Article Text

Abstract
Medication reconciliation in ambulatory care settings helps prevent adverse drug events. Patient involvement in the process is crucial, as clinicians must verify the reported medication history with other sources such as home medication lists or brown-bagged home medications provided by patients. However, only 47.8% of brain injury and stroke adult outpatients at Toronto Rehabilitation Institute, an academic rehabilitation hospital, bring their medications/medication lists to clinic visits. In turn, missing medication information impacts the clinic by causing delays in treatment and interrupted clinic flow. This project aimed to increase the percentage of patients who bring their medications/medication lists to 80% and decrease the impact on clinic visits caused by missing medication information to 10%. This was a controlled before-after study, with the outpatient rehabilitation assessment (OPRA) clinic as the intervention and the spasticity clinic as the control. The model for improvement was used as the project framework. Process mapping, Ishikawa diagrams, driver diagrams and patient surveys generated the change ideas. Verbal reminders during confirmation phone calls, written reminders and medication list templates were implemented. Data were collected on a biweekly basis and analysed using statistical control charts. After six Plan-Do-Study-Act cycles conducted over 49 weeks, both project aims were achieved. The percentage of OPRA clinic patients who brought medications/medication lists was 81.8% and the impact on clinic visits caused by missing medication information was 9.1% of clinic visits. Special cause variation was detected on the statistical control charts. Conversely, there was no special cause variation for the spasticity clinic (the control) for either aim. Lessons learnt include the importance of prolonged data collection when implementing interventions with long lag time, and that verbal reminders may not be effective for patients with cognitive impairments. Future efforts may focus on implementing the bundle of project interventions for the spasticity clinic.
- medication reconciliation
- ambulatory care
- healthcare quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
University Health Network-Toronto Rehabilitation Institute, University Centre’s (UHN-TRI, UC) neurorehabilitation clinic specialises in the treatment of patients whose functional abilities have been impaired by strokes and acquired brain injuries (ABI), and provides comprehensive spasticity management. It is the largest neurorehabilitation outpatient clinic in the city, and comprised 10 academic physical medicine and rehabilitation (PM&R) specialists and one clinic nurse who are supported by two different administrative teams—one for the outpatient rehabilitation assessment (OPRA) clinic which serves patient with strokes and ABIs, and another team for the spasticity clinic (online supplementary appendix 1). The patient population seen in the clinic has a complex mix of cognitive and physical deficits, and typically are prescribed medications from multiple specialists aside from their family physicians.
Supplementary file 1
It is difficult to start or recommend new medications, titrate existing regimens and most of all, ensure medication safety, without an accurate knowledge of patients’ current medications. As a result, the clinic staff spend their scarce time and resources calling patients’ pharmacies to search for information, and in some cases even delay treatment or defer treatment to patients’ family physicians.
As a result, a quality improvement (QI) project was initiated at the clinic to address this problem and to prepare for the eventual adoption of medication reconciliation. This QI project aimed that by 1 May 2017, the percentage of patients who bring their medication lists or medications (medication lists/medications) to their clinic appointments would be 80% or more. This aim was reached via consensus at a physician’s meeting prior to the start of the project. In addition, as judged from staff surveys, we sought to reduce the number of clinic visits where missing medication information affected clinic flow/staff workload to less than 10% of visits.
Background
Adverse drug events are common in the outpatient setting and have the potential for serious harm.1 2 Inaccurate information about patients’ medications can lead to inappropriate treatment and preventable adverse drug events.3 4 The WHO states in the ‘Standard Operating Protocol-Assuring Medication Safety at Transitions in Care’ that ensuring medication safety requires healthcare providers to have accurate knowledge of patients’ medications to ‘avoid omissions, duplications, dosing errors, and potential adverse interactions.’5
There is a large body of literature demonstrating that patients frequently lack accurate knowledge of their medications.6–9 This problem is compounded by the fact that patients may be prescribed medications by multiple specialists, so even medication lists from family physicians on referrals are frequently inaccurate due to the lack of system-level electronic medical records.10 11 One Canadian study demonstrated that 115 out of 120 participants attending a Geriatric Day Hospital programme had at least one discrepancy between the medication list from their family physicians and a medication list generated from a comprehensive medication reconciliation that included interviews with the patient and family members and a brown-bag review.10
Medication reconciliation has been shown across ambulatory care settings to help improve medication list accuracy.12–15 In one study, the completeness of medication lists more than doubled from 20.4% to 50.4% after the implementation of medication reconciliation in four academic internal medicine clinics. However, patient involvement in medication reconciliation is vital, as clinicians need to verify the reported medication history with other sources such as home medication lists or brown-bagged medications brought by patients.5 16
