Article Text

Abstract
Kidney transplant patients in our regional centre travel long distances to attend routine hospital follow-up appointments. Patients incur travel costs and productivity losses as well as adverse environmental impacts. A significant proportion of these patients, who may not require physical examination, could potentially be managed through telephone consultations (tele-clinic). We adopted a Quality Improvement approach with iterative Plan–Do–Study–Act (PDSA) cycles to test the introduction of a tele-clinic service. We codesigned the service with patients and developed a prototype delivery model that we then tested over two PDSA improvement ramps containing multiple PDSA cycles to embed the model into routine service delivery. Nineteen tele-clinics were held involving 168 kidney transplant patients (202 tele-consultations). 2.9% of tele-clinic patients did not attend compared with 6.9% for face-to-face appointments. Improving both blood test quality and availability for the tele-clinic was a major focus of activity during the project. Blood test quality for tele-clinics improved from 25% to 90.9%. 97.9% of survey respondents were satisfied overall with their tele-clinic, and 96.9% of the patients would recommend this to other patients. The tele-clinic saved 3527 miles of motorised travel in total. This equates to a saving of 1035 kgCO2. There were no unplanned admissions within 30 days of the tele-clinic appointment. The service provided an immediate saving of £6060 for commissioners due to reduced tele-clinic tariff negotiated locally (£30 less than face-to-face tariff). The project has shown that tele-clinics for kidney transplant patients are deliverable and well received by patients with a positive environmental impact and modest financial savings. It has the potential to be rolled out to other renal centres if a national tele-clinic tariff can be negotiated, and an integrated, appropriately reimbursed community phlebotomy system can be developed to facilitate remote monitoring of patients.
- chronic disease management
- control charts/run charts
- patient-centred care
- Pdsa
- quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
One in 10 people in England live with chronic kidney disease (CKD),1 and around 32 000 people have a functioning kidney transplant in the UK.2 Patients who have had kidney transplants need regular specialist monitoring commissioned by National Health Service (NHS) England.3 This is routinely done at face-to-face appointments at approximately 3–4 monthly intervals in 52 regional renal centres across England. Each centre serves patients from a large geographical footprint and so patients routinely travel long distances to attend, having an impact on their lifestyle, income and environment.
The number of people with a functioning kidney transplant is increasing, placing heavier demands on renal services and particularly on outpatient capacity. This will require increased funding at a time when the NHS is working under unprecedented financial constraints. Furthermore, healthcare organisations have a duty to deliver improvements in quality, convenience and environmentally sustainable service (eg, reduction in CO2 emissions). For these reasons, there is an increasing focus on delivering care closer to home.4
North Bristol NHS Trust (NBT) Renal Unit covers an area extending to a radius of up to 80 miles for kidney transplant patients. Therefore, some patients have to travel large distances to attend appointments with associated costs both in terms of travel and productivity losses, such as time off work or leisure activities as well as environmental impacts. A significant proportion of these patients have stable kidney function but need continued specialist monitoring and could potentially be managed through telephone consultations (referred to as ‘tele-clinics’).
The project aimed to establish a tele-clinic service for routine monitoring of kidney transplant recipients over a 12-month period. This was based on patient experience reports to the renal unit commenting about difficulties with travel and parking for follow-up appointments. A survey of 96 renal transplant patients suggested that 59% of patients would consider taking up the option of a tele-clinic appointment. A detailed semistructured interview of each of the 11 patients from a pilot tele-clinic in December 2014 was undertaken by an evaluator independent of the quality improvement team to get patient feedback. The interviews were recorded, transcribed and analysed under broad themes to inform us of the tele-clinic service model and the patients’ perception of the benefits and risks of tele-clinics (unpublished). The general consensus was that the telephone consultations were a good idea as an addition to regular face-to-face appointments. Most of the patients suggested that they would be happy to have every other appointment as a tele-clinic but would not want all their appointments replaced in this way. It was felt that they liked the reassurance of being physically ‘seen’ by a specialist.
