Article Text

Abstract
Background Colorectal cancer (CRC) is among the leading cancer diagnoses affecting both men and women worldwide. Prevention and early detection of CRC is possible by increasing access to and utilisation of screening tests. Although CRC screening is highly recommended, screening rates remain suboptimal in the USA, particularly among underserved populations. Our project site, an urban federally qualified health centre, was not meeting the national screening target of 80% of eligible adults.
Objective The aim of this quality improvement project was to increase the number of orders for CRC screening to eligible patients by using unlicensed assistive personnel and automated telephone outreach calls to offer 100 patients CRC screening during an 8-week period.
Methods 40 patients received outreach calls from care coordinators (CC). 40 patients received automated telephone call reminders to call a CC to obtain an order for CRC screening. 20 patients were offered CRC screening by a medical assistant (MA) as part of their scheduled office visits. We used two plan-do-study-act (PDSA) cycles to deliver these three screening interventions.
Results A total of 100 patients received one of the interventions. Ten of those patients received an order for either colonoscopy or faecal immunochemical testing by the conclusion of the second PDSA cycle. The MA-offered screening resulted in the highest percentage of patients accepting CRC screenings and patients preferred this outreach approach compared with CC outreach or automated voice messages. CC outreach yielded a lower rate of accepted screenings. None of the patients who received the automated calls followed up to obtain a screening order.
Conclusion Our project demonstrates that unlicensed assistive personnel have the potential to increase patient access to CRC screening.
- cost-effectiveness
- healthcare quality improvement
- primary care
- quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Of cancers affecting both men and women, colorectal cancer (CRC) is the fourth most commonly diagnosed cancer in the USA.1 CRC is the second leading cause of cancer death in the USA.2 Ninety per cent of those diagnosed with CRC are over the age of 50, but in the USA only 62.9% of this population is receiving CRC testing consistent with current guidelines.3 Although the incidence of CRC has decreased from 2003 to 2012, it remains one of the leading causes of cancer-related deaths across the world accounting for 8.5% of cancer deaths.3 4