Many strategies to encourage patients to bring their medication lists or brown-bagged medications have been identified in the literature. The Agency for Healthcare Research and Quality (AHRQ) recommends in the ‘Health Literacy Toolkit’ that appointment cards, verbal reminders during appointment reminder calls, verbal reminders about and praise for bringing medications during office visits, posters in exam rooms and waiting rooms, bulletin board display of anonymous cases and free medication carrier bags be used.17 Similar recommendations exist in the ‘Assuring Medication Safety at Transitions in Care Implementation Guide’ by the WHO, and there are also additional recommendations of using videos, information sheets, medication list templates, medication list apps, patient portals and community-based pharmacy medication review programmes to help encourage patients to bring in up-to-date medication lists consistently.18
Several studies have used some or all the recommendations successfully to improve the frequency that patients bring their medication lists or brown-bag their medications to clinic. The family medicine practices in the study conducted by Weiss et al implemented all the recommendations in the AHRQ ‘Health Literacy Toolkit’, and the percentage of patients who brought all their medications to their clinic increased from 20.0% pre-implementation to 68.3% post-implementation.19 Nassaralla et al used written reminders on appointment letters, and verbal reminders during phone calls 1 day before appointments at an outpatient academic internal medicine clinic. There was an increase from 13.9% to 33% in terms of patients who brown-bagged their medications and/or brought an up-to-date medication list.12 Varkey et al instead only relied on written reminders on appointment letters, and mailed medication list templates to encourage patients attending an academic preventive and occupational medicine clinic to bring in home medication lists or medications as part of a medication reconciliation QI project. Of the 104 patients enrolled in the study, 5% brought in their home medication list at baseline compared with 52% after reminders and medication list templates were mailed.15
Measurement
The project used a family of outcome, process and balancing measures. The primary outcome measure was the percentage of patients who brought their medications/medication lists to their clinic appointments. The secondary outcome measure was the percentage of clinic visits with impact on clinic flow, staff workload and treatment due to patients not bringing their medication lists/medications. The definitions for impact on clinic flow, staff workload and treatment were determined through consensus by three physiatrists and a clinic nurse prior to use in the project (online supplementary appendix 2). During the project, three physiatrists, the clinic nurse and a medical student completed the manual data collection survey (online supplementary appendix 2) for at least two OPRA clinics and one spasticity clinic on a weekly basis.
Supplementary file 2
The process measure was the percentage of patients who receive a verbal reminder to bring medications/medication lists during confirmation phone calls, collected daily via the administrative staff’s self-report on their call lists. The administrative staff also tracked whether the call reached a person or went to voicemail.
As for balancing measures, the focus was the administrative staff’s perceptions of the change ideas implemented. A project team member attended the administrative team’s huddles once a week to solicit qualitative, open-ended feedback about the project’s change ideas. In addition, the NASA Task Loading Index (NASA-TLX)20 was administered to at least two administrative assistants before and after change ideas that impacted their workload.
To analyse the project data, statistical control charts were generated for the outcome and process measures, and interpreted using Institute of Healthcare Improvement rules.21 T-tests were used to assess the process characteristics for patients who did not bring medications/lists versus those who did. Descriptive statistics were used to analyse the administrative staff’s scores on the NASA-TLX. Qualitative feedback about the change ideas collected through huddles was analysed for themes.
Design
The Plan-Do-Study-Act (PDSA) method of QI was used as the project framework. The project team consisted of two physiatrists, an administrative assistant, clinic nurse and a medical student. In addition to examining data over time, the study used a controlled, before-after design to evaluate the effectiveness of the interventions. The OPRA clinic was used as the ‘intervention group’ and the spasticity clinic was the ‘control’ since they were affiliated with two different administrative teams. All four physiatrists in the spasticity clinic also work in the OPRA clinic, and the patient population served includes patients with cerebral palsy, multiple sclerosis and spinal cord injury in addition to strokes and ABIs. Approximately 15% of patients in the spasticity clinic are also followed in the OPRA clinic. The spasticity clinic uses the same physical clinic space and the same clinic nurse. It was therefore the best available control. All interventions were applied to the OPRA clinic only.
Initial diagnostics for the quality problem focused on consulting stakeholders. Semistructured interviews with a convenience sample of 11 consecutive patients who had not brought medications to a physiatrist’s (author MG) clinic from October to December 2016 asked patients, ‘why did you not bring your medications or a medication list to clinic?’ Their responses were then grouped into themes. A consultation session with clinic administrative and clinical staff was held over a lunch hour in September 2016 to generate a process map (online supplementary appendix 3) and an Ishikawa diagram (online supplementary appendix 4).