Background
Before proceeding with tele-clinics, we conducted systematic searches to identify potentially relevant studies that supported the safety and acceptability of tele-clinics for renal transplant patients and found two non-comparative evaluations. A report of 3 years’ experience from one UK centre that uses a tele-clinic for kidney transplant recipients concluded that if implemented appropriately, the use of tele-clinics for the follow-up of renal transplant recipients is safe and confers environmental benefits.5 However, no formal evaluation of this service has been conducted. A systematic review of the use of tele-health in nephrology concluded that although tele-health applications (not restricted to tele-clinics) are currently being used successfully in the management of patients with CKD, compared with other chronic disease areas, the development of tele-health applications appears underused and under-researched.6
Baseline measurement
As we had not used a tele-clinic model before, we agreed that our first PDSA cycle would form our improvement baseline and a range of comparative measures such as attendance and time taken could be used to compare performance with the standard delivery model.
We agreed to collect several process measures, outcome measures and balancing measures after each tele-clinic (table 1). It was recognised that undertaking blood tests in the community prior to the tele-clinic appointment would improve the effectiveness of the consultation and also reduce the need for any further follow-up telephone consultations to discuss blood test results. We constructed a driver diagram to highlight our working model of the key drivers for change and to organise the improvement ideas. Our aim was to understand the different processes that need to be put in place in the primary–secondary care interface to set up the service and also to ensure that the blood test results are available to the clinician at the time of tele-clinic consultation. The process of undertaking blood tests prior to the tele-clinic was a significant departure from face-to-face appointments where blood tests are performed in the clinic, and the results were reviewed by the specialist after the clinic. Therefore, we collected information from four face-to-face clinics to ascertain the baseline percentage of blood test results that are available and that correct (appropriate) tests have been ordered (96.5%). In part, the project aimed to reduce the number of patients not attending their face-to-face clinics by offering a tele-clinic option. Therefore, in the period August–October 2016, we analysed the number of patients who did not attend face-to-face clinic (6.9%).
Description of quality improvement project measures
The allocated time for face-to-face clinic appointment currently is 15 min. We anticipated that although tele-clinic consultation may require less time due to lack of need for physical examination, this could be balanced out by the lack of visual cues necessitating more in-depth questioning and prolonged consultation time during a tele-clinic. Therefore, we collected the average length of consultation time for tele-clinics but included only time spent on the phone for two reasons. First, patients suitable for tele-clinics and those who opt to do tele-clinics are less likely to be complex clinically compared with face-to-face clinic patients and so may require less time for additional tasks in clinic such as case notes review or following up investigations. Second, additional time may be required to chase blood test results for tele-clinic patients if they are not accessible on the renal IT system on the day and so may not truly reflect the time spent undertaking telephone consultations.
Design
This project was codesigned with patients throughout, using surveys, semistructured interviews and overarching programme governance structures. In addition, two patient representatives were active members of the codesign team and contributed to the improvement ideas and development of the improvement measures and helped to operationalise the service through development of patient information leaflets and questionnaires. In collaboration with West of England Academic Health Sciences Network (WEAHSN), we held a multidisciplinary workshop in December 2015 with patient representatives, renal consultant colleagues, renal administrative team, central outpatients booking team, general practitioners (GP), transplant nurse specialists, quality improvement experts from WEAHSN to process map the potential new care pathway for tele-clinics and capture improvement ideas (figure 1).

Process map for tele-clinics. GP, general practitioner; NBT, North Bristol NHS Trust.
We negotiated a local tariff of £188 compared with face-to-face clinic tariff of £218 with NHS England for an initial pilot project between August 2016 and July 2017. Blood tests were required to be undertaken ahead of the tele-clinic at the local GP surgery, but we were unable to negotiate a payment to GP surgery with local Clinical Commissioning Groups (CCGs) for this additional activity due to lack of engagement from CCGs. However, we anticipated that the patient eligibility and demand for the tele-clinic service will mean that only 1–2 patients per month per GP surgery will require this service and therefore should not unduly burden the local phlebotomy services at the GP surgery. The project lead, through close liaison and through newsletters to GP groups and medical committees was able to raise awareness and secure buy-in to undertake blood tests for the project.