Medically underserved populations in the USA include people who face geographic, economic, cultural or linguistic barriers to healthcare.5 Within underserved populations, CRC screening rates are suboptimal which likely contribute to high CRC burden among these populations.6 Low socioeconomic status (SES) is a significant barrier to successfully completing CRC screening.7 In the USA, there is not a system of universal healthcare. So, people of low SES, especially undocumented people, may have no access to screening services such as colonoscopy.
The site for this quality improvement (QI) project was an urban Federally Qualified Health Center (FQHC) in the USA. FQHCs are the safety net health centres that serve patients regardless of ability to pay for care. This FQHC provides comprehensive health services including primary care, nurse midwifery, oral health and behavioural health. Primary care staff within the organisation include family physicians, family nurse practitioners and certified nurse midwives. Unlicensed assistive personnel are predominantly medical assistants (MA), a role requiring a vocational training programme of 6–9 months, and care coordinators (CC), a role requiring on-the-job training to assist patients in completing provider-recommended services. In 2015, the FQHC cared for 30 197 adult patients. Of those patients, 92.4% self-identify as racial or ethnic minorities. 94.6% of the FQHC patients are at or below 200% of the federal poverty level. The FQHC’s CRC screening rate among eligible patients is 39.7%. This compares to a US average screening rate of 62.9%.8
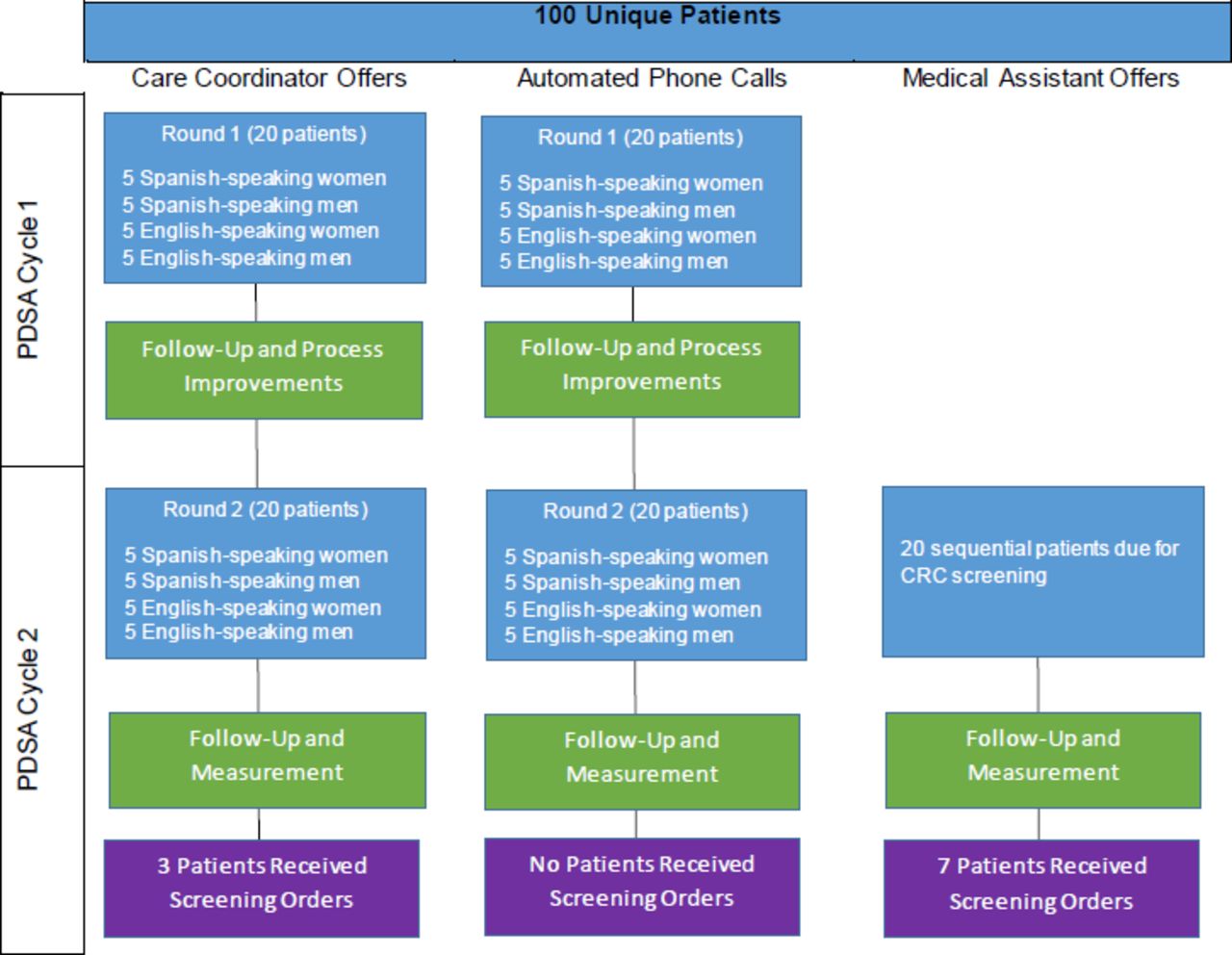
The aim of this QI project was to increase the number of orders for CRC screening to eligible patients by using unlicensed assistive personnel and automated telephone outreach calls to offer 100 patients CRC screening during an 8-week period. Forty patients would receive outreach calls from CCs. Forty patients would receive automated telephone call reminders to call a CC to obtain an order for CRC screening. Twenty patients would be offered CRC screening by an MA as part of their scheduled office visits (figure 1).

Colorectal cancer screening project design and outcomes. CRC, colorectal cancer; PDSA, plan-do-study-act.
