Article Text

Abstract
To address the gap in the uptake of long-acting contraception (LAC) methods among high-risk postpartum women who fail to return for a family planning method at HôpitalUniversitaire de Mirebalais in the Central Plateau Department of Haiti, contraceptive implant trainings were held for providers on the Labour and Delivery, Post-Partum and Internal Medicine inpatient wards.
A very high maternal mortality rate affects large numbers of women in Haiti; however, contraceptive use can reduce maternal mortality significantly. A quality improvement strategy to offer LAC methods to immediate postpartum women at a University Hospital in rural Haiti was initiated in March 2016. This new strategy produced an average improvement from 5% to 32% of women delivering at the hospital, accepting a long-acting method (including bilateral tubal ligations) by the end of the project and which has proved sustainable at an average of 20% to date.
- quality improvement
- obstetrics and gynecology
- women’s health
- nurses
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Problem
Women in Haiti have a very high maternal mortality rate at 359 per 100 000 live births,1 compared with the USA at 14 and Cuba at 39.1 According to a recent study, maternal deaths can be reduced by up to 44% with contraceptive use and when all contraceptive needs are met can reduce maternal mortality by up to 60%.2 Globally, the prevalence of modern contraceptive use increased from 47.8% in 1990 to 58% in 2010.3 In Haiti, uptake lags significantly at 31%.4 Worldwide, one quarter of married or cohabitating women who use a contraceptive method choose a long-acting reversible contraceptive (LARC) method.5
Rationale
The Hôpital Universitaire de Mirebalais (HUM), located in the Central Plateau Department of Haiti, is a 300-bed rural tertiary referral, University teaching hospital that serves a population of approximately 185 000 in its primary catchment area.6 Newly opened in 2013, an average of 375 women per month deliver in the Maternity services, the majority of whom are high-risk women, with severe pre-eclampsia or eclampsia accounting for an average of 16% of the admissions into the services. It is important to note that the primary cause of maternal mortality in Haiti is eclampsia, at 42%.7 8 Outpatient Women’s Health services provides family planning services to a monthly average of almost 500 women7; however, the uptake of long-acting contraception (LAC) averaged only three per month in the 12 months preceding the interventions.
The total fertility rate in Haiti is 3.5 children per woman (figure 1), and in the Central Plateau the rate is significantly higher at 4.8 children per woman.4 The desired fertility rate is 2.2 for all of Haiti and 2.6 for the Central Plateau.4 The gap between actual and desired fertility highlights the lack of access to modern contraceptive methods, particularly LAC, which is more effective at preventing pregnancy than short-term methods.9 10 In our context, long distance impacts women’s ability to return for family planning follow-up visits, which consequently negatively impacts the effectiveness of short-acting methods.

Fertility rate: Haiti. The actual fertility rate in the Central Plateau Department of Haiti where the quality improvement project took place is almost five children per woman; the desired number is closer to 3.4
With the potential for reducing maternal deaths by 44% to 60%2 with contraceptive use, the strategy adopted has the potential to have a significant impact and provide rationale for a larger, nationwide adoption. Anecdotally, it was observed by staff members that the same women were coming back year after year to deliver their babies at the hospital. We could not quantify these numbers, but it highlights the gap in unmet family planning (FP) needs, which has been estimated at 35% by the Haitian Ministry of Health (MSPP).4
Severe pre-eclampsia or eclampsia is diagnosed on admission in 15% to 20% of women delivering at HUM.11 Up to nine women per month are re-admitted to Internal Medicine (IM) ward for peripartum cardiomyopathy (PPCM), a risk factor for which is pre-eclampsia. The rate of PPCM in Haiti is 1 per 300 live births compared with 1 per 3000 in the USA and is associated with a high morbidity and mortality in subsequent pregnancies.12 For these reasons, the nursing and residents in IM services were also incorporated in this quality improvement (QI) initiative.
QI projects initiated at HUM do not require institutional review board approval to be carried out and are therefore exempt from an ethics board approval. However, care is taken to protect the rights and welfare of the patients involved and to ensure quality of care addressed in each project approved by the internal QI hospital committee for indicators identified by services throughout the hospital. Because we understand FP is a controversial topic, the project was discussed within the OB/GYN service and then presented for approval to the QI hospital committee.
