Article Text

Abstract
Background Delirium is a common manifestation in the intensive care unit (ICU) that is associated with increased mortality and morbidity. Guidelines suggested appropriate management of pain, agitation and delirium (PAD) is crucial in improving patient outcomes. However, the practice of PAD assessment and management in community hospitals is unclear and the mechanisms contributing to the potential care gap are unknown.
Objectives This quality improvement initiative aimed to review the practice of PAD assessment and management in a community medical-surgical ICU (MSICU) and to explore the community MSICU nurses’ perceived comfort and satisfaction with PAD management in order to understand the mechanisms of the observed care gap and to inform subsequent quality improvement interventions.
Methods We prospectively collected basic demographic data, clinical information and daily data on PAD process measures including PAD assessment and target Richmond Agitation-Sedation Scale (RASS) score ordered by intensivists on all patients admitted to a community MSICU for >24 hours over a 20-week period. All ICU nurses in the same community MSICU were invited to participate in an anonymous survey.
Results We collected data on a total of 1101 patient-days (PD). 653 PD (59%), 861 PD (78%) and 439 PD (39%) had PAD assessment performed, respectively. Target RASS was ordered by the intensivists on 515 PD (47%). Our nurse survey revealed that 88%, 85% and 41% of nurses were comfortable with PAD assessment, respectively.
Conclusions Delirium assessment was not routinely performed. This is partly explained by the discomfort nurses felt towards conducting delirium assessment. Our results suggested that improvement in nurse comfort with delirium assessment and management is needed in the community MSICU setting.
- attitudes
- critical care
- nurses
- performance measures
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Delirium, or acute brain dysfunction, is a disturbance of consciousness characterised by an acute change or fluctuating course of mental status, inattention and the inability to receive, process, store or recall information.1 More than 80% of patients develop delirium during their intensive care unit (ICU) stay.2 This incidence rate can be influenced by factors such as the level of consciousness, the residual sedative effects and diagnosis such as depression and post-traumatic stress disorder in ICU patients.3 Moreover, a low Richmond Agitation-Sedation Scale (RASS) value increases the likelihood of a positive delirium screen, and among patients whose RASS scores change more than two levels from the previous day, the presence of delirium detected with the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) could be five times more likely.3 4 More importantly, delirium is associated with increased mortality both in hospital and after discharge, prolonged hospital length of stay and long-term cognitive dysfunction.2 5–7 This is especially concerning in ICU settings, where mechanically ventilated patients are at high risk for the development of delirium due to multisystem acute illness, comorbidities, medications and other risk factors.1 8–13
In 2013, the Society of Critical Care Medicine revised its ICU pain, agitation and delirium (PAD) guidelines with emphasis on targeting lighter sedation goals. The implementation of these guidelines has demonstrated improvements to both short-term and long-term ICU outcomes and reduction in costs of care.14 Chanques et al demonstrated that a systematic evaluation of pain and agitation by nurse followed by a medical intervention in an ICU was associated with a decrease in the incidence of pain and agitation.15
However, adherence remains inadequate, with deep sedation being a common place in the ICU.14 16 17 Luetz et al investigated the implementation rate of delirium monitoring among intensivists from various hospitals through anonymous surveys and questionnaires.18 Their data revealed a perceived implementation rate of delirium assessment with a validated tool of 44%, but only 27% of patients were truly asessed.18 Literature revealed routine delirium monitoring was performed more often in university hospitals than in small teaching or regional public hospitals with 54% of the university hospitals using validated delirium scales compared with 29% in non-academic hospitals.18 19
