Article Text

Abstract
Traditionally regarded as good practice, continuous infusions of sedation and analgesic medications are used to reduce anxiety and distress and facilitate care of mechanically ventilated patients in the intensive care unit (ICU). Growing evidence has demonstrated that use of such infusions prolongs days spent invasively ventilated, increases the incidence of ICU acquired weakness and delirium and subsequently increasing the duration of their ICU and hospital stay. Several critical care guidelines recommend titrating to light sedation ±a daily sedation hold or spontaneous awakening trial (SAT). Given the known beneficial effects of sedation holds, we aimed to increase their use within our ICU, a 10-bedded unit with mixed ICU and high-ependency unit facilities in National Health Service Scotland. A retrospective case note review was performed to obtain baseline data of SAT eligible patients who received a sedation hold. The model for improvement 1 was used to implement an ICU protocol based on the ‘Wake up and breath’ guidelines 2 and measure the improvements made. The median percentage of SAT eligible patients that received a sedation hold increased from 47% to 96% during the project period. No significant adverse events were reported during this period and a reduction in ventilation and unit stay was observed. Quality improvement methods have facilitated successful and safe integration of a daily sedation hold protocol in our ICU.
- critical care
- pdsa
- quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Traditionally regarded as good practice, continuous infusions of sedating and analgesic medications are used to reduce anxiety and distress and facilitate care of mechanically ventilated patients in the intensive care unit (ICU). Growing evidence has demonstrated that use of such infusions prolongs days spent invasively ventilated, increases the incidence of ICU acquired weakness and delirium, subsequently increasing the duration of their ICU and hospital stay.3–7 Several critical care guidelines recommend titrating to light sedation ±a daily sedation hold or spontaneous awakening trial (SAT).8–11 Given the known beneficial effects of sedation breaks, we undertook a retrospective case note review to establish our current compliance with these guidelines. This review identified that 47% of SAT eligible patients within our combined ICU/high-dependency unit (HDU) (consisting of a mix of both surgical and medical patients) were receiving a sedation hold, highlighting an opportunity for improvement.
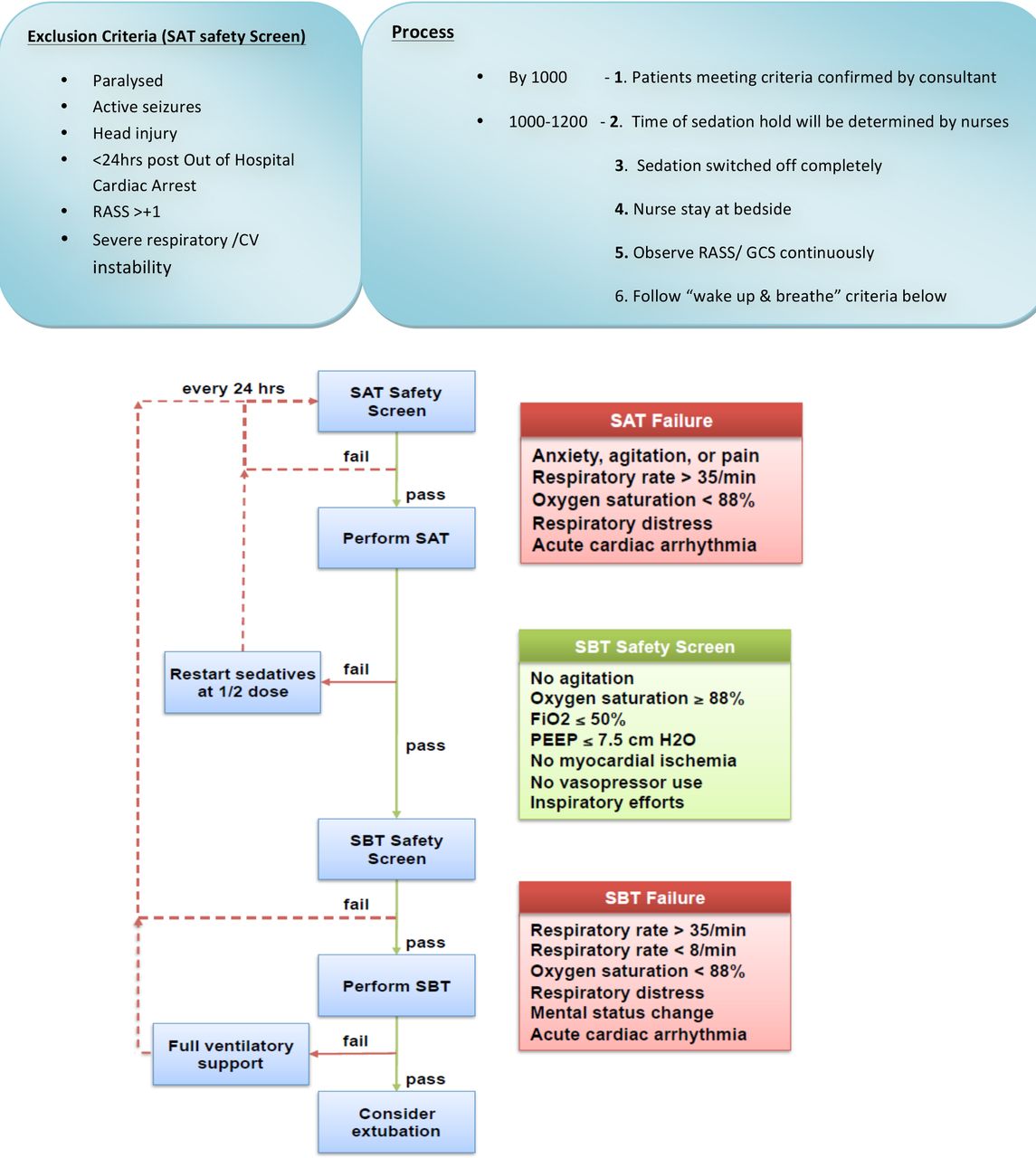
In order to improve practice, a multidisciplinary protocol was designed and implemented based on the ‘Wake up and breath’ guidelines2 with the overall aim to increase the compliance of SATs in eligible patients to 80% over the 6-month intervention period (figure 1).

Daily sedation break/SAT protocol. RASS, Richmond Agitation Sedation Scale; SAT, spontaneous awakening trial; SBT, spontaneous breathing trial; CV, cardiovascular; GCS, glasgow coma scale.
Background
