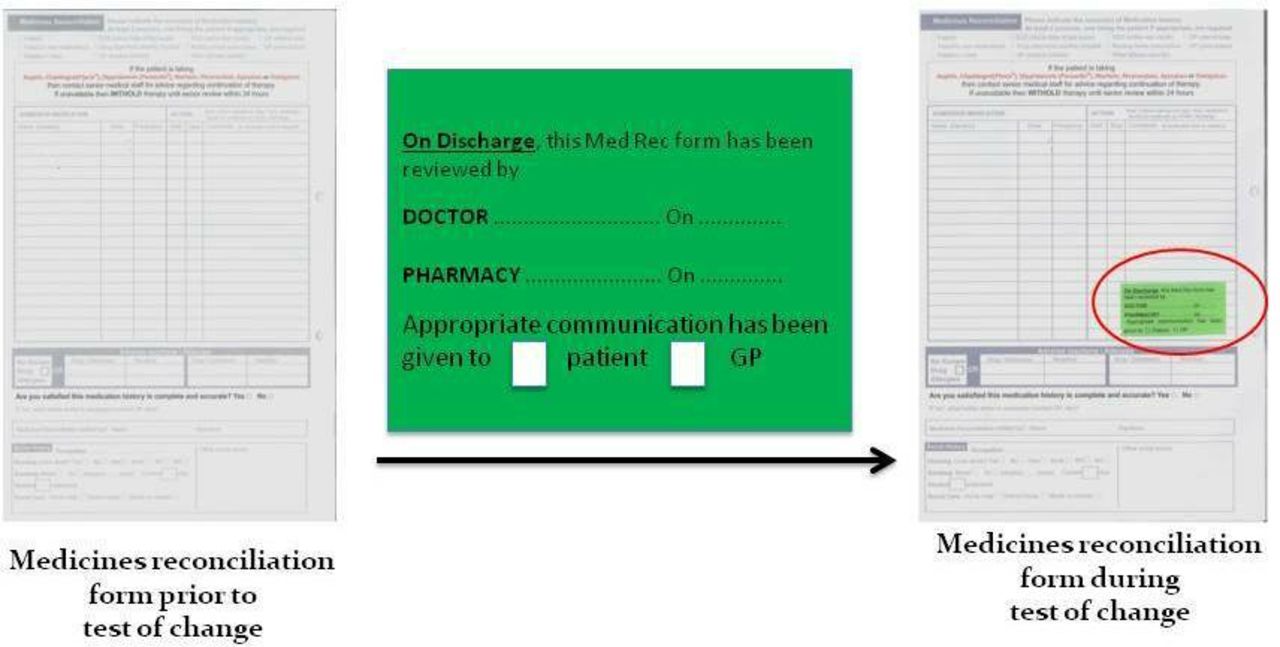
A diagrammatic representation showing the different elements of the sticker that was used as an intervention in the test of change and how it was attached by the ward pharmacists to the patients’ medicines reconciliation on admission forms on verification.
A data collection form was designed and tested using sequential PDSA cycles as part of this project. The data were collected prospectively and presented as run-charts displaying the accuracy of discharge prescriptions over the time period of this project.
Measures
The primary measure for our improvement work was the outcome measure of Percentage of discharge prescriptions with accurate medication list and also clear communication to the general practitioner regarding any changes in medication history prior to any pharmacy input. These discharge prescriptions, when clinically reviewed by the pharmacist as part of the verification step of the MR on discharge process, were considered accurate and not requiring any amendments by the pharmacist. A secondary, and relatively crude, outcome measure was the time taken by the pharmacists to clinically review a discharge prescription in order to complete the MR on discharge process. This data were collected prospectively by the pharmacists as they completed the clinical review process and was also confirmed retrospectively using our electronic discharge document systems.
Discharge prescriptions were included for data collection if the discharge prescription was being screened by the pharmacist at ward level and the patient’s MR on admission form was reviewed by a pharmacist earlier in the admission and had a green sticker attached. This way any inaccuracies in the content of the discharge prescription could be linked to a failure in the process rather than potential errors transcribed from an incomplete MR on admission form. No sampling methodologies were used in the data collection process because all eligible discharge prescriptions were included for review and analysis.
The process measure for this project, which was hypothesised to drive the above outcome measure in the positive direction, is how often the junior doctors completed the green stickers as part of their MR on discharge process therefore ensuring that both the inpatient prescribing and administration chart and the MR form on admission were used as sources to populate the contents of the discharge prescription. To ensure 100% compliance with this process, it was agreed with the junior doctors at the outset of the project that the pharmacist would refer any unannotated green stickers back to the relevant prescribers for review and completion before any discharge prescriptions could be clinically reviewed or verified by the pharmacists (figure 3).

A flow chart describing the process agreed and implemented by the multidisciplinary team as part of this project to ensure complete compliance with the process measure that was hypothesised to drive the outcome measure in the positive direction.