Supplementary file 3
Supplementary file 4
Through the interviews, 8 out of 11 patients reported that they had not been told to bring medication lists/medications, and the process map showed that patients indeed did not receive reminders about medication lists/medications close to their appointments. The Ishikawa diagram further highlighted that the written reminders given to patients were not conspicuous, and that patients did not receive reminders during confirmation phone calls. A driver diagram was then created for the quality problem, and change ideas were created based on the drivers (online supplementary appendix 5).
Supplementary file 5
To address the first two drivers of the quality problem, reminders were implemented. Confirmation phone calls were made to patients 2 days before their appointment, and a script including a reminder to bring their medications/medication lists was developed with the administrative staff to promote buy-in. The script also contained a brief explanation as to why bringing medications/medication lists was important. Similarly, the existing written reminder on new patient appointment letters was made more conspicuous and expanded to explain the importance of bringing medications/medication lists to appointments (online supplementary appendix 6). Lastly, the clinics’ ‘Next Steps for Your Care’ forms, which are given after every appointment, were updated with stickers that stated ‘IMPORTANT: Please bring a list of your medications or your actual medications to your next appointment.’ To maintain sustainability, the written reminder was later incorporated into the form’s template as a callout textbox. Multiple reminders were thought to be needed for the OPRA clinic population, because there is a high prevalence of cognitive impairments.
Supplementary file 6
The third driver of the quality problem pertains to patients who find it cognitively difficult to make a medication list, or may not be aware that complete medication lists need to have medication names, frequencies and doses. The medication list template created by Varkey et al 15 was chosen for adaptation by the project team for this project after an environmental scan. This medication list template was provided to the clinic nurse, administrative staff and a convenience sample of three patients for feedback. The adapted medication list template (online supplementary appendix 7) was mailed to all new patients as part of their appointment letter package, and later given to patients who did not bring their medications/lists.
Supplementary file 7
Strategy
PDSA cycle 1 (week 3)
A new script for confirmation phone calls with a reminder about medications/medication lists was implemented. The change hypothesis was that a contiguous reminder close to the patients’ appointments would be more effective. The scripts were posted at administrative assistants’ workstations and announced during the clinic’s daily huddles. Following implementation, there was no change in the percentage of patients who brought their medication lists/medications, which was unexpected. Feedback from the administrative assistants was that the new script was too long.
PDSA cycle 2 (week 4)
New patients typically receive a mailed initial appointment letter. The letter template was altered by the hospital’s information technology department with a more conspicuous reminder to bring medications/medication lists. There was no immediate change in the percentage of patients who brought their medication lists/medications, which was expected since the time between when patients are first contacted to their appointments could be up to 6 months.
PDSA cycle 3 (week 9)
In response to feedback from the administrative assistants during PDSA cycle 1, the script for confirmation phone calls was shortened for efficiency. There was an increase in the percentage of patients who brought their medication lists/medications with these reminders in the next month, which was expected.
PDSA cycle 4 (week 11)
Since patients with brain injuries have difficulty processing complex verbal information, written reminders may be more effective than verbal reminders. The clinic provides patients with ‘Next Steps for Your Care’ forms as they exit from their appointments, which is a one-page sheet that combines an appointment card with patient instructions. The ‘Next Step for Your Care’ forms were updated with a written reminder that patients need to bring their medications/medication lists with them to their next appointment. There were further increases in the percentage of patients who brought their medication lists/medications. However, these changes are more likely related to PDSA cycle 3, and could not be attributable to the updated ‘Next Step for Your Care’ forms, since patients who received those forms would not return for follow-up for 1–6 months.
PDSA cycle 5 (week 18)
With a further focus on written reminders, an adapted medication list template was mailed to all new patients as part of their appointment letter package to help those with cognitive impairments. The previously seen increase in the percentage of patients who brought their medication lists/medications did not represent special cause variation and there was no further immediate increase after the implementation of the medication list template. This was expected, since patients may not come to clinic until 6 months after they receive their appointment letter package with the template.
PDSA cycle 6 (week 21)
The project team attempted to improve the effectiveness of the verbal reminders. Retrospective analysis of a sample of 30 consecutive patients from two physiatrists’ clinics during November 2016 to March 2017 showed that whether patients received a reminder or not did not significantly impact whether they brought their medications/lists. The project team theorised that patients may need further clarification that medication lists should be a written rather than a mental list and updated the script accordingly. There was no immediate change in the percentage of patients who brought their medication lists/medications, which was unexpected.