Emerging evidence suggests that the deep sedation of ICU patients has significant adverse effects with guidelines advising that unless absolutely necessary it should be avoided. In the late 1990s, it became apparent that continuous sedative infusions were an independent predictor of longer ventilator time and both ICU and hospital stay. A prospective observational study of 242 medical ICU patients demonstrated a statistically significant reduction in ventilator, ICU and hospitalisation days when using bolus or no sedation versus continuous sedation.3 Furthermore a randomised control trial (RCT) found that daily interruptions of continuously infused sedation reduced ventilator time by more than 2 days and ICU stay by 3.5 days compared with usual care.4 These seminal pieces of work led to further research and a general movement away from the deep sedation of ICU patient.12–15
Further research studies have addressed the relationship between deep sedation and delirium in ICU patients (as assessed by the CAM (Confusion Assessment Method)-ICU tool).16 A large RCT demonstrated a significant increase in the incidence of delirium as the level of sedation deepened.7 These results have been supported by a prospective longitudinal cohort study17 which found delirium to be significantly less in lightly versus deeply sedated ICU patients.
In addition to the impact on delirium, ventilation, ICU and hospital days, sedation has been shown to impair mobilisation of patients in ICU, in turn, leading to neuromuscular or ‘ICU acquired weakness’. This condition has also been shown to prolong ventilation days, ICU and hospital stay and increase delirium rates.5 6
In response to the evidence, several critical care guidelines now recommend titrating to light sedation +/-±a daily sedation hold.8–11 Taking cognisance of our baseline data, the compelling evidence gathered from the literature and the best available practice guidelines; a requirement for improvement was realised by our small multidisciplinary team (MDT).
Measurement
Retrospective case note review was used to collect baseline data to determine current practice over a 6-month period from August 2016 to January 2017. The inclusion criterion was patients ventilated for more than 2 days, of these 31 patients were selected at random. Data collected included eligibility for a sedation hold, if one was completed, average Richmond Agitation Sedation Scale (RASS)18 score for stay and number of ventilated/unit days.
The results of this primary audit revealed patients who were SAT eligible received a sedation hold a median of 47% of the time. The RASS score on average for all patients over the duration of their stay was −2.3 demonstrating light to moderate sedation levels. On average, patients during this period spent 7 days mechanically ventilated and 10 days within the ICU/HDU.
Design
There were two key areas identified for improvement one, ensuring more patients routinely received a sedation hold and two, reducing the average sedation levels of patients as assessed by RASS.
The first step in this process was engaging key stakeholders, namely the ICU consultants, nurses and trainee doctors. Results of the primary audit were presented to groups of staff in order to highlight the issue of over sedation and present an opportunity for improvement.