The tele-clinic intervention was designed to have the following main features:
Patients judged suitable for tele-clinics by their specialist would be offered a telephone clinic appointment during which their progress, symptoms, blood test results and blood pressure (BP) measurements would be discussed and advice given. Patient eligibility criteria were developed by renal consultants at NBT based on the consensus that stable patients were unlikely to require physical examination or close monitoring in secondary care more frequently than every 3–4 months. For this pilot, we selected stable kidney transplant recipients who had a functioning kidney transplant for at least a year; had not had any transplant rejection episodes; had not started any new immunosuppression medications in the preceding 6 months; had a rate of decline in glomerular filtration rate that was <5 mL/min/1.73 m2/year; had agreed to alternate tele-clinics and face-to-face clinics; and did not have hearing or learning difficulties that could affect telephone consultation.
Patients were invited to opt-in during routine face-to-face clinic appointments. We created an electronic flag on our renal IT system to identify those who refused the offer and the reasons for not taking up the offer. Those who chose to do tele-clinics were booked in to a tele-clinic as the next follow-up appointment.
The tele-clinic would be offered to patients on an alternating basis with their face-to-face appointment based on feedback received from the qualitative interview from a pilot clinic as described above.
These patients would be sent an appointment invitation letter with instructions to get blood tests done ahead of the tele-clinic and encouraged to measure BP either at home (self- monitoring through automated BP devices) or at their GP surgery. After several deliberations with the laboratory teams and GPs, it was agreed that a blood test form with instructions on what blood samples and what tubes the blood samples needed to be sent in would be incorporated in the clinic appointment letter. Some of these blood tests were standard for all patients, and they were preselected on the form. As different patients were on different immunosuppression medications for their kidney transplant, measurements of immunosuppression drug level were not preselected but required patients or the phlebotomists at GP surgery to select them at the time of sampling. We also created a unique location code ‘NBTRT’ to inform the laboratories that the samples originated in primary care in relation to tele-clinics undertaken by NBT.
We agreed a standard operating procedure with all seven pathology labs in the region (NBT; University Hospital, Bristol [UHB]; Royal United Hospitals, Bath [RUH]; Musgrove Park Hospital, Taunton; Yeovil District Hospital, Yeovil; Weston General Hospital, Weston; and Gloucestershire Royal Hospital, Gloucester) so that results from samples with this location code were forwarded to NBT renal team rather than to GPs to ensure that these results were adequately acted on and to reduce additional workload for GPs in dealing with any abnormal results. The clinical laboratory systems in NBT, UHB, RUH and Weston are electronically linked to the renal IT system and results were automatically downloaded. Those in Yeovil, Taunton and Gloucester were not electronically linked and therefore relied on paper copies of results to be forwarded to renal unit to be manually entered by the renal administration team.
Initially, the telephone clinics were delivered by one consultant, but this was rolled out to six consultants delivering tele-clinics by the end of the project.
Patient and public involvement (PPI)
We describe the involvement of patients in this project according to the GRIPP2 (Guidance for Reporting Involvement of Patients and the Public)short-form recommendations for reporting PPI involvement in research.7 Overall, patients contributed to the project in three main ways: (1) exploration of patient need and proof of concept for the clinic, (2) patient feedback and input into the improvement cycles and (3) project governance.
Exploration of need and proof of concept
Patients were initially involved in this project to understand their current experience of the service and to better understand the impact that travelling to an outpatient appointment had on their lives. This was undertaken to ensure that the project focused on improving patient experience and improving people’s lives. To do this, we undertook an initial paper-based survey of 96 patients. We undertook a more detailed semistructured interview of 11 of the participating patients from the pilot tele-clinics (as described in the background section). These interviews generated very rich data and helped to demonstrate to service managers and commissioners that patients were articulating a need for such a service and preferred the flexibility of this compared with the normal service model. This feedback helped to refine the improvement ideas generated in the workshop and refine the methodology of the PDSA cycles for the tele-clinic.