Background
Prevention and early detection of CRC is possible by increasing access to and utilisation of screening tests.9 Screening tests for CRC can identify abnormal growths before becoming cancerous, or detect CRC at an early stage prompting further intervention. With successful early detection, the initiation of appropriate interventions and treatments often leads to a cure. Increased use of colonoscopy has led to a large decrease in CRC incidence and its death rate in the past decade.9
While colonoscopy is considered the ‘gold standard’ for CRC screening,9 other screening methodologies are available. The US Preventive Services Task Force provides equal recommendations for faecal immunochemical testing, sigmoidoscopy and colonoscopy.9 So screening test selection should be guided based on patient preference and resources. ‘The best test is the one that gets done,’ embraces the view that screening patients for CRC, regardless of test methodology, is the best strategy for preventing CRC among underserved populations.6
At our agency, current practice for ordering CRC screening is for providers to order testing, typically colonoscopy, at the point of care when an eligible patient is identified in the office. This is an example of opportunistic screening. This approach limits screening only to those who attend healthcare encounters and relies on provider workflow to assure screening is offered. Organised screening, a population health intervention, versus opportunistic screening is more successful at identifying all members of a population who are eligible for screening.10 Effective population health interventions include automated phone calls to recommend screening11 and CC-offered screening.12 When opportunistic screening is used, an effective strategy to increase the impact of this approach is to authorise MAs to order screenings based on a standing order set.13
Measurement
The focus of this project was to improve the process for ordering CRC screening, and we did not address completion rates. We tracked two process measures: number of patients for whom screening was ordered and patient intention to act on the screening order. Our outcome measure of interest was cost to deliver the intervention. Our balancing measures included: intervention acceptability to patients and intervention acceptability to staff.
Design
The FQHC was not meeting CRC screening goals for its patients and the system for offering CRC screening relied entirely on patient attendance and provider workflow. Through this project, the QI team sought to improve the process for ordering CRC screening. The team consisted of clinical providers (nurse practitioner and physician), administrators, Doctor of Nursing Practice (DNP) students and DNP faculty from an academic partner. This project implemented evidence-based interventions through a series of small tests of change, including: (1) CC phone call outreach in both English and Spanish; (2) automated CRC screening reminder phone call outreach in both English and Spanish; and (3) MAs offering CRC screening during scheduled visits to eligible patients.
The QI team led an education session for the CCs covering CRC, screening methodologies and screening guidelines. The team then generated a report from the clinic’s electronic health record of patients due for CRC screening. Using a structured phone call script, CCs phoned patients and offered CRC screening, entering orders as appropriate using a standing order set. Concurrent to the CC outreach calls, a separate group of patients received automated phone calls reminding them that they are due for screening and requesting the patient to call a CC to arrange a CRC screening order. The MA-offered intervention made CRC screening orders a part of intake into the exam room. While preparing patients for providers, MAs would review patients’ charts to determine if they were due for CRC screening and enter this order prior to the provider seeing the patient.
Strategy
QI project aims should be specific, measurable, achievable, realistic and timely (SMART).14 Our SMART aim was to increase by 5 the number of orders for CRC screening in a population of approximately 100 eligible, unscreened patients over an 8-week period. We used a rapid-cycle quality improvement approach that included two plan-do-study-act (PDSA) cycles over 8 weeks.15 This project was reviewed by our institution’s Office for the Protection of Research Subjects and was determined to be a QI activity, therefore not subject to Institutional Review Board oversight.
PDSA Cycle 1
In cycle 1, we began by developing a standing order that authorised MAs and CCs to order CRC screening based on specific patient criteria. This order was signed by the FQHC’s chief medical officer and made a part of the organisation’s policies and procedures. We then developed an educational session to train the CCs on CRC screening (CRC background, screening methodology, screening guidelines). Concurrently, we developed a script in both English and Spanish for an automated outbound call to remind patients they are due for CRC screening. We then trained the CCs to make outgoing calls and receive response calls from patients who received the automated phone call. Using the electronic health record’s reporting features, we generated two lists of 20 patients: one group received CC outreach calls and the other received automated calls. Each list of 20 patients contained five each of English-speaking men, English-speaking women, Spanish-speaking men and Spanish-speaking women. During a 1-week period, the CCs called the patients and the electronic health record system sent the outbound phone calls. Three attempts were made per patient.
One week after a patient’s last outreach call was made, the QI team phoned the patient to administer a questionnaire regarding their experience with the intervention. We also interviewed CCs to solicit their feedback on how to improve this process. We used this feedback to revise the process prior to implementing PDSA cycle 2.