Results
Base line data collected during the first 4 weeks of this project showed that only 45% of the discharge prescriptions clinically reviewed by the pharmacist during their working hours of the audit period were deemed accurate and not requiring any amendments before sending to the dispensary for dispensing (figure 1). The errors identified on these prescriptions were a combination of inaccurate list of medicines and multiple gaps in communication to GPs regarding changes in medication histories. Just over 61% of the prescriptions had an accurate list of medicines (figure 4) and the biggest gap in communication was regarding medicines being intentionally discontinued and the absence of clinical reasoning behind that (figure 5). Figure 1 shows that once the intervention was introduced following the 4-week base-line period, the accuracy of discharge prescriptions steadily and quickly improved to reach a median of 83% for the first 3 months and it continued to improve further to a median of 96% by the end of the 8 months of this first stage of the project.

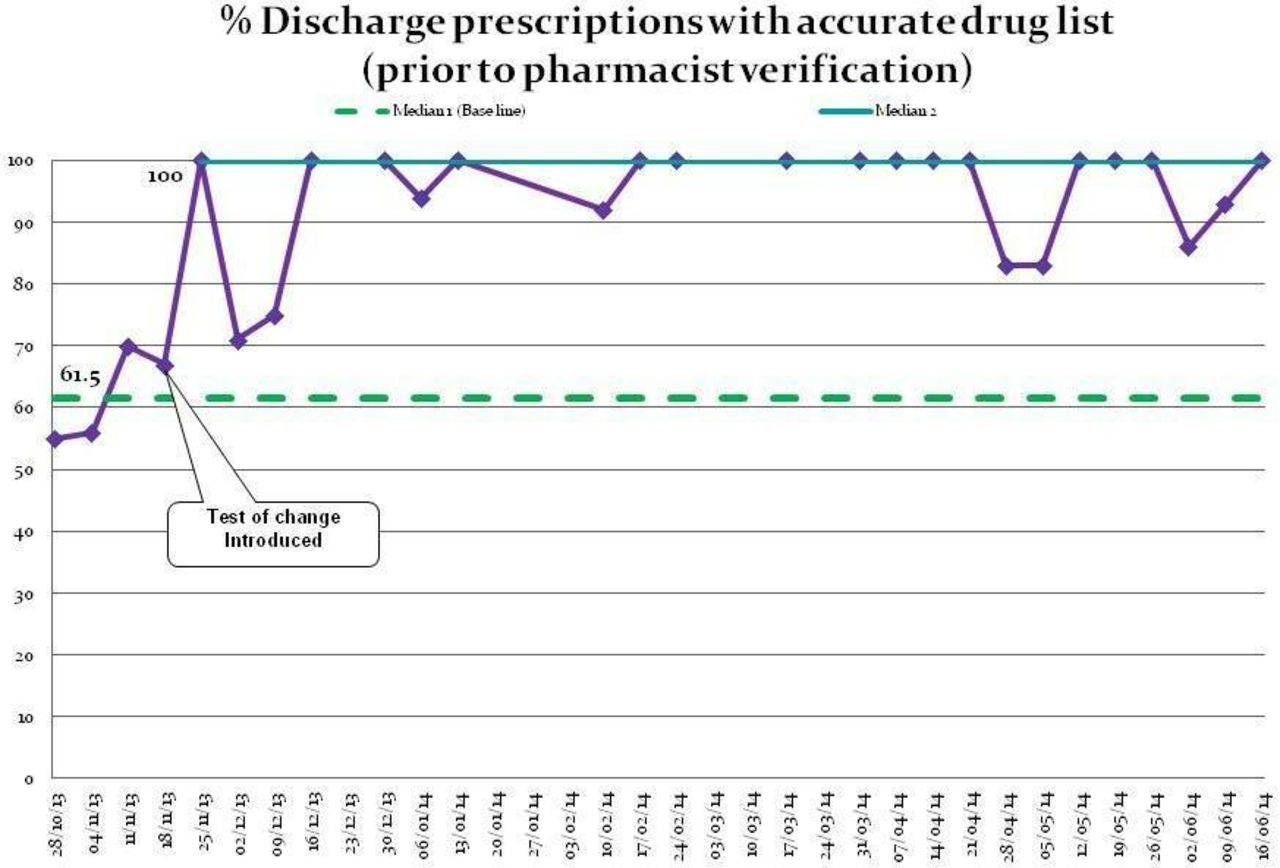
Percentage of discharge prescriptions with accurate drug list (prior to pharmacist verification). Run chart showing how the new process supported the improved accuracy of discharge prescriptions by increasing the percentage of patients with an accurate list of discharge medications from a base line of 61.5% to a median greater than 95% within the first 6 weeks of the project.