Results
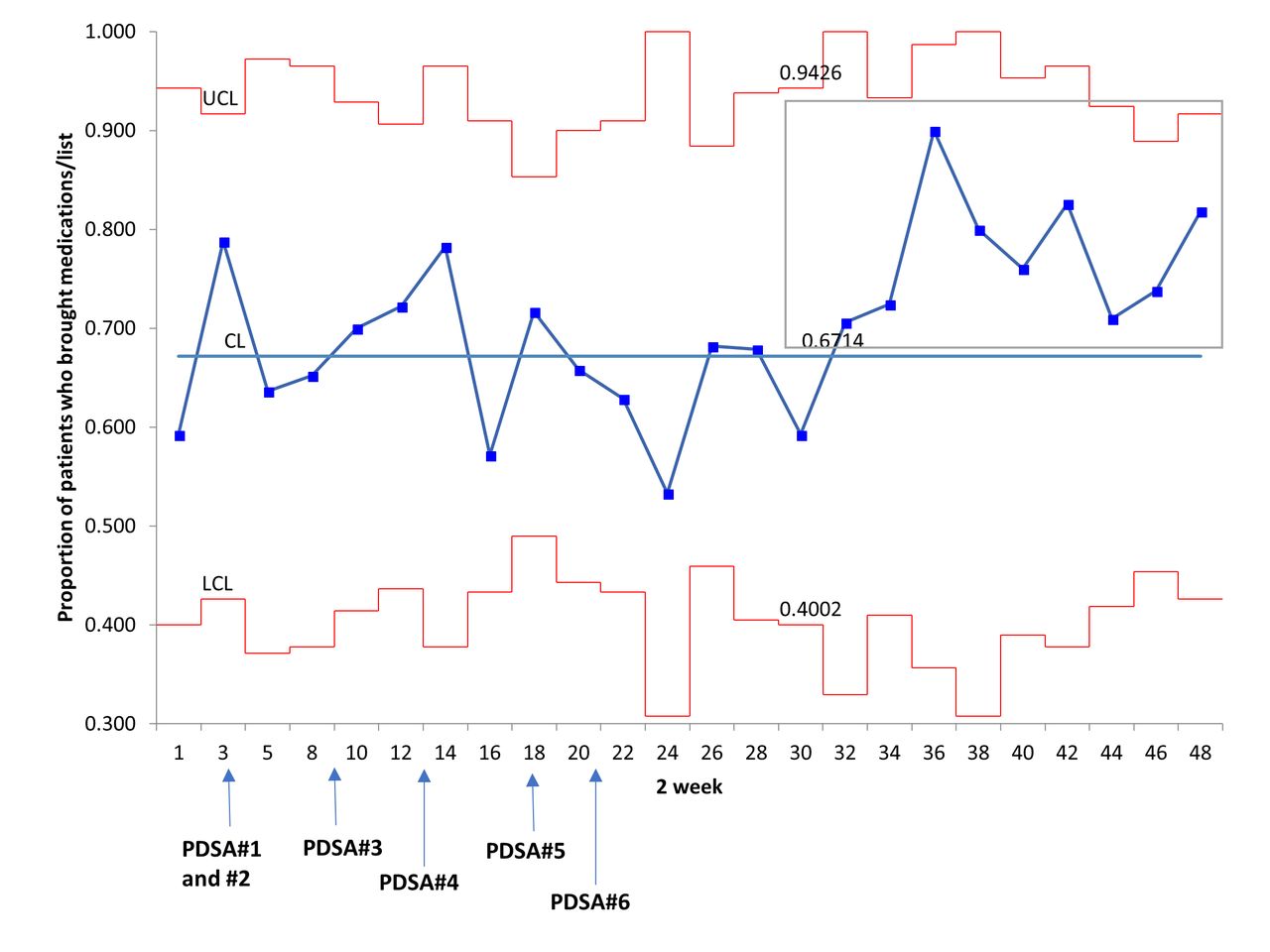
At baseline, a survey of three PM&R specialists’ clinics over 1 week demonstrated 47.8% (11 out of 23) of patients brought their medication lists/medications to appointments despite receiving verbal reminders and in the case of new patients, also written reminders. Over the course of the project, the percentage of patients who brought their medications/lists to the OPRA clinic increased to 81.8% (week 48/49), and the target aim was achieved. As shown in figure 1, special cause variation was detected, and there were 9 points above the centre line from week 32/33 to week 48/49. In comparison, the percentage of patients who brought their medications/lists to the spasticity clinic (figure 2), which had served as the ‘control’ for this project, decreased from 88.9% to 50.0%, but there was no special cause variation observed on the statistical control chart.