The next step was to design a new evidence-based sedation protocol using evidence gathered from the literature review and best practice. All mechanically ventilated patients were considered and exclusion criteria was used to identify patients eligible for a SAT/spontaneous breathing trial and a six-stage approach was adopted (figure 1). Following design, this protocol was disseminated to the ICU consultants and charge nurses for review. After minor modifications it was tested on an individual nurse/ patient basis on a maximum of two patients per day. The protocol was then subjected to rigorous testing via rapid PDSA (Plan, Do, Study, Act) cycles. On completion of testing the protocol was ready for the implementation phase.
The team met frequently during the PDSA cycles to monitor the implementation and take on board any learning opportunities identified.
A short questionnaire was designed for both nursing and medical staff to complete following implementation of the protocol to establish if they felt they had an adequate understanding of the sedation hold protocol, its ease of use and if any issues had been encountered. Medical staffs were also asked if they would now be willing for nursing staff to instigate a sedation hold on patients that met SAT criteria following protocol implementation.
Strategy
The model for improvement1 was used with PDSA cycles to develop, test and implement the new sedation protocol. A simple audit tool was used.
Online supplementary PDSA cycle 1. (March 2017): Aimed to raise awareness of SAT criteria and provide confidence in performing a sedation hold.
Supplemental material
Online supplementary PDSA cycle 2 (June 2017): Aimed to enhance confidence and use of SAT criteria and introduce new time frames for performing the sedation hold.
Supplemental material
The first PDSA cycle tested a seven-stage process outlining the steps to be undertaken when considering and performing a sedation hold. Balancing measures were noted in the form of adverse events which occurred during a sedation hold. It quickly became apparent that the time scale for deciding which patients got a sedation hold was problematic, with only 14% of patients being identified and confirmed as candidates by the stated time. The quality improvement group concluded that the process could be simplified into six stages and the time scale for identifying eligible patients relaxed. The protocol was redesigned and online supplementary PDSA cycle 2 commenced.
Online supplementary PDSA cycle 2 tested the new six-stage process and provided continued education and support to nurses undertaking the sedation hold. In this cycle, all patients had a timely sedation hold and the feedback from the nursing staff on the protocols’ usability was positive.
The protocol was then fully implemented and data collection commenced. The following month (July 2017) was spent prompting consultants to make timely decisions and supporting and educating trainee doctors and nurses on the SAT criteria and sedation hold process. This helped to ensure the protocol was embedded prior to measuring the reliably which took place prospectively on a rolling basis over the subsequent 6-month period.
Data on sedation holds were collected prospectively using a simple paper audit form with six tick yes or no questions, each of which corresponded to a stage in the sedation hold process. Nurses completed these audit forms daily for all ventilated patients and noted any adverse events. Data on average RASS, length of ICU stay and ventilator days was collected retrospectively at the end of each month.
Results
During the testing period for online supplementary PDSA cycle 1, a median of 65% of SAT eligible patients received a sedation hold. This was further improved during PDSA cycle 2, to 79% of SAT eligible patients receiving a sedation hold. Following protocol implementation, 96% of SAT eligible patients received a sedation break, over a 100% improvement from the baseline of 47% (figure 2).
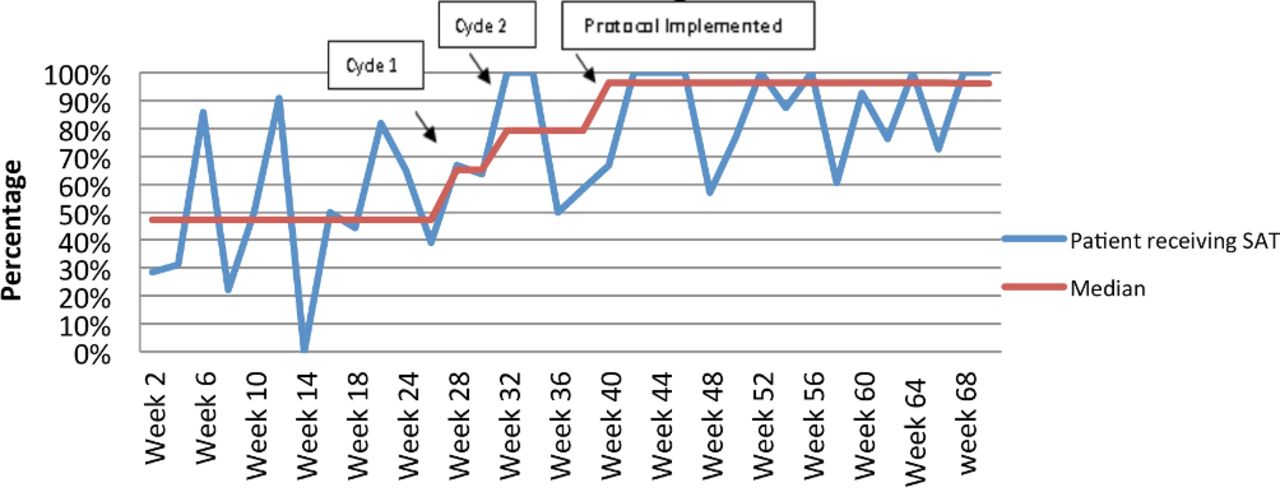
Patientsreceiving an SAT in ICU. ICU, intensive care unit; SAT, spontaneous awakening trial.