PDSA Cycle 2
With feedback from patients who received calls in PDSA cycle 1, we revised the script used for the automated phone message to enhance clarity. We also changed the day and time of the CC and automated phone calls to increase the likelihood that the patient would be available. CC feedback on cycle 1 revealed a need to change permission settings in the electronic health record to enable delegation of order entry for the CCs. We then generated two new lists of 20 patients each using the same demographics. The CCs made outreach calls to 20 of these patients and the other 20 patients received the revised automated phone call. After 1 week, we phoned each patient to again inquire about their experience with the process. The QI team also interviewed CCs to obtain their feedback about the process.
Also within PDSA cycle 2, we implemented MA-offered opportunistic CRC screening. The QI team conducted a brief training with the MAs, modelled on the CC training. On select clinic days, QI team members shadowed MAs and assisted them in identifying scheduled patients who were due for CRC screening. MAs then offered the screening to these patients during their scheduled intake. After the MA completed their intake process, a QI team member interviewed the patient to evaluate their experience with the process. We continued this intervention until we reached 20 patients who received MA offers for CRC screening. Once this number was reached, we interviewed the MAs to elicit their feedback and critique of this strategy.
Results
None of the patients (n=40) who received automated phone calls returned the call to accept a CRC screening order. Of the patients who received outreach calls from CCs (n=40), the CCs were unable to reach 23 patients. These patients either did not answer after three calls or did not return a call within 1 week of the CC leaving a message. Of the patients the CCs were able to contact (n=17), three accepted the CC offer to enter orders for screening (figure 2). Eight patients declined the CC offer to provide the screening order and instead scheduled appointments with their provider to discuss the screening recommendation. Three reported that they had already had a colonoscopy elsewhere and provided these records to the CC. Two patients declined screening entirely. One patient reported they were already scheduled for a colonoscopy in the coming month. Of the patients who received MA offers for CRC screening (n=20), seven accepted an MA-entered order for CRC screening (figure 3). Three declined the MA offer but accepted the same offer from their provider at the visit. Nine patients declined the CRC screening. One patient was found to have been previously tested elsewhere and provided records of the screening test. In total, 10 of the 100 patients in the QI project accepted a CRC screening order from unlicensed assistive personnel.
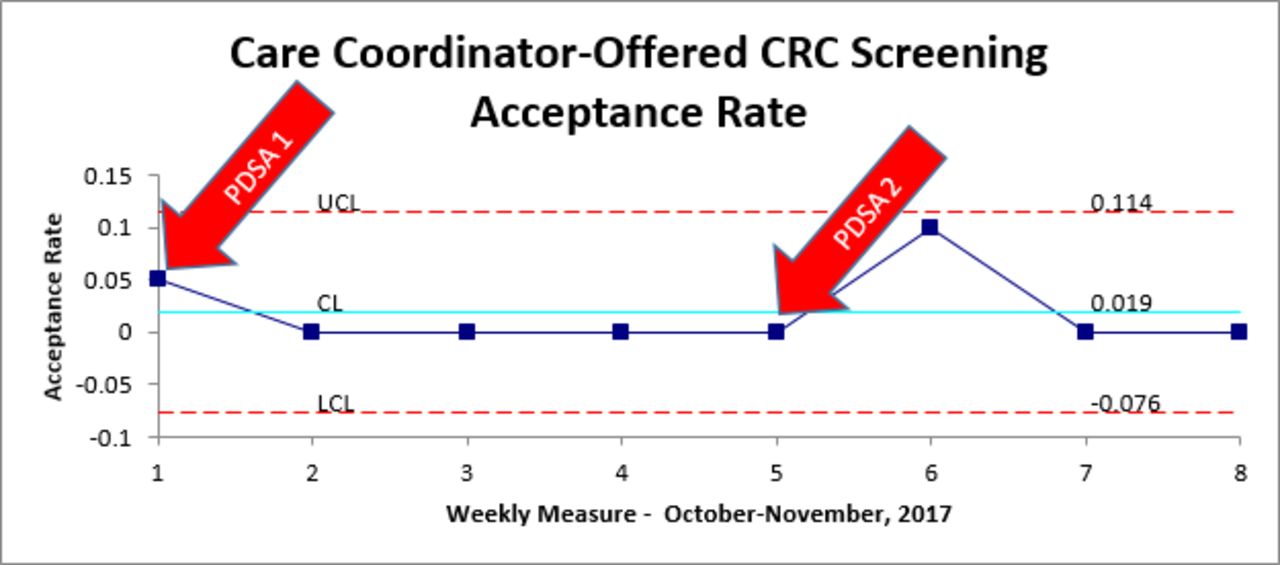
X-chart illustrating rate of patient acceptance of care coordinator-offered CRC screening. CL, control limit; CRC, colorectal cancer; LCL, lower control limit; PDSA, plan-do-study-act; UCL, upper control limit.