Patient feedback and input into the improvement cycles
We recruited two kidney transplant recipients to our project from our existing patient panel who were involved in other research and service development projects at our centre. These two patient members participated in the initial workshop (as described above) and contributed to the development of the driver diagram, articulating the patient’s perspectives and generating improvement ideas. They made a significant contribution to the development of the quality improvement project measures using lived experience to test the relevance of the process, outcome and balancing measures.
They supported the design of the patient information leaflet and the tele-clinic appointment letter, checking that all the instructions to record home BP and undertake blood tests in primary care were relevant and easy to understand. They provided feedback and contributed to the development of the patient satisfaction questionnaire that was administered to all patients participating in the tele-clinics. They also provided further input to revising the content of the tele-clinic appointment letter with instructions based on feedback received from other patients through the patient satisfaction questionnaire.
The two patient members were invited to coauthor this report but declined.
Project governance
Patients were also included in the governance of the programme through Bristol Health Partners, working in partnership with People in Health West of England (www.phwe.org.uk).
People in Health West of England is an innovative PPI collaborative that brings together patient experience across a range of organisations striving to undertake transformational change and research.
Progress on the project was discussed with the core patient members at regular steering group meetings under the auspices of the Bristol Health Partners Board.
Strategy
This project had two parallel PDSA improvement ramps, with multiple PDSAs contained within each.
PDSA improvement ramp 1: close management of tele-clinic set up
As patients had the choice of opting in for the tele-clinics, it was difficult to predict the demand for the service. We, therefore, decided to set up the clinic as and when required depending on the demand. Patients were added on to the waiting list on the patients booking system, and a clinic was created as required. Between August 2016 and December 2016, our first improvement ramp tested close management of these processes required to deliver tele-clinics. The PDSA tests included:
Appointment bookings carried out by renal access coordinator.
Specialist transplant nurse having regular engagement with patients to ensure that they had conducted blood tests and BP monitoring.
One consultant undertaking the tele-clinic at a frequency of one a month.
Throughout the pilot, we measured how many patients’ blood test results had been produced correctly. Our criterion for a ‘correct’ result was one that included all tests including immunosuppression drug levels requested. As the blood test results were conducted in primary care (rather than being done at Southmead Hospital), there was reliance on both the patient and the professional taking the blood test to follow the instructions in the appointment letter. As this was new for primary care professionals and patients, the project team conducted several PDSA cycles to improve the instructions to GP surgery on blood test form within the appointment letter to undertake blood tests. This was based on feedback from patients and discussions with GP surgery where blood tests were not performed correctly as required.
For the tele-clinics to be viable, it was essential for the specialists to be able to see the blood test results during the consultation. This relied on pathology laboratories around the region being sufficiently well linked to NBT’s IT systems for results from samples sent by GP surgery to appear in time for the tele-clinic. There was close liaison with regional laboratories that were not electronically linked to NBT to ensure that blood test results were forwarded appropriately to the renal unit. A result was defined as ‘available’ if it was available through the renal IT system or the NBT Clinical Laboratory system. The clinician could still access results that were not visible on the renal IT system by calling the local laboratories. However, this required additional time spent during the tele-clinic chasing the results.
PDSA improvement ramp 2: embedding tele-clinic service
Between January 2017 and July 2017, our second improvement ramp tested a more distributed model of managing tele-clinic service. Main PDSA cycles included testing:
Additional consultants conducting tele-clinics. A second consultant contributed to tele-clinics from January 2017 to March 2017, and four additional consultants joined in from April 2017.
Frequency of clinics increased to two per month.
Bookings done by NBT Outpatients Central bookings team.