Nursing staff play a crucial role in monitoring PAD in the ICU. Educational interventions have been shown to address barriers to guideline implementation and are crucial for ensuring sustained improvements within the healthcare environment.20 21 Barnes-Daly et al have evaluated an educational intervention in a community setting.22 However, their study also involved the ABCDEF bundle, and thus the independent contributions of a nurse educational intervention have yet to be explored. Walsh et al have assessed the effectiveness of three interventions to improve sedation and analgesia quality and sedation-related adverse events daily in a cluster randomised trial in eight Scottish ICUs over an 8-week period. The interventions were online education programme, sedation-analgesia quality feedback and the use of a novel sedation-monitoring technology (the Responsiveness Index (RI)). The authors found that the education intervention did not improve sedation-analgesia quality but it was associated with an almost 50% relative reduction in sedation-related adverse event rates. The education intervention was universally valued, comprehensive and found as a useful resource by staff. Its effect seemed greatest on the awareness and management of agitation and delirium and it was perceived to improve knowledge that was retained over time and to increase nursing autonomy. They found a significant improvement in optimal sedation-analgesia with RI monitoring. However, RI monitoring seemed to increase the number of patients experiencing sedation-related adverse events. Lastly, the sedation-analgesia quality feedback did not improve quality or sedation-related adverse events. The authors concluded that the combination of an RI monitoring and an online education programme could be extremely beneficial in improving sedation-analgesia quality and patient safety in mechanically ventilated ICU patients.23
In response to the barriers mentioned, the purpose of this study is to review current PAD assessment and management practice in a community medical-surgical ICU (MSICU), examine nurses’ perceived comfort and satisfaction surrounding PAD management in a community MSICU, and consequently inform future educational interventions in order to overcome current barriers to PAD management. An emphasis will be placed on delirium, as it seems to contain the widest knowledge gaps, and results in costly adverse effects on patients and the hospitals.2 5 6 Nurses were chosen as the initial focus because they are at the frontline in assessing and treating PAD, positioning them to play a key role in PAD quality improvement initiatives.21 24
Methods
We followed the Strengthening the Reporting of Observational Studies in Epidemiology statement during the reporting of this study.25
Study design
We conducted (1) a prospective single-centre observational study to review the practice of PAD assessment and management in a community MSICU and (2) a single-centre nurse survey to examine community MSICU nurses’ perceived comfort surrounding PAD assessment and management, and satisfaction with PAD management by other nurses and physicians.
Setting and participants
The studies were conducted in a community MSICU with 14 level III beds and a nurse-to-patient ratio of 1:1 or 1:2. There is a dedicated ICU pharmacist, respiratory therapist, physiotherapist, dietitian and 24-hour in-house intensivist coverage. The healthcare team provides care to general medical, cardiac, respiratory, nephrology, oncology, general surgical, orthopaedic and vascular surgical patients. In this MSICU, a policy is in place to stipulate that pain is assessed using Numeric Pain Rating Scale (NPRS) at the beginning of each shift, after analgesic administration every 4 hours and as needed. Sedation level is assessed using RASS at the beginning of each shift and as needed and delirium is assessed using CAM-ICU.
The studies were approved by the local research ethics board. The observational study was conducted over a 20-week period from April to August 2016. All patients admitted to the ICU for greater than 24 hours were recruited in the observational study. The nurse survey was conducted in August 2016. All ICU nurses were invited to participate through email and in-person invitations during their work shifts.
Data collection and analysis
Observational study
A team of dedicated data collectors prospectively collected patient data by reviewing patients’ medical charts (electronic and paper) daily. Basic demographic and clinical information in addition to specific process and outcome measures surrounding PAD management were collected, recorded and anonymised in an Excel spreadsheet.
Process measures included pain assessment using NPRS, agitation assessment using RASS, target RASS score ordered by intensivists and delirium assessment using CAM-ICU. For the purpose of this study, we specifically evaluated PAD assessment at least once per day. The total patient-days (PD) with the above process measures were represented.
Nurse survey
All ICU nurses were recruited to participate in the nurse survey (developed by the PAD study team, see online supplementary appendix 1) by email and in-person in the ICU. The survey was administered in three different forms to improve response rate: paper survey, fillable PDF form and online survey. Most nurses completed the paper survey during their shift and placed them anonymously in an envelope into a designated box in the ICU. Using 5-point Likert scale, the survey explored nurses’ perceived comfort surrounding PAD management, and satisfaction with PAD management by other nurses and physicians. Proportions were used to represent the survey results.