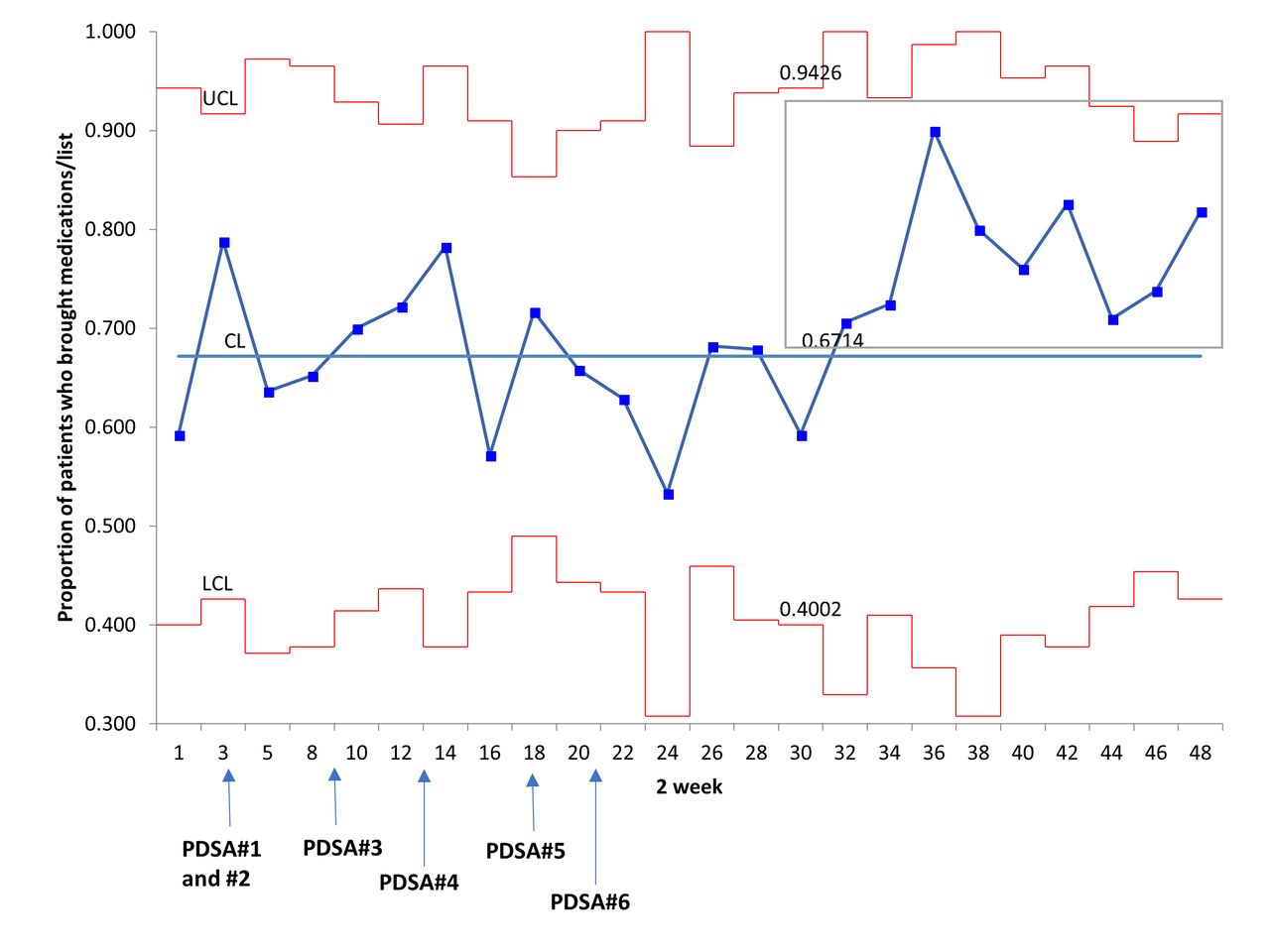
P chart—the proportion of patients who brought their medications/medication lists to the outpatient rehabilitation assessment (OPRA) clinic from 14 November 2016 to 20 October 2017. Each data point represented an average of 29.6 patients per 2-week interval. Special cause variation in the form of 9 points above the centre line was seen from week 32/33 to week 48/49 (grey box). The red lines represent the upper and lower control limits, and the blue line represents the control limit. CL, control limit; LCL, lower control limit; PDSA, Plan-Do-Study-Act; UCL, upper control limit.

P chart—the proportion of patients who brought their medications/medication lists to the spasticity clinic from 14 Nov ember 2016 to 20 October 2017. Each data point represented an average of 12.3 patients per 2-week interval. No special cause variation was seen. The red lines represent the upper and lower control limits, and the blue line represent the control limit. CL, control limit; LCL, lower control limit; UCL, upper control limit.