Weeks that there were no ventilated patients were excluded prior to data analysis.
RASS scores during the testing period showed no improvement with an average RASS of −2.4, therefore, the decision was made to stop collecting it at this stage.
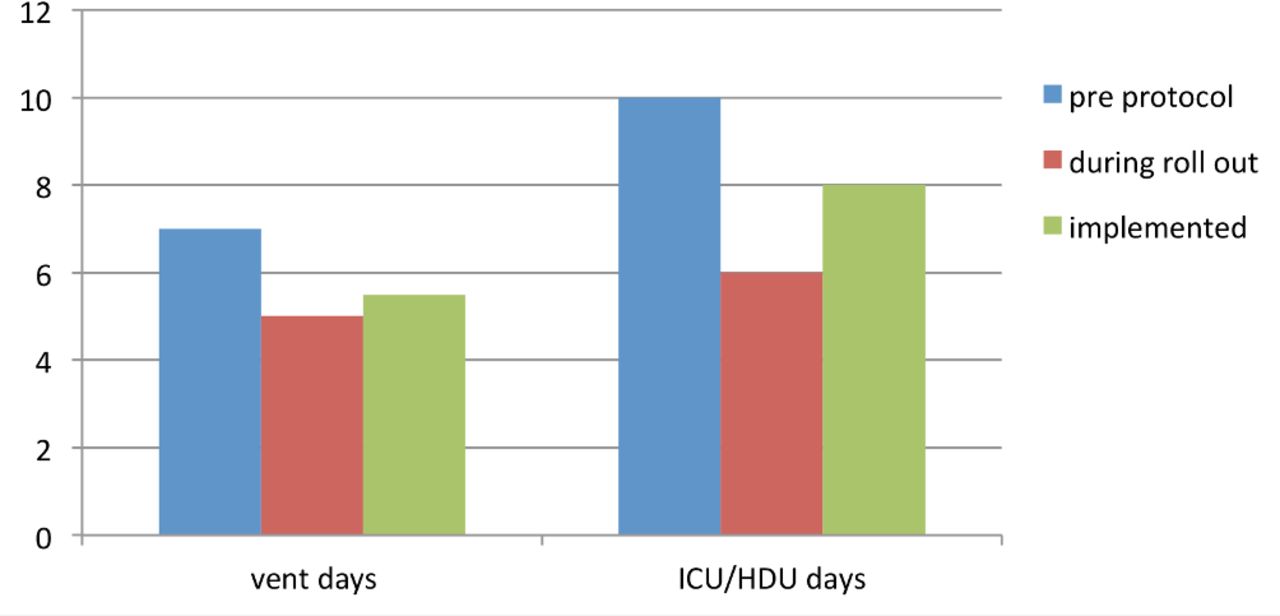
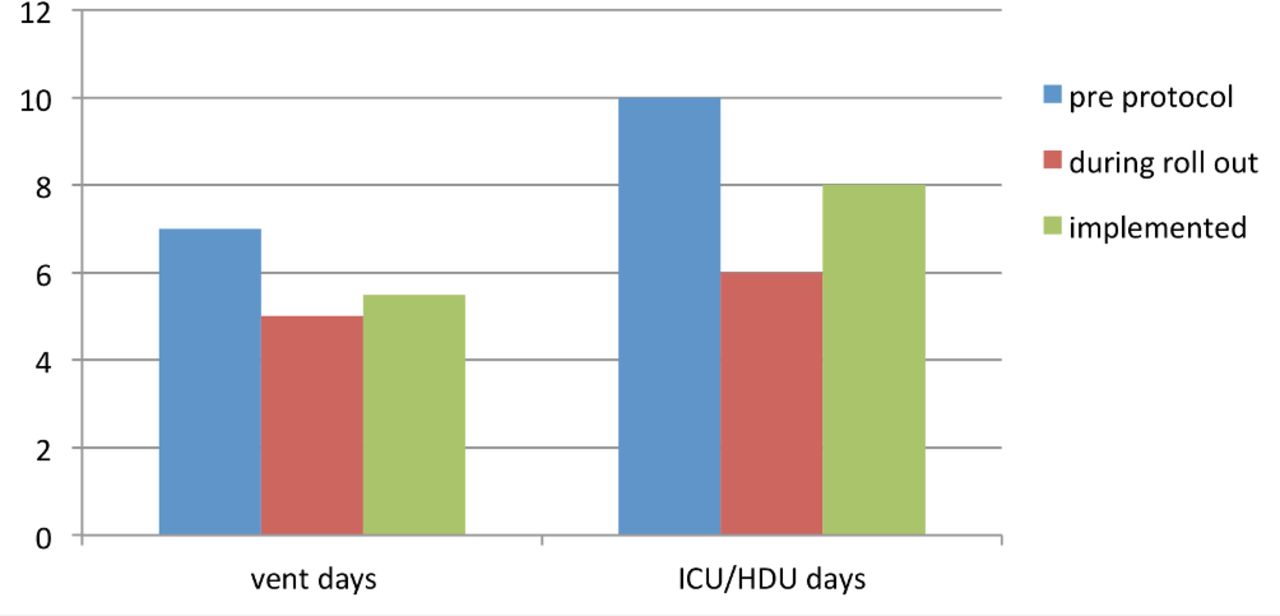
The number of ICU ventilation days reduced from 7 days preproject to 5 days during testing period. This, however, increased to 5.5 days following protocol implementation (figure 3).
{kind=link}
{kind=link}
{kind=link}
Days spent on mechanical ventilation and within ICU/HDU. HDU, high-dependency unit; ICU, intensive care unit.
Length of stay within our combined ICU/HDU also improved from 10 days pre project to 6 days during testing period. An increase was again found post implementation to 8 days (figure 3).
No adverse events such as endotracheal tube dislodgement or invasive line dislodgement were reported during the project period.
Limitations
This improvement project aimed to increase the reliability of SATs in eligible patients to 80% over the 6-month intervention period. The key focus was to implement a sustainable MDT-based solution rather than a short-term intervention. A protocol was designed and adapted during the project using PDSA cycles which helped to ensure the successful implementation of the final protocol.
Limitations include the following: a small population of 112 patients in total were selected during this project; therefore, this limits the generalisability of our results. Additionally, our length of stay data may not be directly comparable to other units due to our composite HDU and ICU. Ventilation and length of stay improved most during the testing phase, conducted over the summer months where traditionally occupancy falls within ICU. Comparison can, however, be made pre and post implementation as the same winter months were used each year for data collection.
We plan to randomly sample patients to reassess process reliability following completion of this project. Continued education and support for staff is a key priority for the team.