Our objective was to increase accessibility to LAC methods to women following delivery in an effort to reduce high rates of unintended pregnancies, short-acting method failures, clandestine abortions, women suffering from very high-risk pregnancies and obstetrical complications and ultimately the numbers of women dying in pregnancy, labour, delivery and post partum. The hospital administrators were very supportive financially and logistically of our efforts to expand women’s access to LARC methods.
Regarding contraception, the MSPP states that the repositioning of family planning constitutes one of the strategies adopted by the Department of Family Health (DSF) to achieve the MSPP objective, which is to reduce maternal mortality. This choice is justified by the fact that women who have a higher number of births present a higher risk of dying and also because, through its function of limitation and spacing of the number of births, family planning contributes to the reduction of maternal and child mortality. As part of this strategy, emphasis has been placed on improving access to family planning services.13
Specific aims
The main objective of this QI project was to expand contraceptive access to hospitalised women of childbearing age who had high risk factors for increased morbidities and mortality. This included educational messages, counselling and provision of a LAC method, if desired, prior to hospital discharge to reduce the risk of future obstetrical and life-threatening emergencies and ultimately impact maternal mortality.
Background and available knowledge
Literature on the contraceptive implant is limited to safety, efficacy, clinical trials, drug interactions, use in specific populations (such as adolescents), clinical profile/side effects, effects on breastfeeding mothers in the postpartum period and educational strategies. There were no publications found specifically looking at QI strategies. Additionally, there were no studies found on the use of contraceptive implants in Haiti. A systematic review was found that looked at the use of contraception among young women in developing countries. This particular study revealed the limits of contraceptive use: lack of access, limitations of knowledge on options and importance of countering negative perceptions of modern methods.14 These are similar challenges faced in our context in Haiti: accessibility issues, limited knowledge regarding different methods and method misperceptions.