{kind=link}
{kind=link}
{kind=link}
X-chart illustrating rate of patient acceptance of medical assistant-offered CRC screening. CL, control limit; CRC, colorectal cancer; LCL, lower control limit; PDSA, plan-do-study-act; UCL, upper control limit.
The QI team phoned each patient who received automated phone calls 1 week after the last call attempt in order to evaluate intervention acceptability. Most patients (n=24, 60%) did not respond to these outreach calls. Of those who did respond to the follow-up calls (n=16, 40%), none reported any intention to act on the automated call. The primary feedback was that the patients did not understand the intent of the automated message. Two patients indicated they understood the message but chose not to act on it due to lack of health insurance. One patient, when explained the reason for the original call, asked the QI team member to please provide them with a colonoscopy order.
The QI team phoned each patient who received CC calls to evaluate intervention acceptability. The team only was able to reach 5 of the 40 patients who received CC calls. These five patients were all individuals who had requested an appointment with a provider to discuss screening. In the conversation with the QI team members, who were registered nurses (RN) and disclosed this on the call, all five patients requested the RN team member to enter an order for CRC screening rather than wait for an appointment with their providers. All patients stated an intent to act on the order.
The QI team interviewed each of the 20 patients who received MA offers for screening at the conclusion of their visits with their providers. Of the seven patients who received an MA-entered order, all expressed an intent to act on the order. Of the 12 patients who declined the MA offer for screening, three subsequently accepted a screening order from their provider. All patients expressed trust in the MAs’ ability to explain CRC screening and enter appropriate orders.
Of the staff members involved in this QI project, the CCs were most receptive to the practice change. The CCs reported that they viewed this activity as part of their work and their role. That did not perceive a burden to carrying out this new work. The primary concern of the CCs was that they did not feel qualified to address any questions that deviated from the screening decision tree we created. They preferred to defer any clinical questions about CRC screening to a licensed provider. CCs reported that 5 minutes of time on the phone was sufficient to explain the need for screening and enter the order. However, some patients viewed the CC call as an opportunity to address other concerns and CCs expressed concern this could impair their ability to complete their other work.
MAs were less receptive to the practice change of this QI project. MAs in the agency are evaluated on a number of metrics including time spent placing patients in exam rooms. MAs were concerned adding the work of offering screenings would adversely affect their performance evaluation. Additionally, the MAs expressed that this additional work would add to the number of other responsibilities they have in their roles. Overall, the MAs reported a high level of dissatisfaction with this practice change.
The automated calling system generated no new costs but also did not generate any accepted offers for screening. The CCs’ outreach to 40 patients yielded three accepted offers for screening which, based on our salary structure, yields a labour cost of $9.22 per accepted screening. The MAs’ offers of screening to 20 patients yielded seven accepted offers at a labour cost of $3.95 per screening.
Lessons and Limitations
We sought to improve the CRC screening ordering process to assure that more patients who are eligible for screening receive orders. Our approach blended both population health strategies with opportunistic screening strategies. It is clear from our QI project that some patients are responsive to screening offers from unlicensed assistive personnel. However, the costs to get screening orders to the people who need them may be prohibitive. The population health strategy that potentially had the lowest cost (automated phone calls) was the least acceptable to patients and generated no responses. The population health approach that was most acceptable to patients (CC outreach calls) was relatively costly. Potentially, if the CCs became more confident in their knowledge and ability to provide this service, more patients would accept the offer as opposed to seeking a provider visit to discuss screening. This would make the cost per accepted offer lower. That QI team members (RNs who were DNP students) who made follow-up calls to patients in the CC group were able to conclude the call having provided the patient with a screening referral suggests the possibility that patients may prefer to receive screening recommendations from licensed providers. Alternatively, this may simply be that the QI team had sufficient content knowledge to address patient questions more effectively.
