Article Text

Statistics from Altmetric.com
Introduction
Nuclear myocardial perfusion imaging (MPI) is a robust tool for detecting coronary artery disease (CAD) and for cardiovascular risk assessment. The radiation from MPI may marginally increase the patient’s risk of a malignancy in the future. Patient-centred risk mitigation strategies such as individualised radiotracer dosing and stress-first imaging are recommended by both clinical practice guidelines and the Choosing Wisely campaign.1–3 Implementation of stress-first imaging may be impaired by inadequate staffing, concerns about safety or perceived disruptions to workflow. We sought to address these perceived barriers and determine if a simplified, stress-first protocol would be feasible at our facility.
Methods
We adopted a stress-first imaging protocol for all patients undergoing MPI at our facility in which no pretest screening was performed and all patients were considered eligible for stress-first MPI. In preparation for adoption, we sought input from all members of the nuclear cardiology team. Nurses, technologists, housestaff and faculty all provided their opinions about possible barriers to success. One of the most prominent concerns was availability of a physician who could review stress-first studies throughout the day on short notice in order to make the decision about performing rest imaging. This duty was assigned to our advanced cardiovascular imaging fellow who was, in turn, responsible for securing adequate physician staffing if he was not going to be available.
The stress-first protocol was to inject 0.4 mg of regadenoson followed by 9–13 millicuries (mCi) of Tc-99m*-tetrofosmin. CT attenuation correction was used for all studies and prone imaging was acquired when feasible. After acquisition, studies were reviewed by a physician who determined if the study was normal or if rest imaging was required. If necessary, rest injection/acquisition was performed 30 min after stress imaging with 37–45 mCi of radiotracer. We compared normalcy rate, radiation dose, rates of angiography and percutaneous coronary intervention (PCI), for two cohorts of consecutive patients. Cohort 1 underwent rest-stress imaging (17 July 2016 to 12 November 2016) and cohort 2 underwent stress-first imaging (13 November 2016 to 17 May 2017). Effective doses were estimated based on the activity administered.4 A normal MPI was defined as no evidence of ischaemia or infarction with a preserved ejection fraction. All MPI at our facility are read jointly by nuclear medicine, radiology and cardiology faculty. No blinding was performed. The primary goal of this project was for quality improvement and not as research. Based on VA handbook 1058.05, our facility made the determination that it does not qualify as human subjects research and therefore does not require institutional review board approval. Median radiation doses were compared with the Mann-Whitney U test and other comparisons were made using Χ2 test.
Outcomes
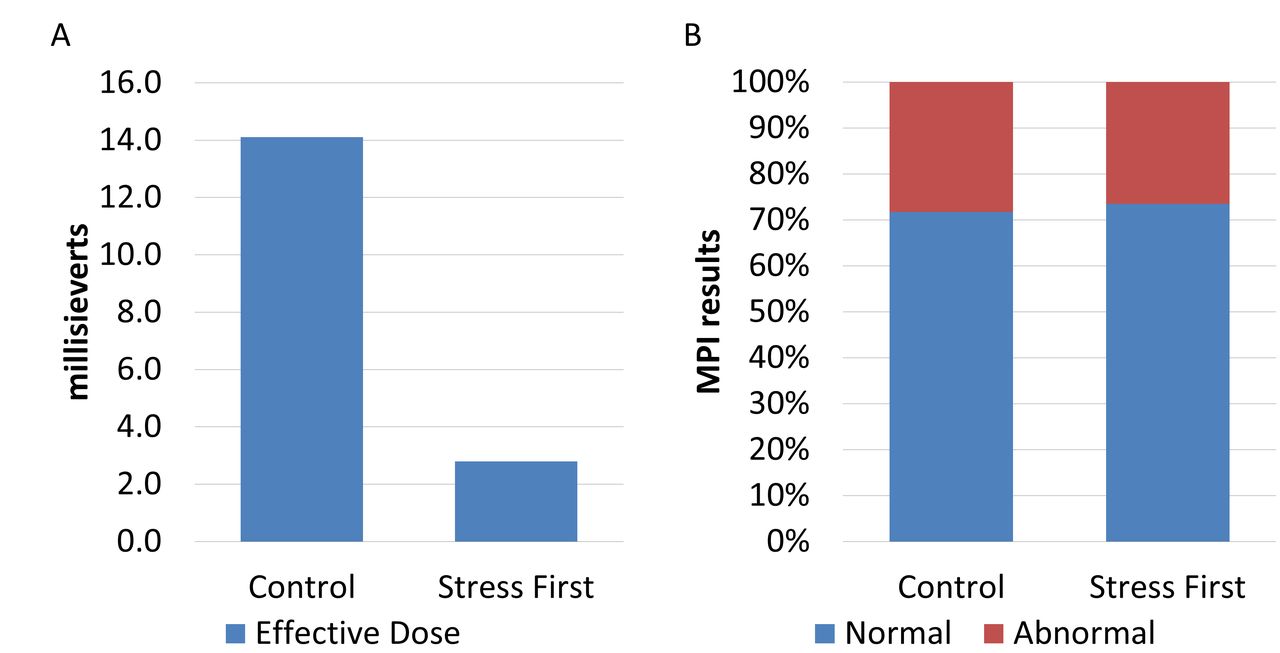
In the rest-stress cohort, 424 studies were performed of which 71.7% were read as normal. In the stress-first cohort, 716 tests were performed, 423 were stress-only studies (59.1%) and 293 were stress-rest studies (40.9%). In the stress-first cohort, the median dose was 2.8 millisieverts (mSv) compared with 14.1 mSv in the rest-stress cohort (p<0.0001). During the observed period, we estimate that 4780 mSv of effective dose were avoided (figure 1, panel A). The rate of normal studies in the stress-first cohort was not different from the rest-stress cohort (stress-first: 73.5% [526/716] vs rest-stress: 71.7%, p=0.54, OR 0.92, 95% CI 0.69 to 1.21) (figure 1, panel B). In the rest-stress cohort, three patients (1.0%) underwent coronary angiography and two patients (0.7%) underwent PCI. In the stress-first cohort, eight patients (1.1%) underwent coronary angiography and two patients (0.3%) underwent PCI.
{kind=link}