Supplemental material
Results
Delirium assessment is the most significant care gap
As part of a PAD quality improvement programme, a prospective observational study was conducted to review the baseline PAD assessment and management practice. There was a care gap in PAD assessment, with delirium assessment being the biggest care gap. Out of a total of 1101 PD, pain assessment using NPRS, agitation assessment using RASS and delirium assessment using CAM-ICU were conducted on 653 PD (59%), 861 PD (78%) and 431 PD (39%), respectively (table 1). Out of 448 PD without pain assessment, 62 PD (14%) had RASS ≤3 and 261 PD (58%) were ventilated. Out of 670 PD without delirium assessment, 75 PD (11%) had RASS ≤3 (table 1). Target RASS was ordered by the intensivist on 515 PD (47%) (table 1).
Pain, agitation and delirium performance measures
Nurses are least comfortable with delirium management
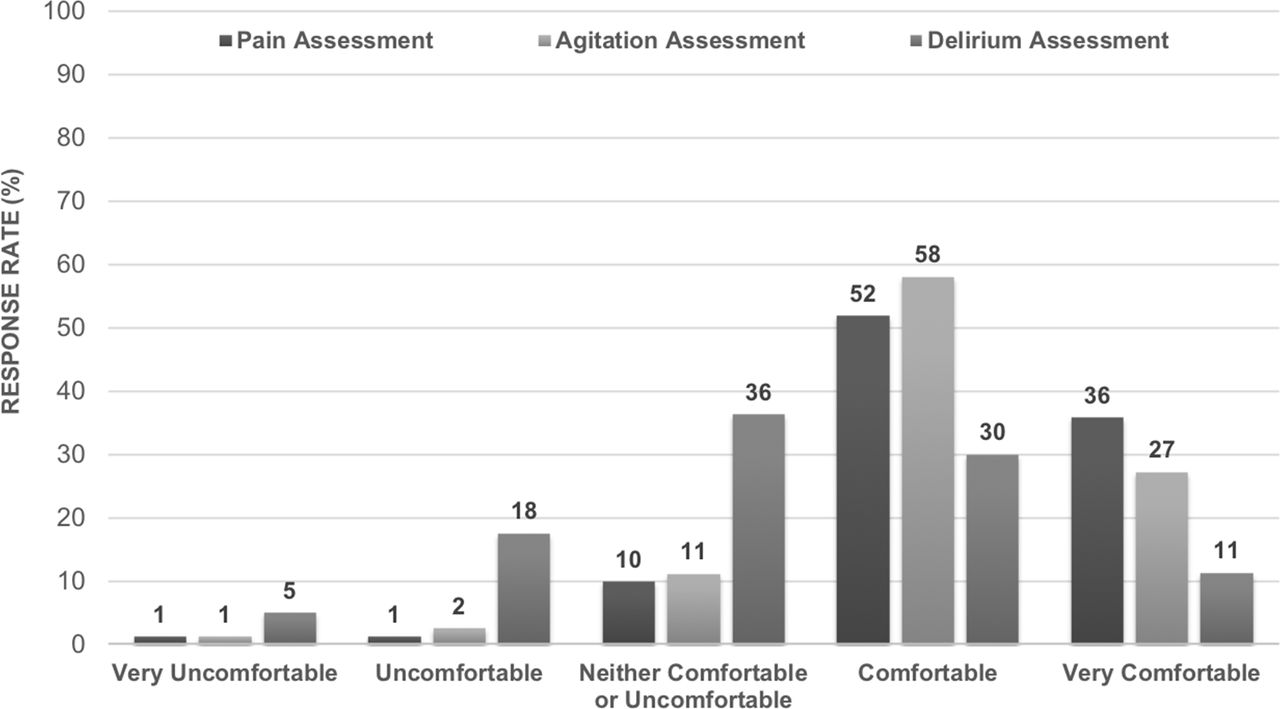
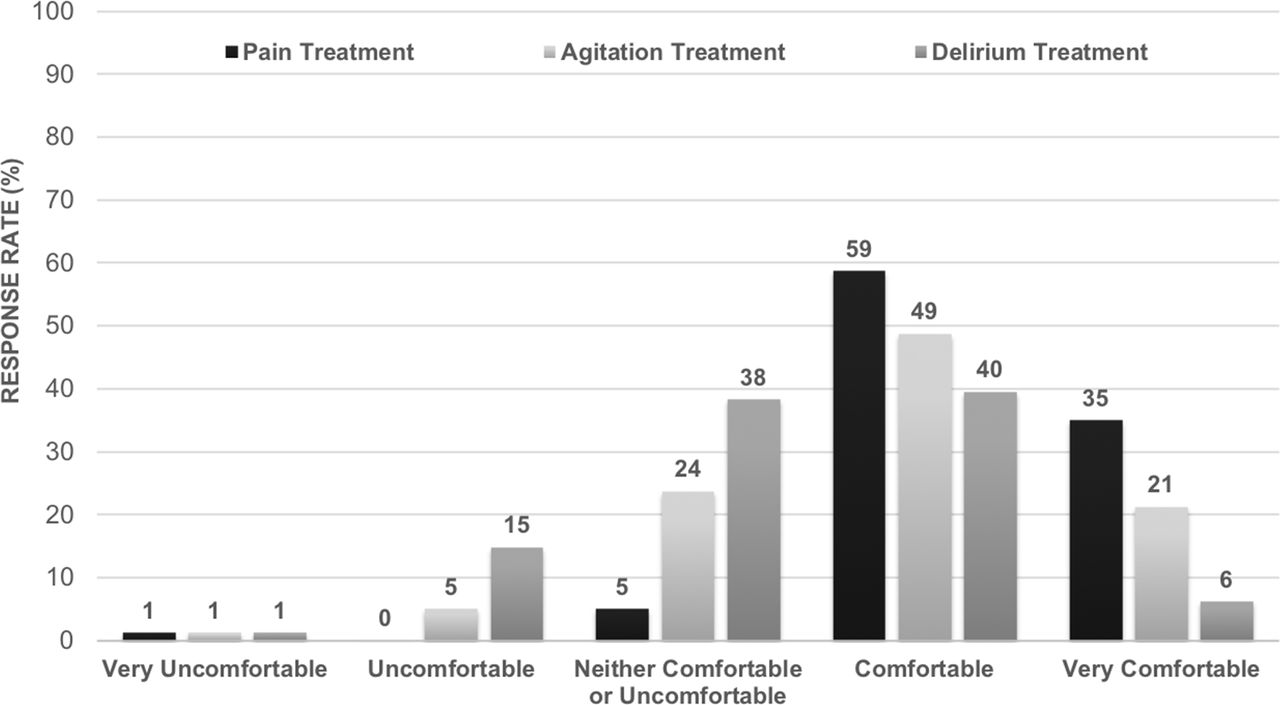
In order to design effective quality improvement interventions for PAD management, a nurse survey was conducted to explore nurses’ perceived comfort and satisfaction with PAD management. The response rate was 98% (81 responses) with nurses reporting a median of 6 years of ICU nursing experience. The results of the survey demonstrated that the nurses were least comfortable with delirium assessment. A total of 88%, 85% and 41% of nurses were either comfortable or very comfortable with the assessment of PAD, respectively (figure 1). We observed a similar trend with delirium treatment. A total of 94%, 70% and 46% of nurses were either comfortable or very comfortable with the treatment of PAD, respectively (figure 2).

Survey response rate of nurses’ perceived comfort levels surrounding pain, agitation and delirium assessment.