While the MA-offered screenings generated the highest number of accepted screenings at the lowest cost per screening, this approach is limited in two significant ways. This approach only reaches patients who are engaged enough in care to attend office visits and it comes at the expense of creating job dissatisfaction for the MA team members. The approach is helpful in that it enables the care team to share the responsibility of assuring that patients receive appropriate screenings.
A key lesson learnt in the MA implementation was that the MAs did not feel a part of the planning process for this QI project. If this approach is used elsewhere, it would be essential to include MA staff members in the original project design. Additionally, the QI team made a false assumption that MAs had knowledge about CRC and screening approaches so did not provide sufficient training prior to implementation.
Several limitations may be considered when interpreting our outcomes. An important limitation of this QI project is that we did not track completed screenings. Patients who accepted screening offers universally communicated an intent to act on the screening. But, the project was not designed to track completion. Another limitation of this study was the small sample size, which affects its generalisability. Lastly, our project was limited to two PDSA cycles. Further cycles would help to refine and improve intervention effectiveness and efficiency over time.
There were two unforeseen challenges in this project. Though authorised to order screenings by a standing order, the CCs did not have permissions configured to enter these orders in the electronic health record at the start of the project. We addressed this and enabled this functionality in the second PDSA cycle. A second challenge had to do with the processing of faecal immunochemical tests. Though the laboratory vendor permitted patients to mail in these testing cards, staff in the clinic instructed patients to return the cards to the clinic in person. This was based on staff members’ experiences with cards being lost in the mail as well specimens rejected by the lab due to incomplete paperwork submitted. This may have been a barrier to patients accepting testing offers when they learnt that they would need to return to the clinic to drop off the specimen.
Our reports of patients who were not current on screening inadvertently included patients who had been screened elsewhere. Reaching out to these patients used resources (CC and MA time). However, an unforeseen benefit is by contacting these patients, we were able to add these results to the patients’ health records.
Conclusions
In this project, we met our aim of increasing by 5 the number of orders for CRC screening in a population of approximately 100 eligible, unscreened patients. We believe that, with refinement, the processes we implemented in this project have the potential to be quite useful in increasing the number of patients who receive orders for CRC screening. The measures we used to evaluate this process (cost to deliver intervention, number of patients for whom screening was ordered, patient intention to act, intervention acceptability to patients, intervention acceptability to staff) were appropriate to the project. While our balancing measures did not include the impact of the intervention on CC/MA job satisfaction, we recommend others attempt to track this should the intervention be reproduced. We hypothesise that this intervention potentially improved CC job satisfaction as they felt more empowered in their roles. However, the intervention likely had a negative impact on MA job satisfaction who felt overwhelmed by adding additional work.
A key observation we made in carrying out this project was the conflict between evidence and our experience. Previous work has demonstrated that automated phone calls increase the likelihood that patients will act on preventive health instructions.11 But, given the rapid rate of change in the telecommunication technology, we question if this remains true today. Our conclusion from this small project is that the era in which people listen to automated phone calls, including those from their healthcare provider, may have passed.
From a purely financial perspective, this project as implemented is not financially sustainable. If scaled up without modification, the labour costs associated with screening are unlikely to be recouped by the FQHC. However, there are substantial systemic savings that could be appreciated by expanding the role of unlicensed assistive personnel to include ordering cancer screenings. Unlicensed assistive personnel could significantly improve the reach of population health initiatives in a cost-effective fashion.
Our project demonstrated that unlicensed assistive personnel have the potential to play an important role in expanding access to CRC screening. We feel that additional refinements to this approach may help healthcare systems to fully realise the value of unlicensed assistive personnel. CRC screening has long been exclusively the purview of individual providers. By expanding unlicensed assistive personnel participation in CRC screening campaigns, we may be able to make a significant impact on the health of our communities.
Acknowledgments
The authors thank Ellen Barton, APRN, and Paul Luning, MD, for their support in executing this quality improvement project and Marianne Durham, DNP, for her assistance in data visualisation.
Footnotes
Contributors KI, SAK, EW and CTY designed, implemented and evaluated the QI programme presented in this manuscript. KI and CTY prepared the manuscript for publication with input from EW and SAK. All authors reviewed and approved the final manuscript submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.