Medical secretaries ensuring that blood test results were available on renal IT system 48 hours before tele-clinic and contacting the local laboratories for results if required.
Results
Patients signing up to tele-clinics
In total, we initially approached 389 eligible kidney transplant patients. Of these, 185 (47.6%) agreed to take part. The most frequent reasons given for declining to take part were: preferring face-to-face interaction and not having issues with accessing the hospital for face-to-face appointments. Table 2 summarises the reasons why the remaining 52.4% patients declined signing up to tele-clinics.
Reasons for patients not taking up tele-clinics
Percentage of patients that did not attend
A percentage of 2.9 (n=6) of tele-clinic patients did not attend their tele-clinic appointment compared with 6.9% for face-to-face clinics between August 2016 and October 2016. Reasons for non-attendance at tele-clinics were investigated and were explained by individual factors (eg, patient that regularly did not attend face-to-face clinics, also did not attend tele-clinic) rather than being linked to any features of the intervention or the changes introduced and tested through PDSA cycles.
Blood test quality
During the pilot, overall 74.8% of blood tests were ordered correctly. Table 3 shows the proportion of blood tests undertaken correctly in the different time periods. The blood test quality in the final PDSA cycle was 90.9% (figure 2). This is slightly lower than the figure for face-to-face clinics (96.5%). Unlike the face-to-face clinic, where blood tests are done by few trained renal phlebotomists, blood tests are undertaken by multiple staff members within several GP practices. We acknowledged the inherent limitations in this model and accepted that the blood test quality for tele-clinics is unlikely to match that for face- to-face clinic results. The results that were often missed or incorrectly done were the immunosuppression drug levels. A missing single immunosuppression drug level does not adversely affect clinical decision making as we mostly rely on trends in immunosuppression drug levels to adjust dosing. Follow-up of these patients with missing results in subsequent face-to-face clinics did not identify any adverse events relating to incorrect results.
Summary of PDSA cycles to improve blood test quality
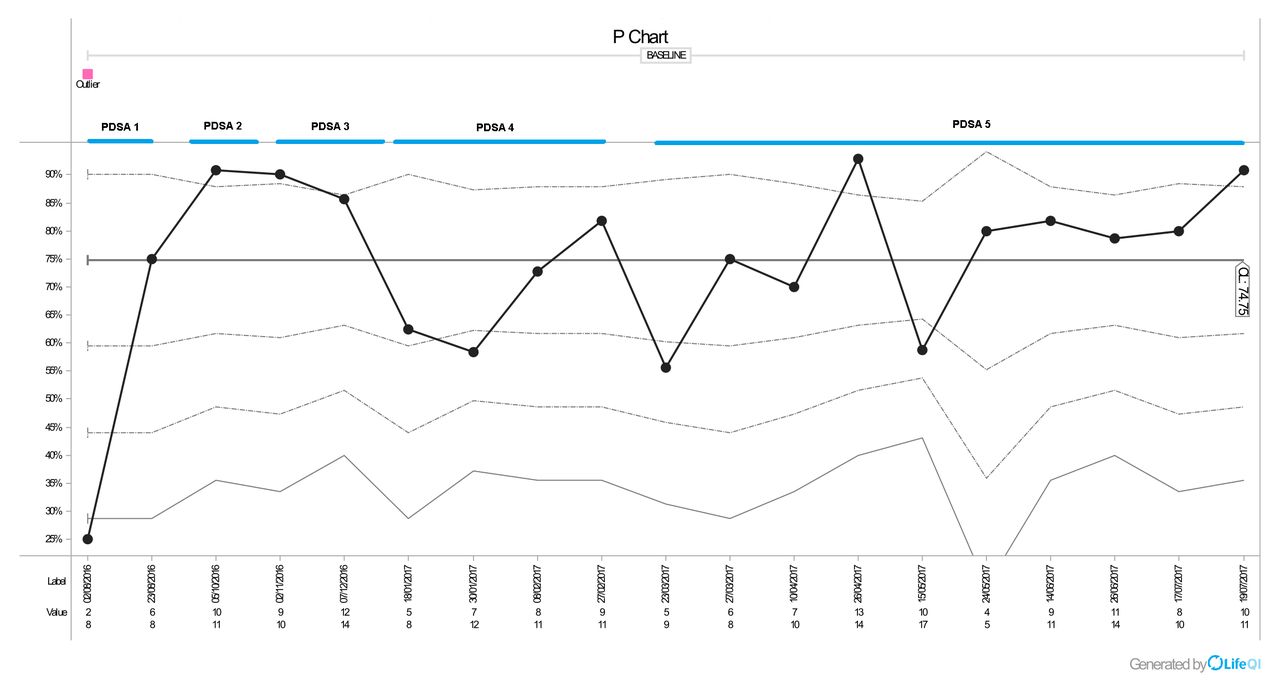
Run chart showing blood test quality. PDSA, Plan–Do–Study–Act.