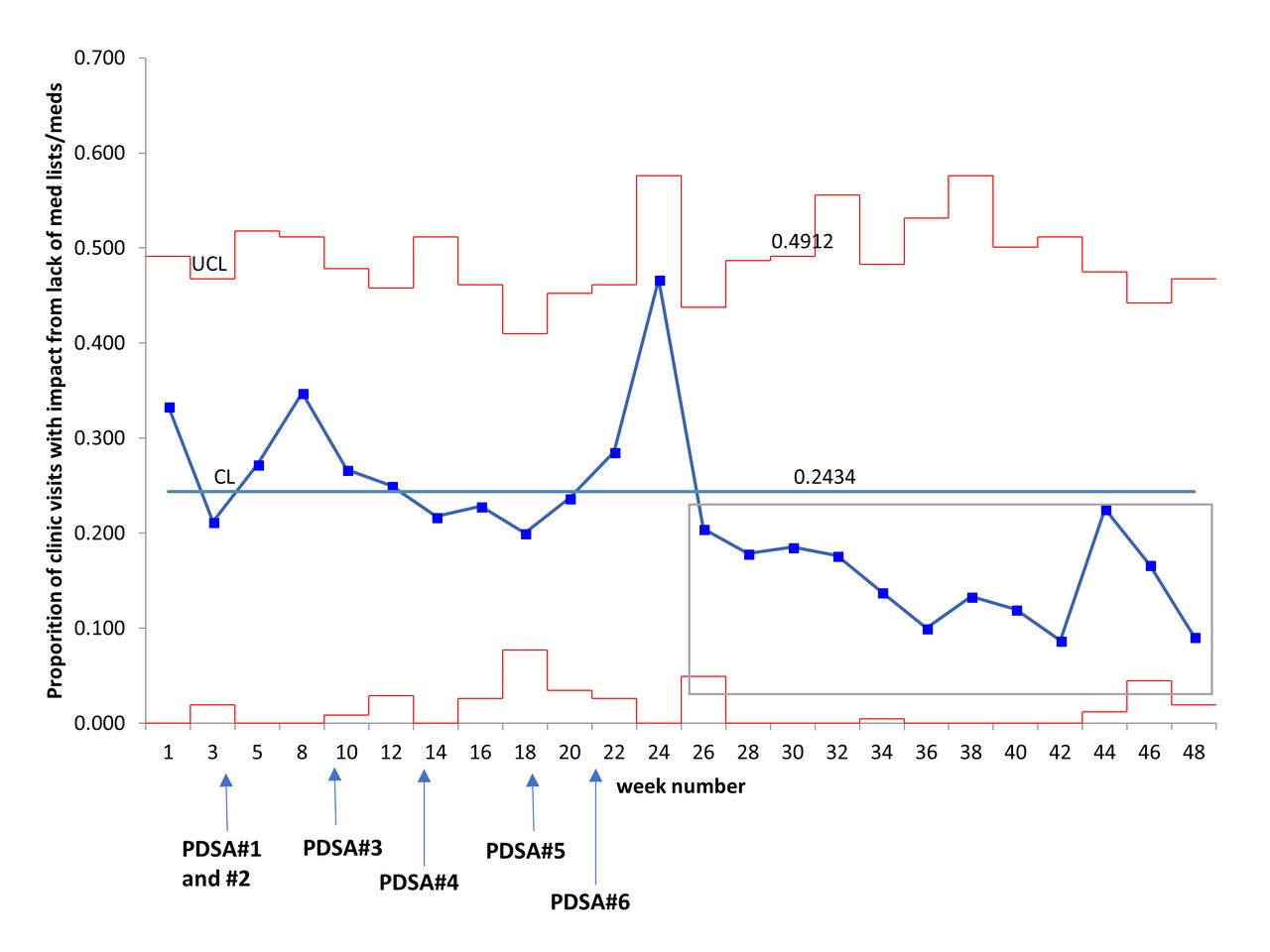
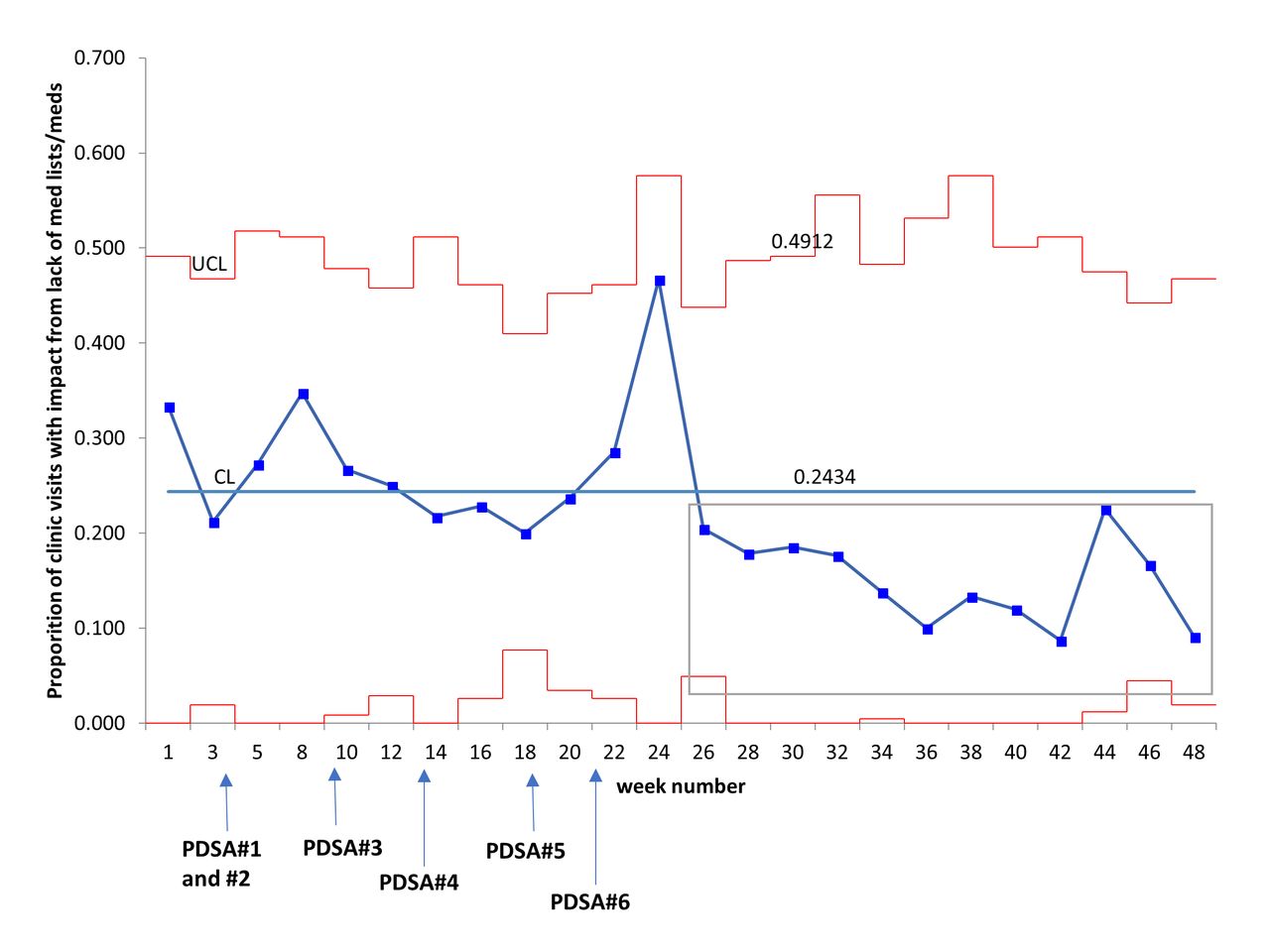
Similarly, the proportion of clinic visits where missing medication information affected clinic flow/staff workload decreased from 33.3% (weeks 1–2) to 9.1% (weeks 48–49), and the target secondary aim was reached. Special cause variation was detected on the control chart (figure 3). There were 12 points below the centre line from week 26/27 to week 48/49. Conversely, the proportion of clinic visits impacted by missing medication information for the spasticity clinic (online supplementary appendix 8) was 11.1% at weeks 1–2 and 50% at weeks 48–49, but the change was not significant on the statistical process control chart. One point above the upper control limit was observed during week 30/31, when 56.5% of clinic visits were impacted by missing medication information.
Supplementary file 8
{kind=link}
{kind=link}
{kind=link}
P chart—the proportion of patients whose clinic visit was impacted by not having brought their medications/medication lists from 14 November 2016 to 20 October 2017 in the outpatient rehabilitation assessment (OPRA) clinic. Each data point represented an average of 29.6 patients per 2-week interval. Special cause variation in the form of 12 points below the centre line was seen from week 32/33 to week 48/49 (grey box). The red lines represent the upper and lower control limits, and the blue line represent the control limit. CL, control limit; PDSA, Plan-Do-Study-Act; UCL, upper control limit.
The verbal reminders (PDSA cycles 1, 3, 6) during confirmation phone calls likely did not contribute significantly to the improvement seen. Confirmation calls are made 2 days prior to the patients’ appointments, and therefore would have an immediate impact on the outcome measures once implemented. Special cause variation (1 point below lower control limit and 2/3 points below 2 sigma) was seen in the percentage of patients who receive a verbal reminder about medications during week 8 and week 9, which corresponded to seasonal holidays for the clinic (online supplementary appendix 9). After the holidays, there was high fidelity for the verbal reminder intervention and most patients received verbal reminders to bring their medications. On average, 89.4%±6.4% of patients between week 10 and week 36 received reminders.