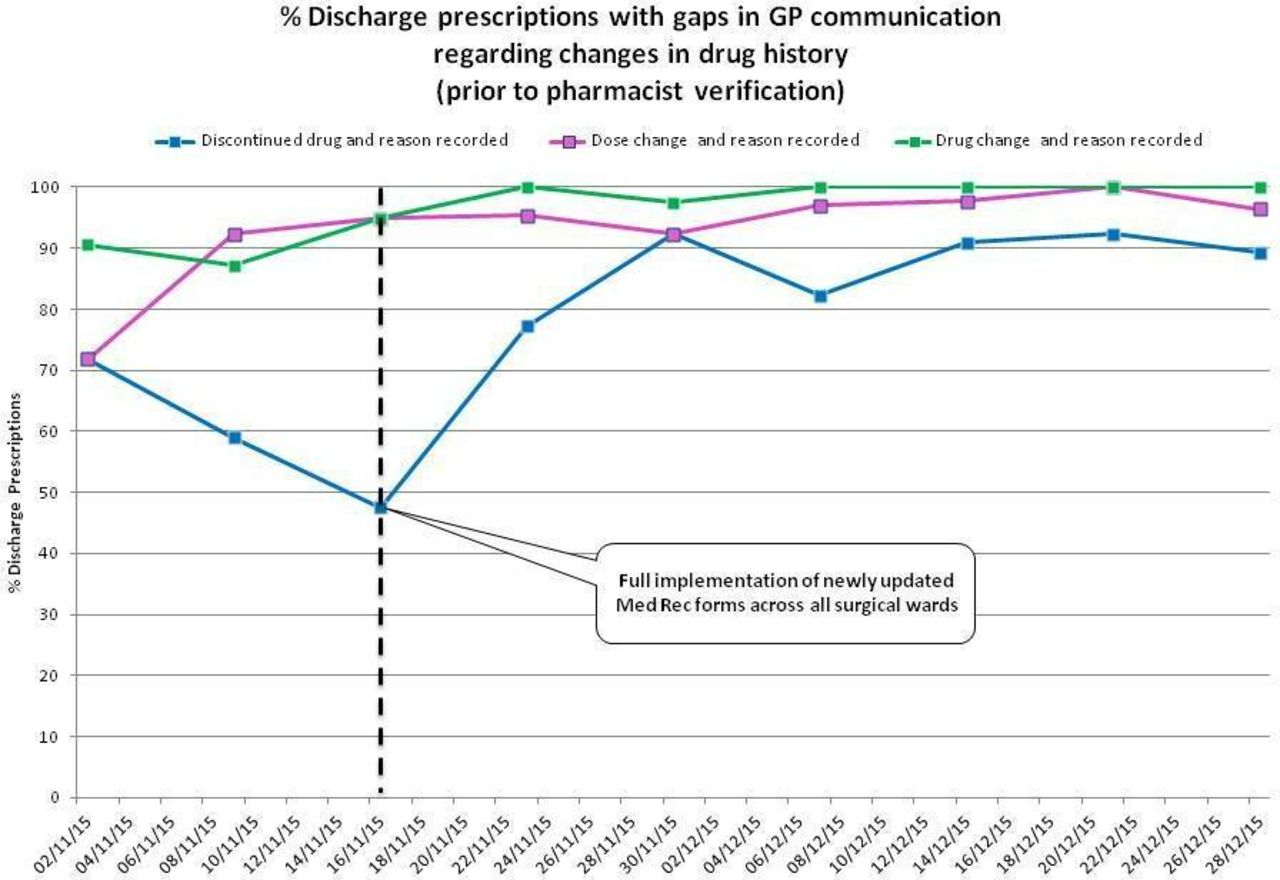
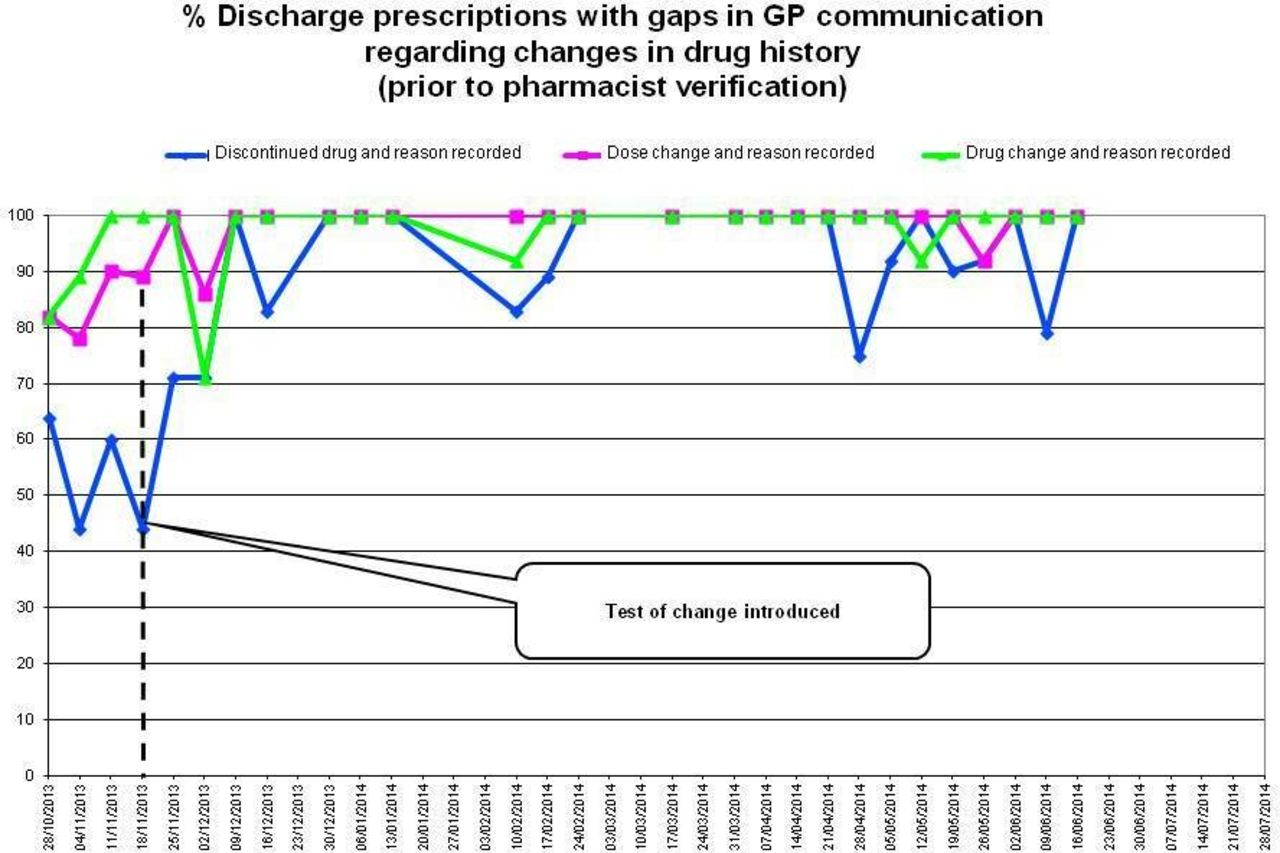
Percentage of discharge prescriptions with gaps in general practitioner (GP) communication regarding changes in drug history (prior to pharmacist verification). Chart showing that prior to this project, the biggest gap in discharge prescription communication was regarding medicines being intentionally discontinued and the absence of clinical reasoning behind that. This chart also shows how the new process supported the junior doctors increase the percentage of patients with clearly communicated changes regarding their medication history to their GP as part of the discharge document.