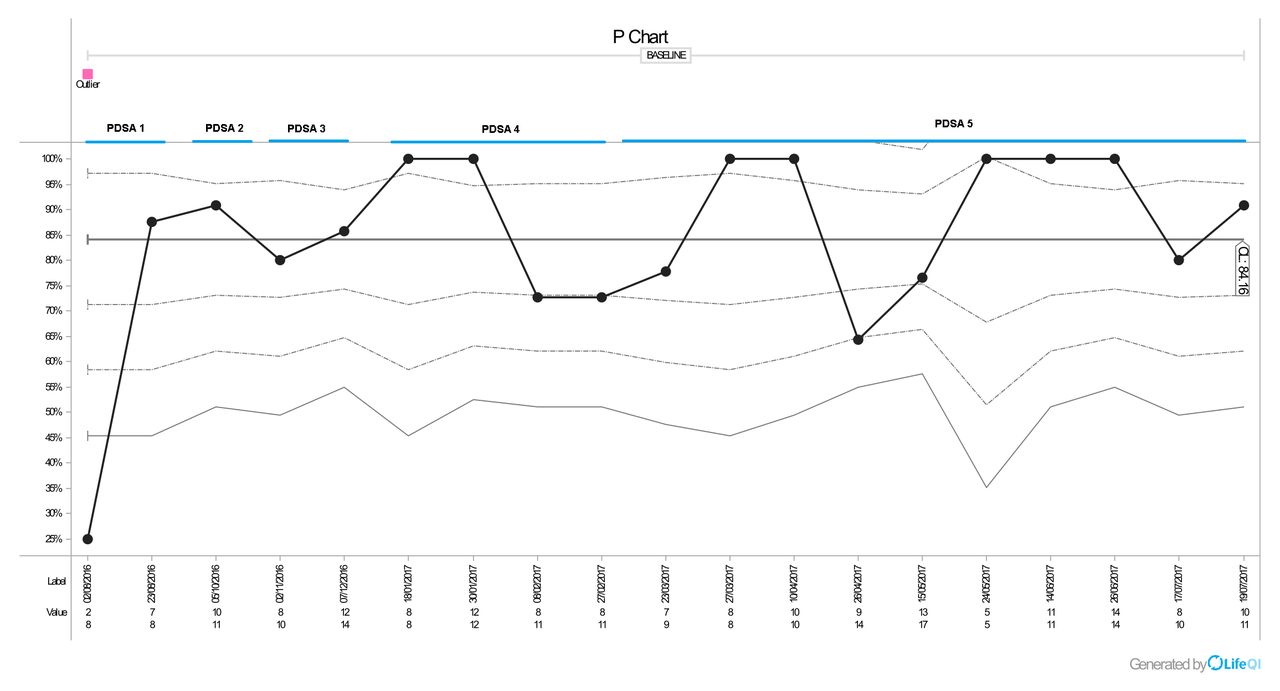
Blood test availability
At the start of the project, results from all laboratories in NBT, UHB, RUH and Weston were accessible through renal IT system. Towards the end of the QIP (Quality Improvement Project) in July 2017, we were able to get the remaining laboratories in Taunton and Yeovil, electronically connected, and results were automatically downloaded onto the renal IT system. Gloucester was still not electronically linked, and we relied on paper copies of results to be sent to us. The main reasons for results not being visible were: blood test forms (with location code NBTRT) not accompanying the samples sent by GP surgery. Instead locally generated labels used by primary care staff on blood samples and therefore results forwarded back to GPs and not to renal unit. There was a lack of awareness of protocol for processing results accompanied by blood test form with NBTRT location code among some laboratory staff. On average, 84.4% of blood test results were available for the tele-clinics during the entire project but the final PDSA cycle showed an improvement to 90.9% (figure 3).

