Article Text

Abstract
Discomfort in the hospitalised patient continues to be one of the healthcare system’s greatest challenges to positive patient outcomes. The patients’ ability to focus on healing is impaired by discomforts such as pain, nausea and anxiety. Alternative, non-pharmacological therapies have shown to be effective in reducing discomfort and managing pain, complementing analgesic agents and optimising pain therapy modalities. This multi-cycle project is aimed to assess the effect of alternative therapies on inpatient, progressive care patients who reported discomfort or little to no relief in discomfort from prescribed analgesics and adjuvant agents. In the first Plan Do Study Act (PDSA) cycle, patients who reported discomfort were offered aromatherapy or visual relaxation DVDs. In the second PDSA cycle, patients were offered a comfort menu that consisted of multiple alternative interventions such as aromatherapy, ice or heat and ambulation. During each cycle, participants completed a survey measuring comfort levels before and after patient-selected alternative intervention(s) were administered. In the first PDSA cycle, 88% of patients reported an increase in comfort level after the intervention, and 97% reported an interest in using alternative therapy again. In the second PDSA cycle, 47% reported increased comfort, and 89% indicated a willingness to try alternative therapies again for improvement of comfort level. Overall, the quality improvement project increased the level of comfort reported by hospitalised patients, creating a gateway to comfort with less emphasis on prescribed analgesic medications.
- PDSA
- quality improvement
- nurses
- pain
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Many times, the causes of discomfort for hospitalised patients are complex, and effective ways to reduce pain, anxiety, stress and nausea without the sole use of pharmacological interventions are needed. Although the use of non-pharmacological methods to maximise pain relief has been demonstrated, these methods have not been offered routinely as a first-line intervention.1–4 The purpose of this study is to implement a process that supports the utilisation of alternative methods such as aromatherapy, visual relaxation DVDs and the application of ice or heat to decrease the causes of patient discomfort while simultaneously addressing the standards of care for their medical diagnosis.
This quality improvement project was performed at the University of Kansas Health System, a regional academic medical centre providing a full range of inpatient services in the greater Kansas City area. The project was conducted on a 22-bed medical telemetry unit that primarily cares for internal medicine patients with infection, gastrointestinal, hepatobiliary and cardiac disorders. To understand how well patients’ reports of pain were addressed before the initiation of the quality improvement project, team members examined patient ratings of pain intensity, using the Numeric Pain Rating Scale (NPRS).5 6 The NPRS is an 11-point scale, from 0 to 10, indicating no pain to the most intense pain imaginable. Many patients reported experiencing little to no change in pain intensity after pain medication was administered. In response, the team explored alternative interventions that could better aid in pain management and sought effective comfort therapies to reduce distressful symptoms such as nausea and anxiety.
Background
During the 1990s, pain was accepted as a ‘fifth vital sign’ that highlighted the need for improved pain management and supported the notion that pain was undertreated.7–9 During that period, a push to enact policies to control and manage patients’ pain levels was initiated on a national level. Organisations such as the Veteran’s Health Association and the Joint Commission quickly accepted the policy standards for the management of pain and introduced a national strategy to improve pain treatment.10 Prescriptions for pain medication by healthcare providers increased substantially. Inadvertently, providers began prescribing analgesic medications that have addictive properties to patients who complained of pain, which many believe has led to the overtreatment and overuse of opioids.2 According to the Centers for Disease Control and Prevention, approximately 115 Americans die every day from an opioid overdose,11 and prescription opioids have been confirmed to be a large contributor to the opioid epidemic.12 13
In response to public outcry of opioid-related deaths, hospitals have implemented action alerts and educational sessions to reduce the number of opioid prescriptions while managing patients’ chronic discomfort.14 15 However, the inpatient setting continues to have patients who suffer from acute and chronic pain, stress, anxiety, nausea and other discomforting symptoms. Managing these symptoms, while reducing the risk for future potential addictions, has become a priority for healthcare providers. Alternative therapies to relieve pain and enhance comfort such as aromatherapy, visual relaxation DVDs and ice or heat have the capacity to provide a way for discomfort to be addressed in a safe manner.16–18 Aromatherapy has proven to decrease stress, depression and anxiety.19 Further, findings reported in a systematic review support the use of music as an adjuvant approach to pain control in adult hospitalised patients.20 Moreover, using non-pharmacological interventions to address comfort without the adverse effects associated with opioid use can improve patient safety and satisfaction with their perception of comfort and pain relief.