The new process supported the improved accuracy of discharge prescriptions by increasing the percentage of patients with an accurate list of discharge medication from a base line of 61.5% to a median greater than 95% within the first 6 weeks of the project (figure 4), while also supporting the junior doctors increase the percentage of patients with clearly communicated changes regarding their medication history to their GP as part of the discharge document (figure 5).
It can also be seen from figure 1 that after 3 weeks of the introduction of the new process the accuracy of the discharge prescriptions was improved and maintained above 80% for 17 out of the 20-week duration of the project with six consecutive weeks where the accuracy was maintained at 100%.
A total of 37 discharges were included in the audit over the initial 4-week base-line period averaging nine discharges per week, while a further 191 discharges were included in the audit over the remaining 7 months period maintaining a similar average of seven discharges per week.
Stage 2: Spread
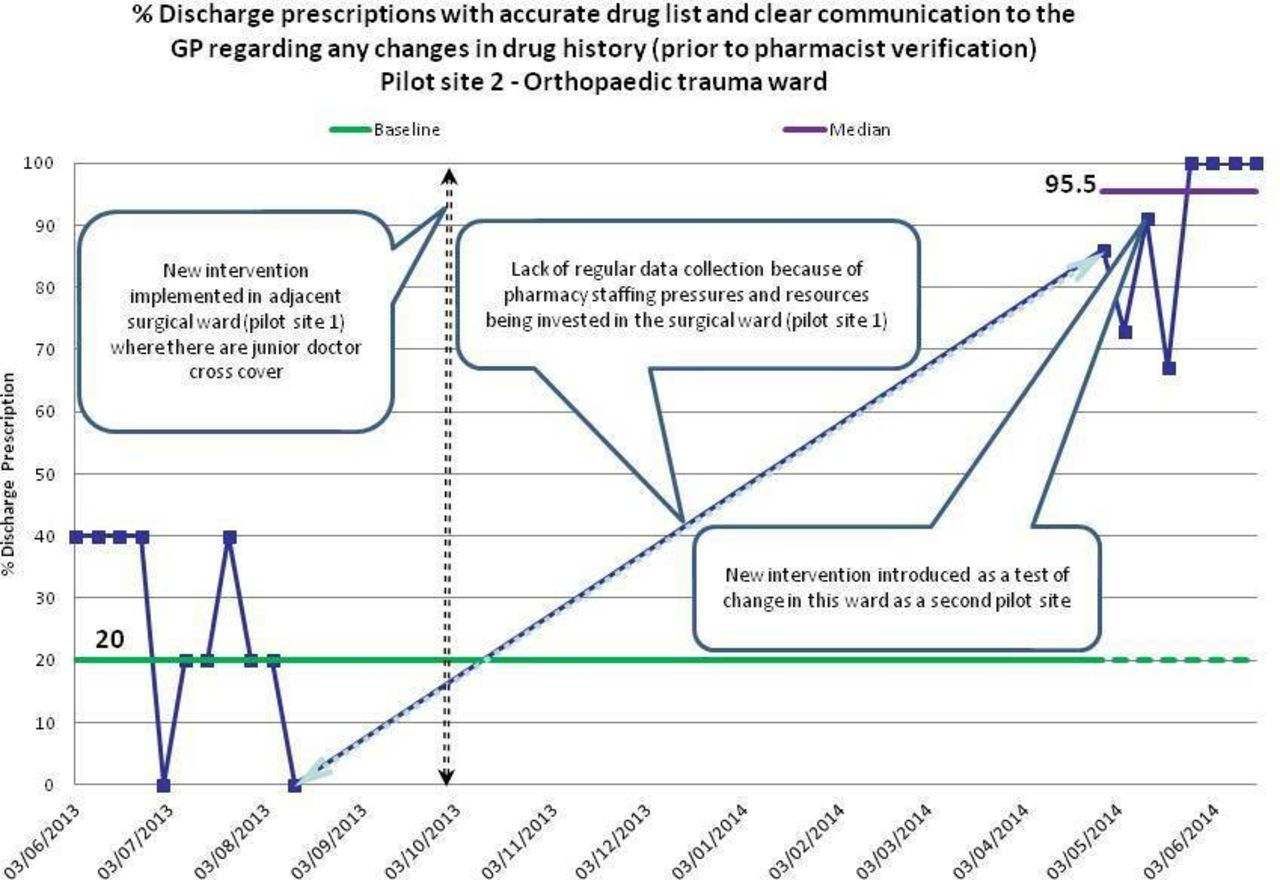
After a total of 7 months of successful implementation and sustainable results in the surgical pilot ward, the project was replicated in one of the trauma orthopaedic surgery wards to evaluate the impact of this intervention out with the pilot ward. Despite the lack of a complete data set from the second orthopaedic pilot ward due to staffing shortages, the results in figure 6; however, displayed a very similar pattern to that observed in the surgical pilot site, where the base line accuracy of discharges in the orthopaedic ward was 20% and that increased and was sustained at levels above 95% after the implementation of the new intervention in the surgical ward initially followed by the orthopaedic ward, respectively.