A study that looked at the number of unintended pregnancies in sub-Saharan Africa examined the impact of expanding the use of contraceptive implants at the expense of short-term hormonal birth control methods.15 Of the 14 million unintended pregnancies that exist every year in sub-Saharan Africa, 28% occur among users of short-acting hormonal FP users. It was estimated that if 20% of the users of short-term contraception switched to long-acting progesterone implants, it could impact 1.8 million unintended pregnancies every year. This can be applied to Haitian women as well; however, the goal of this project was not to try to influence current family planning users but rather to offer the implant to hospitalised women immediately post partum (or post-abortion) with the hopes of reducing future morbidity and mortality via both reduction of unintended pregnancies and high-risk obstetrical emergencies.
Methods
Context
At the start of this project, it was clear that women were not educated about nor accessing LAC FP contraceptive methods, which include bilateral tubal ligations (BTLs), contraceptive implants and intrauterine devices (IUDs). Although IUDs and BTLs were not part of this particular project, in Haiti, they are considered part of LAC methods and are measured together.
In late 2015, WHO changed its Medical Eligibility Criteria (MEC) for the contraceptive implant from Category 3 (risks outweigh the benefits) to Category 2 (benefits outweigh the risks) for immediate postpartum and breastfeeding women.16 This change was the impetus for the onset of the project, which was initiated in March 2016.
Baseline measurement
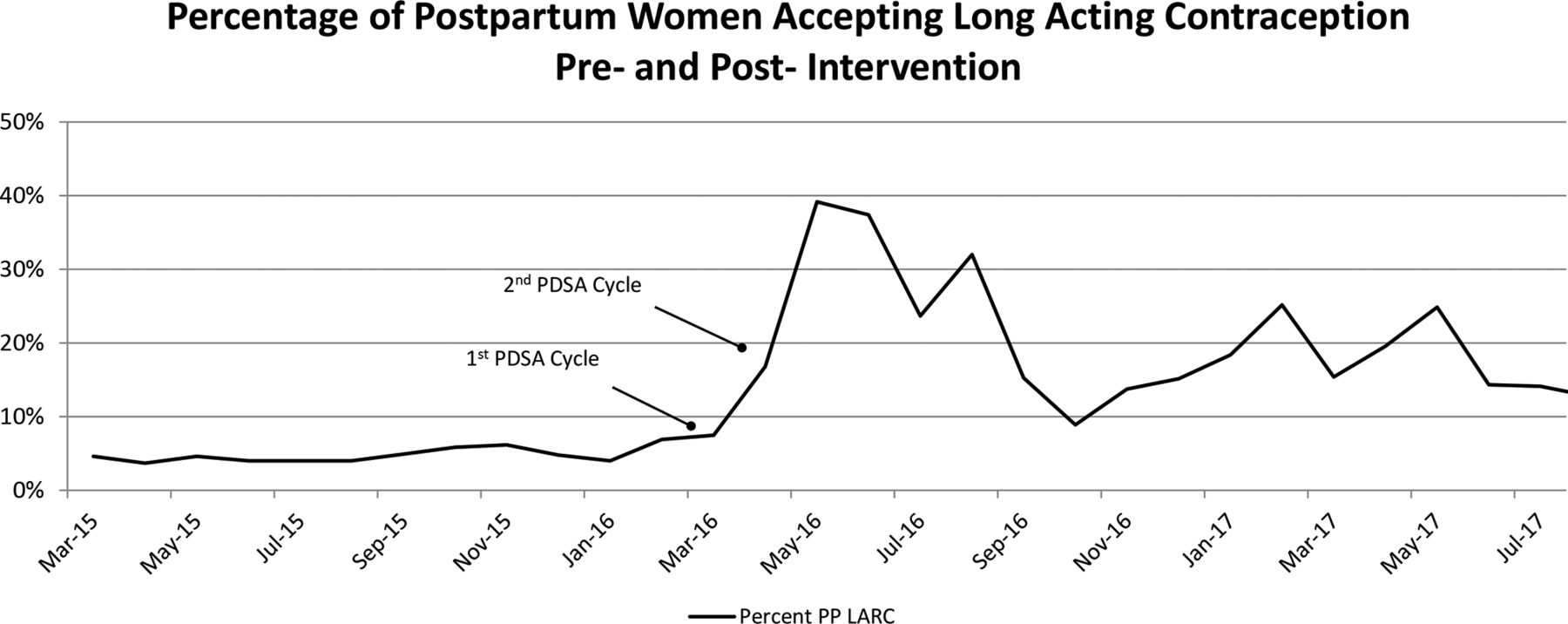
Data that were routinely collected on a monthly basis for the Maternity services were used for the purpose of this project to facilitate baseline and ease of continuous data collection. The acceptance of LAC methods in the data gathered over the 12 months preceding the initiation of the project (March 2015 to March 2016) showed an average of zero implants per month for inpatient services with no other FP options for immediate postpartum women aside from BTLs, which are only offered to women undergoing caesarean sections (figure 2). As a percentage of the deliveries on the services pre-intervention (March 2015 to March 2016), we saw a baseline average of 5% of hospitalised women who delivered at the hospital or who were admitted on IM with PPCM, accepted and were discharged home with a LAC in place (figure 3).
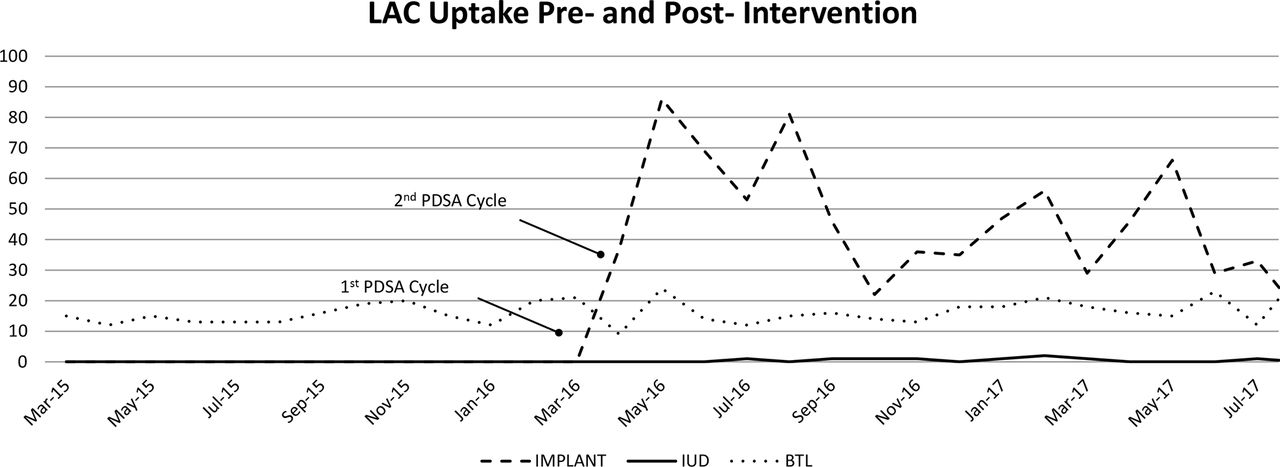
Long-acting contraception (LAC) uptake: pre-intervention and post-intervention. The quality improvement project started in March 2016, with an immediate and long-lasting improvement noted among postpartum women choosing the contraceptive implant. BTL, bilateral tubal ligation; IUD, intrauterine device.