Measurement
Before an alternative pain therapy reduction method was selected by the patient, nurses asked patients to rate their comfort level, using the Clinically Aligned Pain Assessment Tool (CAPA), a four-item scale ranging from intolerable, tolerable with discomfort, comfortably manageable, to negligible discomfort.21 The decision was made to switch from the NPRS to the CAPA tool to guide administration for nurses, prompting better conversation with patient about their discomfort. Thus, allowing the patient to specify their discomfort beyond a number. Patients were asked to indicate what type of discomfort they were experiencing (ie, pain, anxiety, nausea, insomnia or other discomfort). When a patient reported discomfort, they were offered a list of alternative therapy options from which to choose. In cycle 1, alternative therapy options included aromatherapy and visual relaxation DVDs. In cycle 2, the options included alternative methods as displayed in online supplementary appendix 1. One-hour post alternative therapy, patients were asked to re-assess their comfort level, using the same CAPA tool, and to report how likely they were to use the therapy again during times of discomfort. In the first cycle, sleep was noted but not rated using the CAPA tool. In the second cycle, if a patient was sleeping during post assessment, then the nurse noted this as ‘negligible discomfort’ on the assessment form. Other researchers have indicated improving patient sleep represents a natural starting point for improving comfort.22 Nurses also tracked how many patients refused alternative therapy.
Supplemental material
All patients who participated in alternative methods for pain and discomfort reduction had the potential to be surveyed more than once (ie, each day throughout their hospital stay). This was allowed due to factors such as an extended length of stay, different procedures completed throughout the patient’s stay and change in a patient’s condition during his/her admission or readmission.
Design
It was evident that the unit needed a standardised process to provide patients with appropriate alternative therapies. The project team consisted of content experts, frontline nursing staff and unit management. The team members met monthly and intermittently engaged with the hospital’s pain management team. The goal was to provide alternative comfort measures for patients who reported discomfort or who were already receiving pain relief medication but reported continued discomfort. The stakeholders agreed that the CAPA tool would be used to determine patients’ discomfort levels, and as a method by which alternative therapy was provided consistently. Any patient who reported lack of relief from discomfort was eligible to participate in the quality improvement project and was offered alternative therapies. Discomfort was defined by the patient’s perception of anxiety, pain, restlessness and irritability. The implementation of aromatherapy and visual relaxation DVDs was standardised across unit clinical staff. To support inter-professional collaboration, rounding providers were informed about the study and the methods of implementation. Additionally, nursing staff was educated on the process, and onboarding of new staff included orientation from key stakeholders.
Strategy
The aim of this quality improvement project was to increase comfort in hospitalised patients on a medical telemetry unit by using non-pharmacological interventions. The study spanned two PDSA test cycles.
PDSA cycle 1: In this PDSA cycle, the effectiveness of two alternative therapies, aromatherapy and visual relaxation DVDs, was tested. The patient was surveyed before and 1 hour post implementation of the alternative therapy. At the conclusion of this cycle, patients and frontline providers suggested the need for additional alternative therapies. Based on feedback, the project team collaborated with content experts to expand alternative therapy options available to patients.
PDSA cycle 2: During this cycle, the team offered additional alternative therapies to achieve a higher level of comfort among the patient population. A Comfort Menu was developed (see online supplementary appendix 1) with explanations of each intervention to help patients visualise options. For this cycle, two different nurses (one who was involved in the intervention and one who was not) surveyed the patient before and after the intervention to reduce potential nurse bias. The nurse who brought the patient the alternative therapy completed the initial survey. One hour after the intervention had been implemented, a different nurse asked the patient the same survey questions. Outcomes from this cycle established the need for hospital-wide implementation. Additionally, continued use of the Comfort Menu has been sustained through onboarding of new frontline providers.