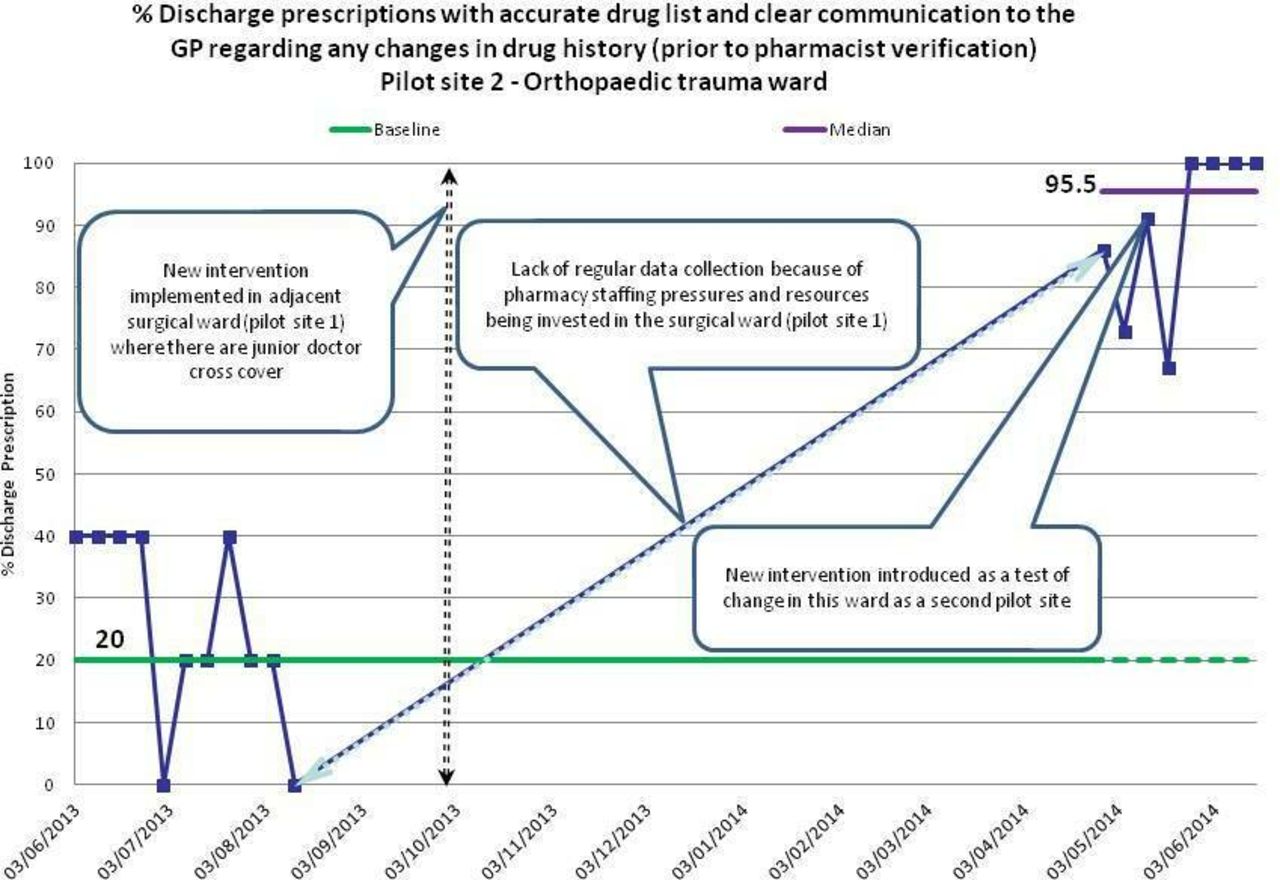
Percentage of discharge prescriptions with accurate drug list and clear communication to the general practitioner regarding any changes in drug history (prior to pharmacist verification). Pilot site 2: Orthopaedic Trauma ward. Run chart showing how the orthopaedic ward as a second pilot site displayed a very similar pattern to that observed in the first surgical pilot site, where the base line accuracy of discharges was low at 20% and then increased and was sustained at levels above 95% after the implementation of the new intervention in the adjacent surgical ward initially before full implementation in the orthopaedic ward at a later stage.