Supplementary file 9
However, despite the high fidelity of implementation, a retrospective analysis performed by cross-referencing the data collection sheets with the administrative assistants call lists for a sample of 30 patients from two physiatrists’ clinic during November 2016 to March 2017 showed that whether patients received a reminder or not did not significantly impact whether they brought their medications/lists (p=0.12). Although verbal reminders via phone calls are recommended by the AHRQ, in hindsight patients with cognitive communication deficits from ABIs in the OPRA clinic would have difficulty processing and remembering multiple pieces of information in phone calls.
Therefore, the improvement observed in this project is more likely attributable to the written reminders implemented in PDSA cycles 2 and 4 that targeted new and follow-up patients. These interventions have significant lag time of 3–6 months, depending on the wait times in the clinic, and the effects from these interventions were therefore not detected until week 30/31. However, the project team could not rule out that the combined effect of written and verbal reminders led to the improvement seen.
Balancing measures for the project focused on the administrative staff’s perception of the project. NASA-TLX results indicate that the confirmation phone call script with the verbal reminder at first presented greater demands on the administrative staff, but by the end of PDSA cycle 6 was less physically and temporally demanding and required less effort than before the project (online supplementary appendix 10). Qualitative feedback from weekly huddles indicated largely positive feedback on the change ideas and there were no reported consequences such as patient frustration with the verbal or written reminders.
Supplementary file 13
There were no data from the spasticity clinic due to staff holidays affecting clinic operations during weeks 39 and 43. Otherwise, there were no missing data for the project.
Lessons and limitations
A key lesson learnt from this project was the importance of prolonged data collection when implementing interventions with long lag time. Although the project was ultimately successful in reaching its aims, due to the written reminder intervention’s long lag time, the project team was concerned about the initial lack of success and had nearly terminated the project prematurely.
Another lesson learnt was the importance of context in QI work. The project team had conducted a literature search and found a plethora of evidence-based interventions for the quality problem. However, the studies by Nassaralla et al 12 13 and Varkey et al 15 did not explicitly involve patients with cognitive impairment. Therefore, when the project team attempted to implement verbal reminders during confirmation phone calls, the intervention unexpectedly did not yield any immediate improvement. If this project was undertaken again, the team would first take steps to innovate solutions that focus on addressing the patient populations’ cognitive impairments.
In terms of limitations, the project included only one process measure to assess for fidelity of implementation. Although there were anecdotal reports of new patients bringing completed medication list templates that had been mailed, measuring the number of completed medication list templates received per week as an additional process measure would have been valuable to ascertain the effectiveness of the templates. In addition, there were predefined standardised criteria for the impact of patients not bringing medications/medication lists, but the data were collected by four different project team members without measures of inter-rater reliability.
The start-up costs for the project are estimated at $C917.02 (online supplementary appendix 11).
Supplementary file 11
Conclusion
Patient involvement in medication reconciliation is crucial, as clinicians must verify the reported medication history with other sources such as home medication lists or brown-bagged home medications provided by patients. Prior to this QI project, 47.8% of brain injury and stroke adult outpatients at Toronto Rehab, an academic rehabilitation hospital, did not bring medications/medication lists to clinic visits. This project aimed to increase the percentage of patients who bring their medication lists/medications to their appointments at UHN-TRI, UC to 80% or more, thereby decreasing the impact of missing medication information on clinic processes to less than 10% of clinic visits. After six PDSA cycles over 49 weeks, the project has successfully achieved both of its aims. The changes implemented are highly sustainable since the changes did not result in significant increases in staff workload, and the written reminders have been automated into the clinic’s information packages and ‘Next Steps for Your Care’ forms.
Lessons learnt include the importance of prolonged data collection when implementing interventions with long lag time, and the importance of context in QI. Future efforts will focus on implementing the bundle of project interventions for the spasticity clinic.
References
Footnotes
Contributors MG, CS, BF, MB and AL conceived the project idea. MG, AT, AD, MP, BF and MB performed the diagnostic analysis of the quality problem, and designed the change ideas and the PDSAs. MG, AT, AD, MP and AL collected the data for this QI project. MG, AT, CS and AD performed the data analysis and interpretation. MG drafted the paper, and AT, AD, MB, CS, BF, MP and AL critically revised the paper. All authors gave final approval of the version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval This project received a formal letter of exemption from the Research Ethics Board (REB) at University Health Network. The REB deemed the nature of the project as quality assurance/quality improvement, as defined in Article 2.5 of the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans, 2nd Edition.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.