{kind=link}
{kind=link}
{kind=link}
An average of 20% of postpartum women chose long acting contraception post-intervention between April 2016 and July 2017, compared to 5% pre-intervention, March 2015 through March 2016.
Design
This is a report from the field of the use of continuous quality improvement (CQI) method to address the barriers to the adoption of LAC at a teaching hospital in rural Haiti.
Following an internal evaluation and analysis of our monthly data, it was determined that the family planning services at HUM were not actively educating nor making LAC accessible to hospitalised women. This observation led the OB/GYN service to address this concern through the establishment of annual indicators, which were approved through the hospital QI committee.
An internal QI team on the maternity service, composed of a nurse midwife, an OB/GYN resident, the Women’s Health Coordinator, a nurse and the Chief of OB/GYN services, was formed. The CQI tools including flowchart, and Ishikawa and Pareto diagrams were used to conduct the root cause analysis (RCA) and to support decision-making. Our team first performed the RCA in order to better understand the problem and to determine where to intervene and how. It was then decided to address the top reasons for which postpartum women were not accessing LAC family planning methods at the facility.
The Ishikawa tool of cause and effect assisted us in outlining the major causes contributing to the problem of lack of uptake of the LAC methods. These causes were grouped into ‘People, Equipment, Procedures and Environment’. An analysis of each cause was established then quantified and further analysed in the Pareto diagram. The major causes were, for the most part, due to barriers to accessing LAC family planning methods, which negatively impacted FP uptake. It was discovered that the maternity staff on postpartum and labour and delivery (L&D) wards were not motivated nor trained on FP methods and did not educate or encourage women who had delivered in the service to seek a contraceptive method prior to discharge. No protocol for dispensing methods to hospitalised women who desired contraception existed; there were no materials available on the postpartum and L&D wards; in addition, there was no access to FP in the evenings or on weekends. Lack of protocol, materials and poor organisation between inpatient and outpatient services (lack of referrals) were also noted. All of these missing or weak links amounted to postpartum and hospitalised women having a very limited access to contraception.
The initial flowchart that was first analysed showed all women being referred to the outpatient family planning services for all contraceptive education as well as the dispensing and follow-up for the chosen method which highlighted the lack of access to contraception. The improved flowchart essentially demonstrates the decentralisation and improvement of access to FP services, specifically the contraceptive implant that can easily be made available on inpatient wards of the hospital. Short-acting methods are not mentioned specifically, but they were also made available; interestingly, no change in uptake of these methods has been noted.
The interventions put in place included protocols for the services, trainings for the staff and placement of the FP methods on the inpatient wards. We also had to include data collection tools in the form of registers and motivate the Family Planning nurse to collect these new data sources for our monthly reports.
Numerator
The number of hospitalised postpartum women or women admitted in internal medicine with cardiomyopathy, of childbearing age, who had received educational messages and accepted a long-acting FP method.
Denominator
The total number of hospitalised postpartum women or women admitted in internal medicine with cardiomyopathy, of childbearing age, who had received educational messages on long-acting FP methods.
Intervention
Continuous QI using Plan Do Study Act (PDSA) cycles.
Strategy
We conducted two PDSA cycles to evaluate processes and incorporate clinical feedback during this QI initiative.
PDSA cycle 1
The first PDSA cycle in March–April 2016 focused on simultaneously training clinicians, implementing protocols and assuring availability of materials in the services. The rationale being that access to materials and protocols immediately following a training is necessary in order to put in place a new patient care strategy and observe an improvement. For this reason, we had multiple strategies in the first PDSA cycle that were implemented together. Primary areas for improvement included
Training of clinicians on L&D, postpartum and IM on family planning counselling and placement of the contraceptive implant.
Education of clients on long-term FP methods available.
Assure availability of family planning materials, protocols and registers on the services.
Motivation of the staff to satisfy the patients regarding their chosen FP method.
Implant training
The implant training course used was developed through the K4Health (sponsored by USAID, Johns Hopkins University, among other collaborators) ‘Training Resource Package for Family Planning module in French on Implants’.17
Didactic trainings were carried out on the counselling and insertion of Jadelle, a 5-year, two-rod, progesterone-only contraceptive implant for providers on internal medicine, L&D and postpartum services. The trainings lasted 8 hours and were conducted by a nurse midwife.