Run chart showing blood test availability. PDSA, Plan–Do–Study–Act.
Length of tele-clinics
Across all tele-clinics, the average call length was 10.3 min (figure 4). The figures from January 2017 are an average for all consultants who have done the tele-clinic. There is a trend towards reduced length of consultation time over the course of the project. This could be due to the fact that clinicians became more familiar with the conduct of the tele-clinic. We also had developed a standard tele-clinic template, which was used by clinicians as an aide memoire during the consultation process. The spike observed in April 2017 was associated with another consultant colleague undertaking the tele-clinic for the first time.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Run chart showing average length of call during each tele-clinic.
Patient experience
There were 97 responses to the patient satisfaction survey (57.7% response rate). Surveys were sent by post and through the Survey Monkey website. A summary of findings is presented in table 4. A rating of ‘6’ is the highest level of satisfaction, while ‘1’ is the lowest. The ‘0’ was chosen by a small number of patients when a statement was not relevant (eg, if they had not been able to arrange a blood test). A percentage of 97.9 of respondents were satisfied overall with their tele-clinic. Positive comments about the experience focused on the quality of the conversation itself and the convenience of conducting the clinic by phone. More negative comments tended to focus on what might be lost through telephone interaction rather than face-to-face sessions or specific comments about challenges in arranging blood tests.
Summary of patient ratings of the tele-clinic service
Estimated reduction in CO2 emissions
Among those who responded to the survey, the average distance normally travelled by patients to their face-to-face appointments was 36.4 miles. The tele-clinic saved 3527 miles of motorised travel in total. This equates to a saving of 1035kgCO2.8 The actual reduction in travel distance and CO2 emissions will be much higher than this given that the response rate to patient survey was only 57.7%.
Patients requiring urgent follow-up within 1 month tele-clinic
This measure was in place to ensure the safety of the tele-clinics. There were no unplanned admissions to hospital or urgent follow-up outpatient visits at NBT for the patients taking part in the tele-clinics. However, we do not have data to verify if the tele-clinic patients had required additional visits to their GPs that may not have been required if they had been seen in a face-to-face clinic.
Cost of service
The tariff for tele-clinics was £188; this is £30 less than the standard face-to-face rate of £218. The service provided an immediate saving to commissioners of £6060, but this excludes the blood sampling costs in primary care. Generating a definitive estimate of cost saving for the tele-clinic project has proved challenging due to the way that activity and costs are recorded in secondary care. Isolating the total specific costs for a face-to-face clinic versus a tele-clinic has not been possible. This would be a valuable area for future research.
Inappropriate patients booked into tele-clinic
We have been testing whether patients who do not meet the eligibility criteria have been booked into tele-clinics. In total, three inappropriate patients were booked into the tele-clinics. One patient was diagnosed with dementia and so was no longer eligible. One patient was due to a booking error and had been seen for a face-to-face clinic the week before. One was a patient that regularly did not attend face-to-face clinic appointments and did not pick up their phone call.