Results
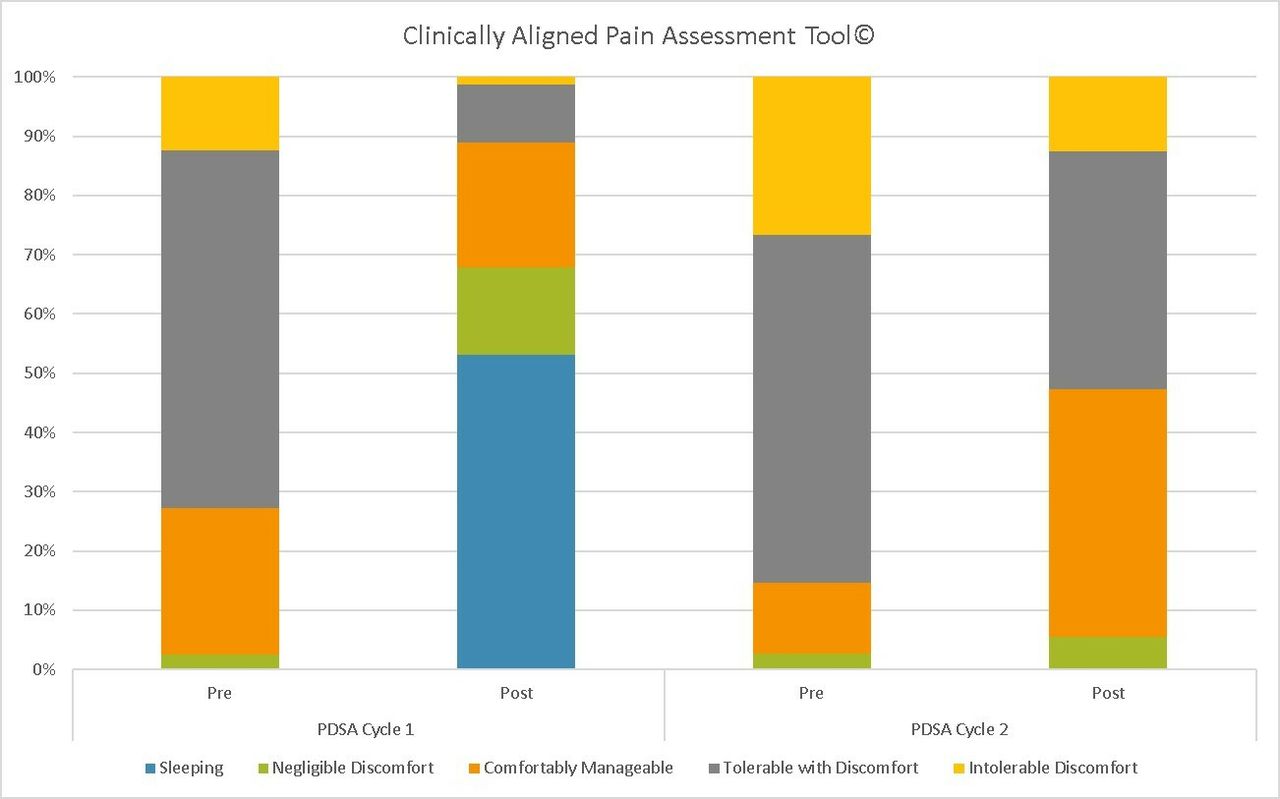
The main outcome measure was comfort level post alternative therapies for patients reporting discomfort on the inpatient telemetry unit. In cycle 1, 104 surveys were administered to 65 unique patients over a 12-week period. Of those patients, 25% were admitted with the common diagnosis of infection, and the most commonly reported discomfort type was pain (37%), followed by a combination of discomfort (ie, pain and anxiety) at 35%. In this cycle, 77% of those who were offered alternative therapy agreed to partake, and 2% of those who partook reported negligible discomfort, 25% reported being comfortably manageable, 60% reported tolerable with discomfort and 12% reported intolerable discomfort at the time of intervention. One hour post intervention, comfort was reassessed: 53% were sleeping on reassessment, 15% reported negligible discomfort, 21% reported being comfortably manageable, 10% reported tolerable with discomfort and 1% reported intolerable discomfort. For cycle 1, the outcome represented an 89% improvement in comfort level from the baseline assessment (see figure 1). Secondary to assessing comfort level, the project team asked if the patient would use the therapy again. Ninety-eight percent of respondents indicated positively about using alternative therapy to enhance comfort.