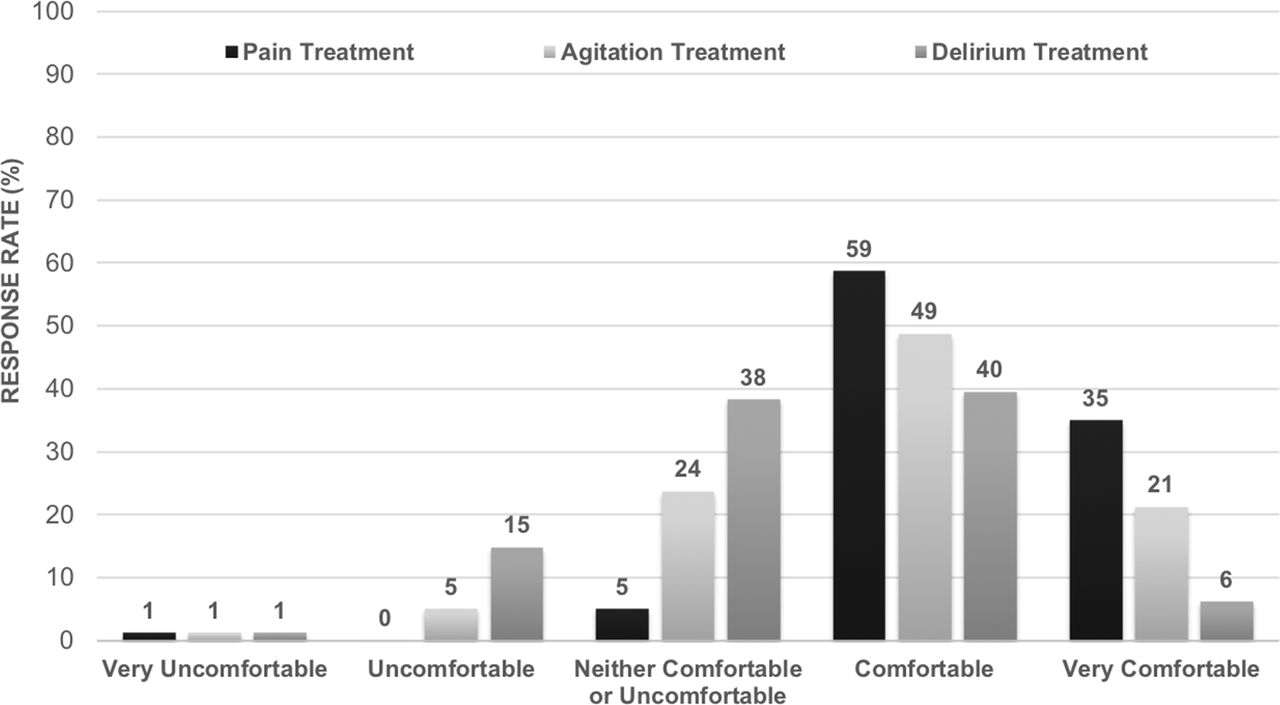
Survey response rate of nurses’ perceived comfort levels surrounding pain, agitation and delirium treatment.
Nurses are not satisfied with PAD management
The survey also explored whether the community MSICU nurses felt that there was a care gap in PAD management. Our survey demonstrated that nurses were not satisfied with PAD management provided by other nurses (only 47% of nurses were satisfied or strongly satisfied with PAD management provided by other nurses) (figure 3). The nurses’ satisfaction towards intensivists’ PAD management was similar (only 42% of nurses were satisfied or strongly satisfied with PAD management provided by intensivists) (figure 3). These results suggest that ICU nurses felt that there was a care gap in PAD management.

{kind=link}
{kind=link}
{kind=link}
Survey response rate of nurses’ satisfaction surrounding pain, agitation and delirium management provided by other nurses and intensivists.
Discussion
This prospective observational study and nurse survey study were conducted to examine the potential care gap in PAD assessment and management in a community MSICU and to obtain buy-in from the frontline nurses for subsequent PAD quality improvement initiatives. Despite having a policy in place to stipulate the assessment of PAD regularly, there were care gaps in PAD assessment with delirium assessment representing the most significant care gap. It is noteworthy that the observed suboptimal delirium assessment rate represents a care gap rather than an inability to screen as only 11% of the patients without delirium assessment were oversedated (RASS ≤3). However, the observed suboptimal pain assessment rates may represent an inability to screen rather than a care gap because at the time of the observational study, this community MSICU was using NPRS rather than a behavioural pain scale to assess for pain. This precluded pain assessment in patients who were oversedated with RASS ≤3 (14% of PD without pain assessment) or ventilated (58% of PD without pain assessment).