Lessons and limitations
PPI involvement was crucial to ensure that the new service being offered was fit for purpose as this was intended to improve patient experience. The semistructured interviews highlighted the importance of offering patients the choice to opt-in for tele-clinics and to maintain some of the appointments as face-to-face visits and hence the provision of alternating tele-clinics and face-to-face appointments. The patient members within the quality improvement team were kidney transplant recipients themselves attending face-to-face appointments at our centre and therefore provided valuable insight in codesigning the service, logistics of undertaking blood tests in primary care and the use of language that was understood by patients with kidney disease in the clinic appointment letter and patient information leaflet. In addition to the experienced patient members’ input in to the project, we found the feedback that we collected through our satisfaction survey informative and provided us a broader perspective of other patients’ experiences.
The success of the tele-clinics relied heavily on primary care’s willingness to conduct blood tests without a formal agreement for these costs to be reimbursed. Due to the small volume of patients per practice needing this service, it was possible to sustain this for the pilot. However, six GP practices decided not to support the pilot due to the lack of reimbursement. While efforts were made to explain the purpose and benefits of the pilot, we have not been able to engage with CCGs and GP surgery due to sustainability transformation plan reconfiguration and other competing priorities for the CCGs. Addressing this issue will be essential for the service to become embedded and sustainable long term as without consistent GP support, the service will inevitably lead to health inequalities.
We anticipated higher demand for tele-clinics (59%) based on patient survey than observed for this project (47.5%). This figure, gathered through this project, draws on a larger number of patients and can be used for more accurate planning of future tele-clinic services. We have also identified the reasons for patients declining tele-clinics. This gives a platform for future attempts to recruit suitable patients to tele-clinics.
While we have been able to identify several financial and efficiency benefits arising from the project, we have not been able to produce a definitive picture of the cost of tele-clinics versus face-to-face clinics. Collaboration with health economists might help to address this gap. In addition, while we failed to find any evidence that tele-clinics were associated with increased 30-day hospital admission or urgent follow-up visits in secondary care, this quality improvement project was never powered to detect such a difference. A much larger study, ideally a randomised controlled trial, would be required to provide far more definitive evidence of safety or equivalence between the two modes of delivery.
In addition, we were not able to collect data on additional GP consultations in-between the tele or face-to-face clinics. It is possible that a face-to-face clinic may detect early problems and deal with them thereby reducing future GP workload. However, it is also possible that face-to-face consultations generate more workload for GPs than tele-clinics. This requires further evaluation.
Conclusions
The project has shown that tele-clinics for kidney transplant patients are deliverable and well received by patients with a positive environmental impact. The project has also delivered modest financial savings for the NHS; however, the true financial picture for the wider health economy and the health economic benefits for patients and the environment has been hard to capture and would warrant further research. This model has the potential to be rolled out to other renal centres if a national tele-clinic tariff that is acceptable to all stakeholders can be negotiated, and an integrated and appropriately reimbursed phlebotomy service can be developed to facilitate remote monitoring of patients between primary and secondary care.
Acknowledgments
We would like to thank our patient representatives Guy Robertson and Brigid Dowsett for their contribution to this project. We are also grateful to Chronic Kidney Disease Health Integration team GP members Dr Sam Davies and Dr David Munson for their advice. We also would like to thank the Bristol Health Partners for providing project support time. We also would like to thank CLAHRC West for their support with undertaking literature search for this project. We are grateful to GP surgeries who have kindly facilitated blood sampling for this project without any financial reimbursement and to NBT renal consultant colleagues and administrative team for their support.
Footnotes
Contributors UPU developed the idea of tele-clinic, led the project and wrote the manuscript. OW was the project manager collecting and analysing data. YB-S contributed to the project set up and commented on the manuscript. ML, KA, AP and CD conducted the tele-clinics and contributed to data collection. DE and AB provided expertise on quality improvement methodology and commented on the manuscript.
Funding We would like to thank the West of England Academic Health Sciences Network for their quality improvement expertise and for funding this project.
Competing interests AP reports personal fees from Vifor Fresenius Renal Pharma, personal fees from Bayer GmBH outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.