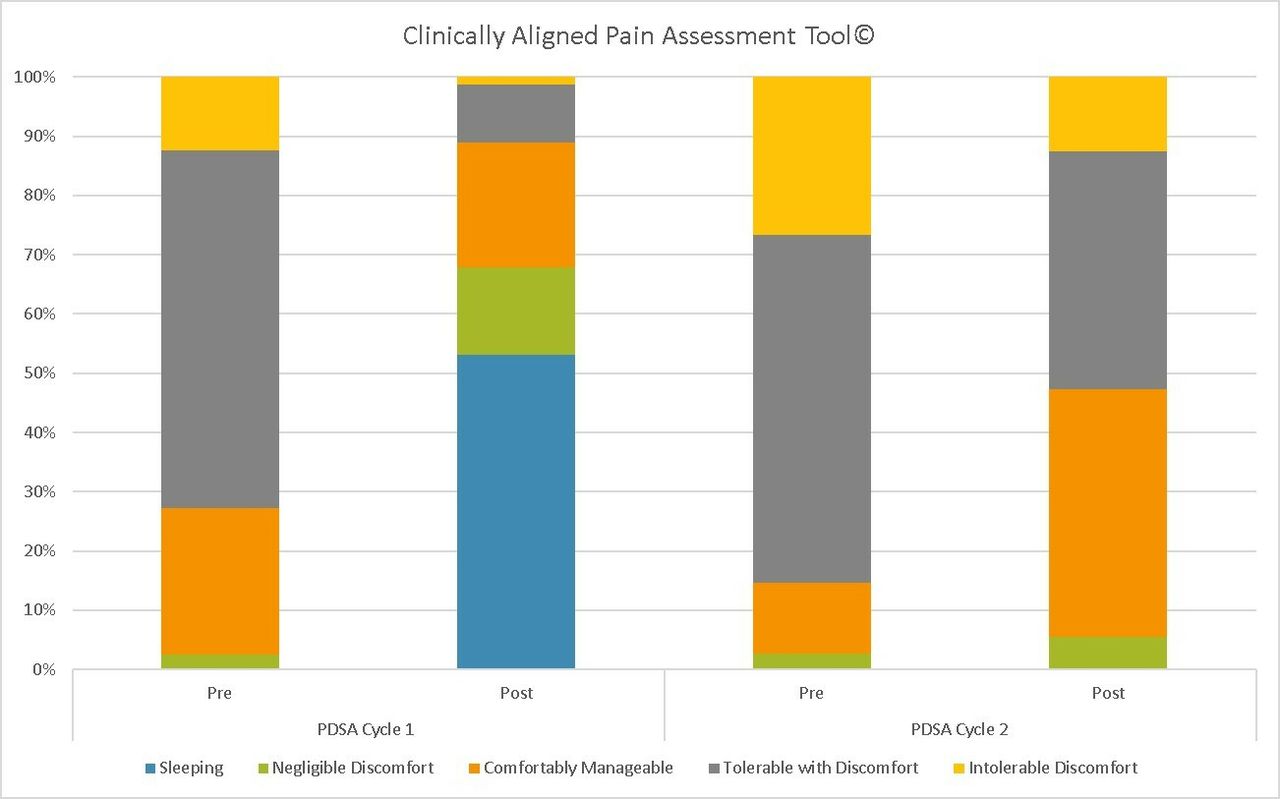
Clinically aligned pain assessment tool results for cycle 1 and cycle 2. PDSA, Plan Do Study Act.