This is evident from the result of questionnaires carried out postintervention that highlighted medical staff were less aware of the protocol than nursing staff. Possible reasons for this include medical staff rotating or only covering out of hours. Additionally, all medical staff that replied stated they would be willing for nursing staff to instigate a sedation hold if SAT criteria had been met.
Conclusion
As previous research has shown, sedation holds reduce length of stay and length of ventilator days. While taking into account its limitations and small sample size, it appears to have a similar effect within this project, although we cannot conclude this without reservation. When directly comparing corresponding months (pre and post intervention), days spent mechanically ventilated reduced from 7 to 5 and days spent within our combined unit reduced from 10 to 8, suggesting that the introduction of this protocol has had a positive effect on these results (figure 3).
It would appear that despite equal promotion of this project to all stakeholders, nurses remained much more aware of the protocol, therefore, nurse-led sedation holds may be more appropriate.
It was noted, however, that despite more patients receiving sedation holds, this did not result in improvement in patients’ average RASS scores. As the RCT comparing protocolised sedation management versus protocolised sedation with daily sedation interruption revealed that sedation holds were associated with higher mean daily doses of midazolam and fentanyl and more daily boluses of benzodiazepines and opiates,15 this would suggest that light targeted sedation may be more beneficial. This is an area in which we hope to concentrate future work.
Overall sedation holds have been found to be achievable and safe to carry out.
Acknowledgments
Nursing and medical staff Hairmyres ICU. Data Support Scott Purdie NHS Lanarkshire.
References
Footnotes
Contributors DF planned the study. All authors designed the model and the computational framework. DF and LF carried out the implementation, data collection and data analysis and interpretation. DF wrote the manuscript with input from all authors. Critical revision of the article was carried out by MC. Final approval of the version to be published was agreed by all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.