A pre-test and post-test were given, and PowerPoint presentations, group case studies and training videos in addition to a practice session on the insertion of the Jadelle implant were held. A booklet of training hand-outs, examples of the registers and the WHO chart of MEC for all family planning methods in French18 were distributed.
Each participant was expected to pass the post-test (set at 75%), then correctly counsel and place a minimum of three implants under supervision prior to receiving a certificate of participation and permission to independently counsel and place the contraceptive implants on the inpatient wards.
PDSA cycle 2
May 2016: This second PDSA cycle focused on fine-tuning the strategy with scale-up to ensure sustainability. We continued to motivate the clinicians to satisfy our patients with their chosen family planning method.
Continue to train clinicians on L&D, postpartum and IM on counselling and placement of the contraceptive implant.
Ensure continuous education of postpartum women on the benefits of long-term methods, the importance of family planning/birth spacing and the methods available.
Ensure monthly data collection at all points of service continue to be collected.
Continue to contribute to the overall reduction of morbidity and maternal mortality.
Note: Not part of this specific strategy, however, it was deemed necessary by the clinicians to have short-term methods also available to postpartum women.
As a result of this cycle, we decided to adopt the strategy and agreed to permanent implementation of the changes.
Results
Implant training outcome
A total of 28 clinicians (nurse midwives, nurses and residents in OB/GYN or IM) participated in the Jadelle training in March, April and May of 2016; however, the trainings continue to be held as needed since the end of the QI project. The average pre-test score was 64% and the average post-test score was 89%.
LAC uptake
Implant: With expansion of access, an uptake in the acceptance of the contraceptive implant was seen to have increased significantly following the trainings and implementation of the new strategy. Average acceptance was 0 per month over the previous year, and after the project implementation, 37 contraceptive implants were placed in April, 86 in May and 69 in June 2016 for immediate postpartum women. The continued success of this strategy following the formal end of the QI project in May 2016 can be observed in figures 2 and 3. From May 2016 through August 2017, our services continue to provide counselling and place an average of 47 implants per month on Post-Partum and Labour and Delivery (figure 2), with an average of 20% of women who deliver at the hospital go home with a long-acting contraceptive method (figure 3). Only two implants have been placed in IM service to date.
All women who deliver in the hospital receive group educational messages and family planning counselling prior to leaving the hospital. They are provided with individual counselling if they choose a family planning method and receive the chosen method only after providing their consent. Counselling consists of an explanation of risks and benefits of the method chosen by and appropriate for the individual woman. Women provide their verbal consent for an IUD or implant and written consent for tubal ligations. We educate women on all contraceptive methods available (Depo-Provera, pills, condoms, IUDs, implants and surgical sterilisation) to immediate postpartum women. We observed that despite counselling, the short-acting methods were not noted to have changed during this project.
IUDs and BTLs: All patients are counselled on all family planning methods available; however, uptake of other long-acting methods, on average, lags behind the implant. These methods were not part of the QI strategy and showed very little change over time as seen in figure 2.
We saw a great improvement in the percentage of women who delivered in the Maternity services accepting a LAC method. The average percentage went from 5% to 20% of women being discharged home with LAC (figure 3).
In terms of patient satisfaction, we noticed a minimal number of women return to the facility for implant removal; of the 572 implants placed between January and August 2017, only 54 women returned for removal, a rate of 91% satisfaction. Of the 54 women who presented for removal, 24 (4%) had their implant removed because they had achieved the 5-year lifespan of the method; we can therefore safely say that these women were also satisfied and potentially 95% of women are satisfied with their contraceptive choice. It is important to note that although this strategy was targeting hospitalised women of reproductive age, we also observed an increase in the numbers of women accessing our outpatient family planning services seeking contraceptive implants. Lastly, as we have expanded family planning efforts to become more community-based, uptake among women during our community outreach sessions has also increased. The data from these results are not mentioned here, but it is evident that this strategy has already had a long-lasting and far-reaching impact.
Discussion
Summary
The Ministry of Health strategic repositioning of long-acting family planning with an emphasis on improving access as a key strategy, in addition to the recent MEC changes for the contraceptive implant by WHO from Category 3 to Category 2 for immediate postpartum breastfeeding women helped to inspire this QI initiative and strategy to offering postpartum women LAC options prior to hospital discharge. The interventions put in place have proven sustainable based on our continuous positive results over 1 year later.