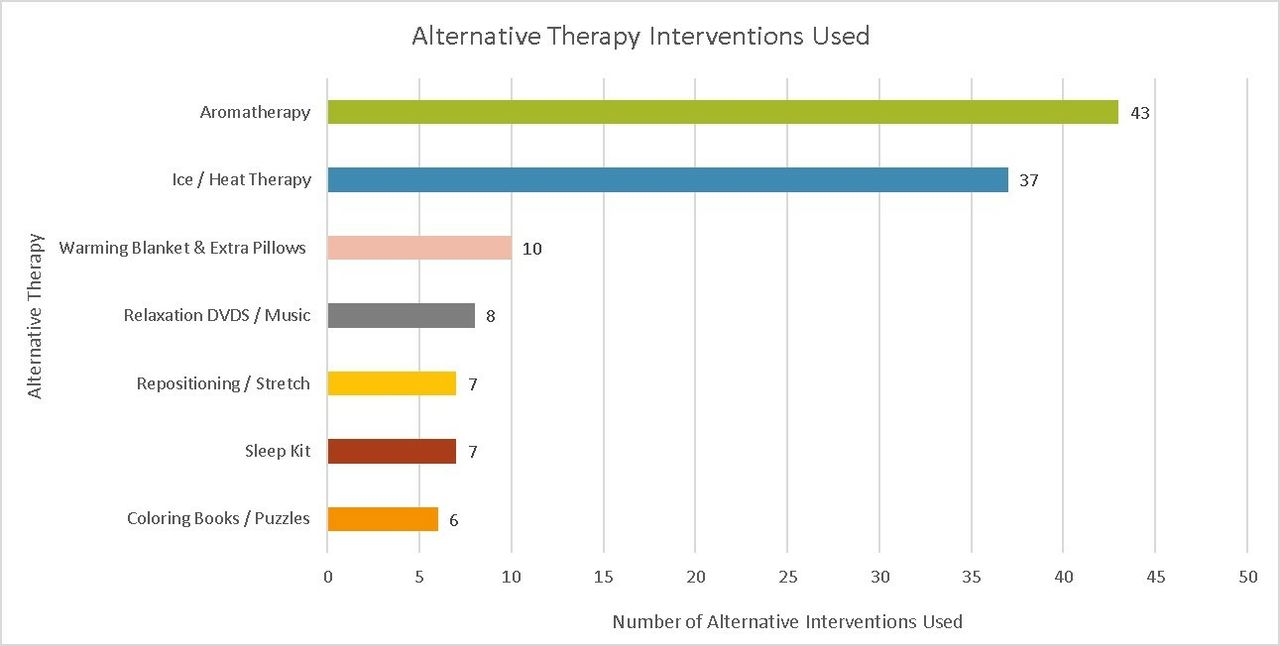
In cycle 2, the team broadened the approach to alternative therapy with the Comfort Menu. Change in the level of discomfort and control of comfort as reported by the patient was tracked. One hundred and one surveys were administered to 78 unique patients. Similar to the first cycle, the most common admission diagnosis was infection (21%), and the most common reported discomfort type was pain (78%). In cycle 2, 76% of patients agreed to participate in alternative comfort therapies, and the most commonly selected alternative therapy methods are displayed in figure 2. At the time of the intervention, 3% of the patients reported negligible discomfort, 12% were comfortably manageable, 59% reported tolerable with discomfort and 27% had intolerable discomfort. One hour post intervention, 6% stated negligible discomfort, 42% of patients reported being comfortably manageable, 40% reported tolerable with discomfort and 13% had intolerable discomfort. For this cycle, the outcome represented a 47% improvement in comfort from the baseline assessment. Additionally, when patients were asked how they perceived their change in comfort, 51% of patients reported their discomfort as ‘getting better’, and 70% stated the comfort menu options were effective in controlling discomfort. Furthermore, 89% of those who tried alternative pain interventions would do so again.

![[bmjoq-2018-000506supp001.jpg]](https://bmjopenquality.bmj.com/content/bmjqir/8/2/e000506/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
{kind=link}
{kind=link}
Most commonly selected alternative therapies from PDSA cycle 2. *Patients had the option to select more than one intervention. PDSA, Plan Do Study Act.
Lessons and limitations
Patients might have been surveyed more than once because there was no effective way of tracking whether or not a patient had been surveyed previously by another nurse. The survey instrument was also adapted to include the option ‘sleeping’ in the first cycle; however, this was not included in the second cycle because it was considered ‘negligible discomfort’. Lastly, there was inconsistent use of specific brands of aromatherapy oil throughout the study.