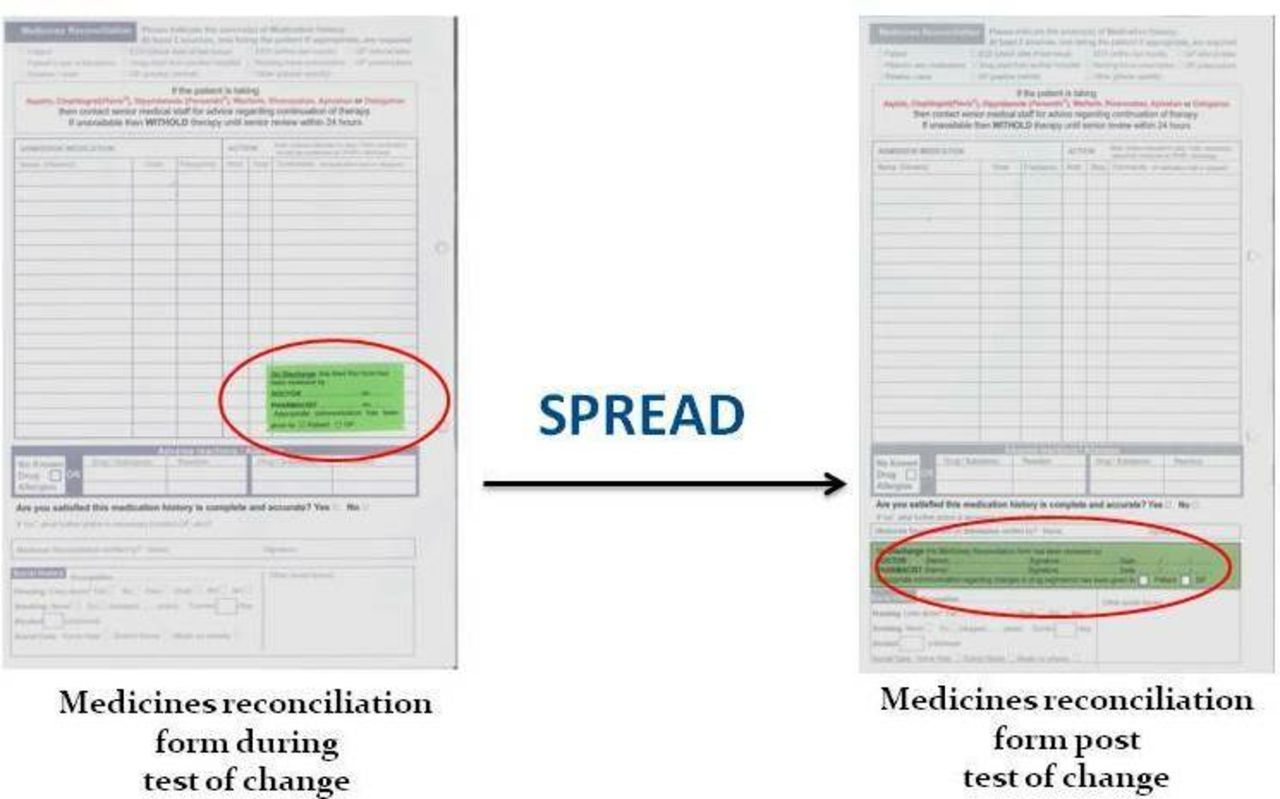
Following the successful implementation and sustainability of the intervention in two separate pilot wards and both independently producing very similar positive outcomes, it was decided to spread the intervention to the remaining eight wards in the surgical department. This involved the redesign of the MR on admission form so that the contents of the green sticker are embedded permanently in the form (figure 7).

A diagrammatic representation showing the changes made to redesign the medicines reconciliation on admission form to permanently accommodate all the new elements of the sticker as part of our sustainability and spread plans.
Data collected across all the 10 wards of the surgical department (figure 8) shows a very similar pattern to that observed in the pilot wards. Only 30% of all the discharge prescriptions clinically reviewed by the pharmacists across the department were accurate and not requiring any amendments before sending to the dispensary for dispensing, with the accuracy steadily and quickly improving to reach a median above 81% following the implementation of the new process. Figure 9 shows that the biggest gap in communication identified during the spread phase was also regarding medicines being intentionally discontinued.

Percentage of discharge prescriptions with accurate drug list and clear communication to the general practitioner regarding any changes in drug history (prior to pharmacist verification). Run chart showing that data collected across all the 10 wards of the surgical department after the spread of the new process displayed a very similar pattern to that observed in the pilot wards, where once the intervention was introduced following the 4-week base-line period, the accuracy of discharge prescriptions steadily and quickly improved from 30.5% to reach a median above 81%. Med Rec, medicines reconciliation.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of discharge prescriptions with gaps in communication regarding changes in drug history (prior to pharmacist verification). Chart showing that similar to the initial surgical pilot ward, the biggest gap in discharge prescription communication during the spread phase was also regarding medicines being intentionally discontinued and the absence of clinical reasoning behind that. This chart also shows how the new process supported the junior doctors increase the percentage of patients with clearly communicated changes regarding their medication history to their general practitioner as part of the discharge document. Med Rec, medicines reconciliation.