Trainings conducted at HUM can be replicated in other institutions throughout Haiti to motivate maternity staff to educate and encourage women’s access to LAC methods immediately after delivery, prior to hospital discharge. Additionally, other institutions can consider, including staff from IM, Paediatrics and other internal wards, to decentralise and broaden access to FP methods, ensuring that women with cardiomyopathies also have access to LAC family planning methods.
Interpretation
As there were no publications found on the impact of QI strategies specifically around the contraceptive implant to compare our findings with, it is safe to say that this strategy is unique in the interventions put in place and the outcomes observed. The limited access to and very high need for broad-scale family planning access improvement strategies in the context of very rural and high maternal mortality in Haiti leaves the door open to many creative solutions to addressing this problem. The strategy undertaken at our facility is only one that has shown great and continued success, and our hope is that it will be applied in other health structures throughout the country and beyond.
Lessons and limitations
Part of the plans for expansion of this project has been to include the paediatric and surgery wards, as well as continuing trainings for staff on the IM ward. In 2017, trainings for nurses and residents in these two new services have been taking place with very poor results. We have not seen the success that has been evidenced on the labour and delivery and postpartum wards. It is difficult to understand why this may be and further investigation into the reasons behind this outcome is necessary in order to continue to improve quality and access to essential preventative healthcare services such as family planning.
The points in time where we see a decrease in results coincide with the peak in deliveries on the Maternity Services (September through December). This is due primarily to lack of time on the part of staff to educate, counsel and offer the method, as they are extremely busy with deliveries and caring for postpartum women and newborns. Our graphs show several peaks and drops as staff motivation waxes and wanes in terms of provision of the counselling and education necessary to meet our clients’ needs.
Lastly, as our demand for the implant in the hospital grew, it became immediately clear that we had to ensure a timely resupply of the product. An increase from 3 to over 100 implants placed per month (including outpatient services) meant communication with the Hospital Administration and supply chain personnel within our network where we provided a logical rationale for the large increase in demand.
Conclusion
The project interventions have proven sustainable over time as evident in our results. Overall, we have seen continued motivation on the part of the staff to educate and counsel postpartum women. We have also observed continuously high numbers of women leaving the hospital with a long-acting contraceptive in place, who show high satisfaction rates. Most importantly, we are able to continue to address the gap in unmet FP needs through improving access to long-acting FP, which consequently impacts actual versus desired fertility among women who reside in the Central Plateau Department of Haiti. This last point will ultimately reduce maternal mortality as women have more control over their fertility and feel educated and empowered to make birth choices that protect themselves and their families.
The LAC trainings and expansion of our family planning services to inpatient services in March, April and May of 2016 resulted in a significant increase in the access to and uptake of the Jadelle contraceptive implant among immediate postpartum women and women with PPCM at HUM. This was an effort to increase accessibility to LAC methods by women after delivery in order to reduce unintended pregnancies, women suffering from very high-risk pregnancies and obstetrical complications and ultimately the numbers of women dying in pregnancy, labour, delivery and the postpartum period at our hospital.
This approach can be replicated in other institutions throughout Haiti and beyond, to impact high maternal mortality rates.
Acknowledgments
We are grateful to the entire nursing and medical staff on the maternity service at HUM for their contributions and dedication to the improvement in the quality of care that is provided at our hospital specifically for the mothers who deliver with us. We would like to thank Marlene Damas Borgella, Nurse Manager of the Maternity services, for her supervision and dedication to both the staff and the welfare of our patients. We also want to acknowledge the dedicated and hard-working QI committee at HUM for their support and continuous feedback with the objective of improving the quality of care provided to every patient that walks through our doors.
Footnotes
Contributors MCJ-B and SL came up with the initial idea for the QI project. MCJ-B designed training, implementation of the protocol, data collection tools, wrote the statistical analysis plan, cleaned and analysed the data, and drafted and revised the paper. MCJ-B is responsible for the overall content as guarantor. SL and EDJ assisted in the staff training, motivation and supervision of correct implant placement. They also assured the successful realisation of the project. CM and JPJ added edits and comments to the working drafts of the manuscript. All authors have approved of the final version of this article while MCJ-B and OS did critical revision of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The authors have disclosed that they have no significant relationships with, or financial interest in, any commercial companies mentioned in or pertaining to this article.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.