Most importantly, the nurse survey also demonstrated that the nurses felt the most uncomfortable with delirium assessment and management. This suggested that the nurses’ discomfort in delirium assessment contributed to the observed care gap in delirium assessment. These results suggest the need for education interventions to improve the competency of nurses with delirium management.
Devlin et al showed that only 3% of ICU nurses ranked delirium as the most important condition to evaluate, compared with level of consciousness (44%), presence of pain (23%) or improper placement of an invasive device (21%).26 Moreover, ICU nurses reported many barriers to delirium assessment including intubation (38%), the complexity of tools for assessing delirium (34%) and the inability to complete assessments of delirium in sedated patients (13%).26 These factors potentially contribute to the low rate of delirium assessment shown in this observational study. Furthermore, they suggest the need for nurse-focused educational interventions to help nurses overcome these misconceptions about delirium and perceived barriers to delirium assessment and to close the care gap.
Walsh et al focused their educational intervention on the management of PAD and the process evaluation demonstrates that these components were most positively perceived and they improved staff knowledge.23 Moreover, Carrothers et al showed that factors such as an ICU culture of quality improvement, access to training materials and access to hands-on support from nurse champions resulted in faster implementation of delirium screening process. In contrast, excessive turnover and knowledge deficits are related to delayed implementation of the PAD guidelines.27
The nurse survey also revealed that only half of the ICU nurses were overall satisfied with how PAD were managed in the ICU by other nurses or intensivists but were confident in their own care practices related to pain management. This suggests that a multidisciplinary quality improvement initiative could be crucial in closing the care gap to ensure a more consistent approach to PAD in the ICU. That said, this high rating of self-confidence in individual practice may be impacted by social acceptability bias given the self-reported nature of the nurse survey. Research has shown that interdisciplinary collaboration is essential to the successful implementation of individualised care. It is critical to promote an inclusive culture in which there is buy-in from bedside nurses, allied health professionals and physicians, and a ‘no-blame’ attitude, as they are the core of the Early Comfort Using Analgesia, Minimal Sedatives and Maximum Humane Care framework.17 This can be achieved through adequate staff education on sedation-analgesia management.28 29 Finally, the focus must be on multimodal interventions, which include but are not limited to, implementation planning, training/support, effective documentation and debriefing when possible, while being mindful that staff turnover, poor staff morale and lack of interdisciplinary respect are barriers to patient-centred care.27
The strengths of this study include the combination of prospective observational cohorts with over 1000 PD and a nurse survey with greater than 98% response rate to explore the mechanisms contributing to the observed care pattern. The limitations of this study include the reliance on nursing charting practice to reflect actual clinical practice and the lack of formal validation of the nurse survey.
In summary, this prospective observational study identified a PAD management care gap, specifically in delirium assessment. This was explained by the results of the nurse survey that demonstrated the discomfort nurses felt towards delirium assessment and management. The results from these studies, along with the literature, will inform subsequent targeted quality improvement interventions to close the care gap and therefore improve patient outcomes in the community MSICU.
Acknowledgments
We acknowledge all the nurses who participated in the nurse survey.
References
Footnotes
FM is the first author.
33 JLYT is the senior author.
Contributors RM performed data analysis and prepared the manuscript. KR planned the study, developed the survey and performed data analysis. FM, PY, CM, CT and MC performed data analysis. DF and ML planned the study. JLYT planned the study, developed the survey, developed data collection form and prepared the manuscript.
Funding This work was supported by the Ontario Nurses’ Association and the McMaster University, Department of Medicine, EJ Moran Campbell Internal Research Career Award 2015–2018 (JLYT).
Competing interests None declared.
Ethics approval Hamilton Integrated Research Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.