A total of 266 discharges were included in the audit over the initial 3-week base-line period of the spread phase averaging 89 discharges per week, while a further 524 discharges were included in the audit over the remaining 6-week period maintaining a similar average of 87 discharges per week.
Discussion
MR addresses the well-documented problem of unintended medication discrepancies introduced across transitions in care.2,6 Improving the transfer of information about medicines across all care settings helps reduce incidents of avoidable harm to patients and improves patient safety.2 The steps of MR at the different stages of transition of care have been long known, well documented and are seemingly straight forward. At discharge, the steps include determining the post-discharge medication regimen, developing discharge instructions for the patient, educating the patient and communicating the information to the primary care team.16 Despite having a local MR policy that clearly described this process, in an effort to standardise practice, there was however very little compliance from our junior doctors. This was reflected in our base line data of less than 50% accuracy in MR on discharge, which is similar to those reported by other studies where more than 70% of discharge prescriptions had at least one unintentional discrepancy.17 A group discussion with the junior doctors to share these findings and explore possible reasons behind it confirmed that despite its wide circulation and availability, there was little awareness and familiarity with the local MR policy and its recommendations especially regarding the need to refer back to the patient’s MR on admission form and using it as a vital source of information alongside the inpatient prescription chart to generate an accurate and safe discharge prescription. This meant there was no standardisation in the process of MR on discharge resulting therefore in tremendous variation in the information gathered, types of sources used and how information is communicated to other providers across the continuum of care. Because the local MR policy has been in place for a number of years and was a permanent agenda item on all junior doctors’ inductions that happened three times a year across the whole organisation, we therefore decided that our improvement intervention cannot simply be additional education or increased awareness. We instead decided to design and test an intervention to support the junior doctors comply with the recommendations of the MR policy by standardising the process of MR on discharge. The intervention aimed to eliminate unwarranted variation in the process of gathering a patient’s medication history, while also ensuring that any changes or amendments made to the medication history since admission are clearly articulated in the discharge communication along with the clinical reasoning behind this.
The newly designed process helped achieve quick and sustainable improvements in the accuracy of MR at discharge exceeding 95% in our pilot wards and 81% across the whole of the surgical department. Our initial findings and results from the pilot wards emphasised the importance of junior doctor familiarity with this new intervention to deliver and sustain the desired improvements. Familiarity comes with time and our inability to sustain data collection across the whole surgical department for more than 6 weeks due to staffing pressures might explain why the improvements during the spread phase did not reach our 90% aim. This could also be as a result of the frequent junior doctor’s rotations and cross cover from other non-surgical wards where this intervention is absent hence magnifying the element of unfamiliarity.
These results provide strong evidence to support the theory on which this quality improvement project was based, proposing that there is a direct link between the use of a patient’s MR on admission record alongside their inpatient prescription chart as sources of information during the MR on discharge process and the accuracy of the discharge prescription produced as a result.
We believe that there are six main factors that have contributed to the success of this project.
First, the intervention was designed, tested and implemented using the basic yet essential principles of the improvement methodologies such as the use of data and patient stories to build will, full staff engagement and empowerment from the very outset in the design and testing phases, using small scale testing and consecutive PDSA cycles, segmentation and sustainability before spread and the ongoing sharing and display of results with all the front line staff and relevant stakeholders. Second, the intervention used was designed to be simple and easy to use so that it can be easily incorporated into the junior doctors’ routine practice and therefore generating very little resistance. Feedback from the junior doctors during the testing and implementation phases confirmed that this new standardised process was easy to follow and did not cause any increase in their workload.
Third, the intervention was mainly designed and implemented as a communication tool to support a team approach to MR on discharge rather than a governance tool to monitor the junior doctor’s performance and compliance with the process. The new process requires both the junior doctors and also the pharmacists to annotate the MR on admission form on review. When the junior doctors annotate the MR on admission form, this provides clear indication to the pharmacist that the form and its contents have been reviewed and used to generate the discharge communication. The pharmacists are also expected to annotate the MR on admission form on review because this indicates to the other members of the multidisciplinary team, such as nurses and other members of the pharmacy team, that they have undertaken the clinical review process and that the patient has been counselled accordingly.
Fourth, our surgical department only embarked on a project to improve the accuracy of MR on discharge after many years invested in improving and sustaining the accuracy of MR on admission which is a vital aspect of this process, because without an accurate MR on admission form there can never be an accurate discharge prescription.
Fifth, a simple redundancy step was designed, agreed and implemented in order to achieve and maintain 100% compliance with the new intervention which in turn helped deliver and sustain very high levels of improvement in the desired outcome. During the 4-week spread phase of the project, 30% of all the discharge prescriptions required the pharmacist to prompt the junior doctors to annotate the MR on admission forms. Although this might be considered a high percentage, it is worth noting that this was 80% during the start of the process and continued to decrease with time. With more time and as the process becomes embedded into the day to day practice, we would expect a further decrease.