Radiation dose and proportion of abnormal tests. In panel A, the median estimated effective doses for the control and stress first cohorts are compared. In panel B, the proportion of myocardial perfusion imaging (MPI) tests considered normal and abnormal for the two cohorts are compared.
Discussion
We sought to evaluate the quality improvements associated with a stress-first MPI imaging protocol without prescreening of patients. The findings demonstrate that this imaging protocol is feasible and substantially reduces radiation dose.
Stress-first and stress-only protocols have been described in the medical literature for many years with a recent resurgence in interest.5 Compared with rest-stress imaging, stress-first appears to be safe, despite concerns about shine-through and artefacts from low-dose imaging.6 7 While our data in isolation are insufficient to demonstrate safety of this strategy, we did not observe any evidence of harm. Some prior studies on stress-first imaging have only enrolled patients at low pretest likelihood of CAD. Our project suggests that abnormal MPI, coronary angiography and PCI rates are similar for stress-first imaging and rest-stress imaging even in an unselected population.
We observed that 71%–74% of MPI were ‘normal’ however only 1%–2% of our cohort underwent subsequent coronary angiography. Explanations would include MPI that are only mildly abnormal (summed stress or summed difference scores under 5), those with infarction but no ischaemia, or those with abnormal ejection fraction. For many patients in these groups with abnormal MPI, invasive angiography may not be clinically relevant or indicated.
From a technical perspective, stress-first imaging is simple to perform; the key challenge lies in implementation. Barriers to implementation include physician and technologist scepticism, limited access to radiotracer deliveries, reduced reimbursement for not performing both stress and rest images and availability of a physician to read stress-first images promptly. Facilitators of implementation are comparatively weak and more of value to the patient than the practice: improved safety through reduced radiation dose and reduced time for the patient being scanned. This imbalance in barriers and facilitators can be seen in surveys of nuclear cardiology practices where stress-first imaging is the exception, not the norm. A recent study found that only 7.7% of MPI performed in North America were stress-first, compared with 84.4% stress-first performed in Europe.8
Implementation at our facility ultimately became possible through the commitment of physicians to read the studies promptly and a multidisciplinary implementation plan with our technologists. Software solutions including virtual private networking and remote viewing portals reduce barriers so that physicians should be able to review MPI studies as they are completed and determine if rest imaging is necessary. While external pressure from third-parties could require stress-first MPI in the future, we think the best way to encourage use of stress-first imaging is to continue to publicise the feasibility and benefits of this strategy.
Footnotes
Contributors DEW, RJ, DCW, VT and AW contributed to the concept of the investigation, critical revision of the manuscript, final approval for publication and agree to be accountable for all aspects of the work. RJ was responsible for primary data acquisition. RJ and DEW were responsible for data analysis and interpretation. DEW was responsible for the primary draft of the manuscript.
Funding This manuscript is result of work that was supported by resources of the Malcom Randall Veterans Affairs Medical Center.
Disclaimer DW had full access to the data and accepts responsibility for its integrity.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement A deidentified copy of the unpublished data from the project can be made available through a data sharing agreement with our host institution.
Patient consent for publication Not required.