Similar to the first cycle’s limitation, the second cycle had no effective method of tracking if a patient had been surveyed previously by another nurse. Another challenge was keeping the visual relaxation DVDs consistently available because items were lost or inadvertently taken home by patients. Furthermore, there was also a limitation of the inability to stock and source aromatherapy oils in house to ensure supply consistency. This inconsistency was related to the aromatherapy oils becoming available across all hospital units. The project team attempted to notify materials management of this house-wide expansion in advance but the oils were placed on backorder.
In both cycles, patients were initially reluctant to participate in alternative therapies instead preferring pharmacological treatment options because of their unfamiliarity and lack of exposure to non-pharmacological therapies. However, in the second cycle, the team benefited from training provided by specialists in relaxation and alternative discomfort relief on how to discuss alternative therapy options with patients. Additionally, a visual menu proved helpful for patients when selecting potential non-pharmacological interventions and enhancing exposure towards alternative therapies. Finally, our project team recognised that non-pharmacological comfort measures were not always available to the patient following discharge from the hospital, and further data are needed on patients’ ability to sustain use of alternative therapy post discharge.
Conclusion
The multi-cycle QI project was successful in relieving patient discomfort by providing alternative therapies to inpatient, progressive care patients who reported little to no relief in discomfort from prescribed analgesics and adjuvant agents. Bridging off the success of the first cycle, a Comfort Menu with a greater variety of pain relief options was created, successfully implemented and well received by patients. The pain relief options were offered at no cost to the patient as most of the tools and supplies used were donated or covered in the hospital unit budget. Patients demonstrated tolerance of their discomfort when using alternative modalities and were highly likely to use these alternative comfort therapies again. This project has already gone through two PDSA cycles and has proven sustainability. Ten months post cycle 2, aromatherapy was implemented across all units of the hospital with support via development of a procedure. After the completion of cycle 2, external grant funding was awarded to support both the continuation of unit-based comfort offerings and the maintenance of the project. Future efforts will be focused on decreasing pharmacological therapies for the relief of pain and evaluating the effectiveness of pharmacological interventions in the relief of patient discomfort. Additionally, efforts will be aimed at implementing the use of all Comfort Menu interventions throughout the health system. Processes will be developed to partner with prescribing providers to integrate these alternative treatment modalities into standard practice.
In summary, this project is timely as supported by a highly publicised opioid epidemic in this country. In a period where federal government officials are providing stepwise approaches to pain control, continued evaluation and more projects like this one are pivotal in having impact on this epidemic. This project demonstrates successful implementation of alternative therapies and suggests non-pharmacological treatments for pain and discomfort can be an integral part of a comprehensive treatment approach.23 Future studies should further evaluate alternative therapies as an adjuvant to pharmaceutical, physical and exercise therapy, and cognitive behavioural therapy, especially in response to the Surgeon General’s call to end the opioid epidemic.24
Acknowledgments
Preliminary results were accepted as an abstract at the Annual Conference of the Vizient/AACN Nurse Residency Program held in March 2017, the RNovator KC 31st Annual Visions Symposium held in November 2017 and the 31st Annual Visions Symposium held in March 2018.
The authors thank Melanie Simpson, Sara Hocking, Jennifer Surprise, Noreen Thompson, Caroline Black Jenn Ray, Sarah Larson and Moira Mulhern for their invaluable feedback and support for this project.
References
Footnotes
Contributors MM, MS, SW, MW, AA, BL and TB made substantial contributions to the conception and design, acquisition of data, analysis and interpretation of data. All authors drafted and revised the manuscript for important intellectual content. CS, CG and MJ made substantial contributions to the submitted manuscript by assisting with the acquisition of data, analysis and interpretation of data, drafting of the manuscript, statistical analyses and critical revisions of the manuscript. All authors read and approved the final manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The quality improvement protocol was approved by the Institutional Review Board of the University of Kansas Medical Center.
Provenance and peer review Not commissioned; externally peer reviewed.