Finally, this new intervention has helped introduce a change in the type of communication that dominated the interactions between the junior doctors and the clinical pharmacists regarding discharge planning. One of the junior doctors involved in this project explained during one of the feedback sessions how this new process has completely transformed his working relationship with the clinical pharmacists regarding discharge planning. He explained how the process successfully facilitated a welcome shift from a ‘parent–child’ relationship where the pharmacists are always seeking the junior doctors and pointing out mistakes that need to be amended to a more effective and efficient ‘team work’ approach where junior doctors and clinical pharmacists work together to generate a safe discharge prescription.
Implementing this new intervention and standardising the MR on discharge process has allowed us to successfully reduce variation which in turn helped in reducing both harm and waste. Harm was reduced as a result of improving the accuracy of information about medicines transferred across the care settings and therefore lowering the risk of avoidable harm related to undocumented intentional discrepancies and unintentional discrepancies in a patient medication history. Waste was also reduced because implementing a systemic approach to reconciling medications on discharge was found to decrease pharmacists’ workload by reducing the need to invest additional time to correct mistakes on the discharge prescriptions. Pharmacy time at discharge was significantly decreased by up to 40 min per patient, a finding that was also reported in similar studies implementing a systemic approach to reconciling medications.18 Reducing these unnecessary delays improves the efficiency of the discharge process as a whole and therefore also reduces waste in overall bed capacity and patient flow.
Limitations
We believe that there are two main limitations to our project. First, to ensure 100% compliance with the process measure during that data collection phases of this project, all the discharge prescriptions included for review and analysis where those screened by the clinical pharmacists during their normal working hours; Monday to Friday 08:00–16:00 (figure 3). This meant that there is no data to show how well the process is followed out of hours and during the weekends when there is no pharmacy presence on the wards to undertake the verification step of MR on discharge and prompt the doctors to annotate the MR on admission forms when needed. Second, this project was carried out in the surgical department and it is therefore unclear whether this new intervention would offer the same improvements in a non-surgical environment without further testing.
Conclusion and next steps
As we continue to redesign and improve healthcare services in our quest to improve patient safety, there is an urgent need to re-emphasise the importance that information about medicines is effectively communicated when care is transferred between different teams across the continuum of care. Although this can be challenging, we have shown that it can be done effectively and reliably if this responsibility is equally shared by healthcare professionals from all disciplines while being supported by safe systems that make it easy to do the right thing. The success of this project was largely due to the simplicity of the intervention and its ability to encourage and support standardising the MR on discharge process through a multidisciplinary approach. This new structured approach to MR on discharge, involving different members from the multidisciplinary team and conducted in an environment of shared accountability, helped reduce waste, harm and variation while encouraging a positive shift in the team dynamics between junior doctors and clinical pharmacists.
Guided by our findings, there are a number of steps that we have planned and started to action as part of this ongoing quality improvement journey. Our next steps include collecting data from weekend discharges from the surgical department retrospectively in order to gauge the level of junior doctors’ compliance with this new process in the absence of ward pharmacy support. We have also liaised with colleagues in other non-surgical departments, including oncology and internal medicine, who have agreed to test this new process in their clinical areas to see if it would have the same impact. This would also be part of a wider spread plan across the whole organisation in an effort to further reduce variation in the MR on discharge process when the junior doctors move between different clinical specialities as part of their training programme. We also plan on testing how to formally include the patient and their carers to play a role in the MR on discharge process and possibly annotate the MR forms, alongside the other members of the multidisciplinary team, to confirm their participation and understanding. Engaging the patient is one of the best strategies to prevent reconciliation errors through a patient-centred approach.5
Finally, one of the main concerns commonly raised around MR is its reliance on pharmacists.5 Although involving pharmacists in MR, as most published studies have done, has demonstrated great improvements, pharmacists are in short supply in most hospitals. Continuing to involve pharmacists in MR therefore risks taking them away from other important activities related to pharmaceutical care and patient safety. A previous study tried to address this by offering different levels of MR to patients depending on their needs and had demonstrated significant time savings.19 Perhaps designing and successfully implementing a standardised multidisciplinary MR process that can achieve high sustainable levels of accuracy, as demonstrated in our project, can also help reduce the reliance on pharmacists and help free them up to undertake other clinical roles. The evolving clinical role of pharmacy technicians in the British healthcare system has helped develop models of care where pharmacy technicians now play a vital role in supporting MR on admission.20,21 We therefore plan to explore further the roles that our pharmacy technicians can play in supporting MR on discharge. We believe that there is a unique opportunity to evolve our current MR on discharge model further where certain aspects can be undertaken by pharmacy technicians with continued support of a clinical pharmacist when needed through a referral system. This will help further develop the clinical skills of our pharmacy technicians and strength their role in the MDT while also releasing pharmacists’ capacity to undertake new clinical roles such as prescribing.
Acknowledgments
The authors would like to thank Gillian Allison, Jennifer Bisset and Emma Clark for supporting implementation and data collection. We would also like to thank Dr Owain Prys-Jones for supporting junior doctor engagement.
References
Footnotes
Contributors All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the manuscript. Furthermore, each author certifies that this material or similar material will not be submitted to or published in any other publication before its appearance in the BMJ Open Quality. Authorship contributions: Category 1: Conception and design of study: SB. Acquisition of data: SB, JD. Analysis and/or interpretation of data: SB. Category 2: Drafting the manuscript: SB. Revising the manuscript: SB, JD. Category 3: Approval of the version of the manuscript to be published: SB, JD.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.