Article Text

Abstract
Maintaining quality of care and meeting patient expectations in the face of rising demand within emergency departments (ED) is a significant challenge for clinicians. This study tested the Always Events (AE) approach as a means to identify AE’s relevance to patient care in the ED and act on this to address patient concerns. The project team looked to identify aspects of care patients would like to see improved within the minor injuries stream (MIS). Following triage, patients typically have presentations that do not require admission and require a single interaction with a clinician. Interventions seeking to improve patient experience were created and impact was monitored using patient feedback using a quality improvement (QI) framework.
AEs were identified via convenience sampling using a short semistructured survey questionnaire. Patients were asked ‘What should always happen in the Emergency Department?’ Communication and information provision regarding how the department worked were identified as key themes. Two interventions, an educational poster and a video campaign, were designed and implemented. Improvement was assessed via convenience sampling of patient questionnaires using a 5-point Likert scale and free-text responses.
Initial patient satisfaction levels regarding information provision stood at 80%, rising to 88% after our poster intervention and 92% by the end of the video intervention. Understanding of how the ED functions was initially 83% in the baseline sample before rising to 86% following poster and video interventions. Patient questionnaires indicated that information provision directly from staff was variable throughout the study period.
Implementing the AE approach in the MIS has improved patient experience. Our poster intervention had the greatest benefit regarding patient understanding of the ED and information provision. This project has also indicated that the AE method can be successfully combined with a QI tool and applied in the ED to address patient needs.
- emergency department
- patient-centred care
- patient satisfaction
- quality improvement
- quality improvement methodologies
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- emergency department
- patient-centred care
- patient satisfaction
- quality improvement
- quality improvement methodologies
Problem
The task put to the project team by NHS Education for Scotland (NES) for this improvement innovation study was to examine the validity and effectiveness of implementing the Always Events (AE) approach to quality improvement (QI) in a Scottish emergency department (ED). This is a novel person-centred QI approach which focuses on addressing patient-identified problems in a collaborative manner. This project identified information provision and communication as key themes that needed to be addressed.
Patients presenting to the minor injuries stream (MIS) are people who predominately attend with a single acute issue with the vast majority of patients being discharged from the service. Attending the ED has the potential to be a confusing and intimidating experience for patients. Research has indicated that poor communication and information provision remain a significant source of complaints for EDs.1 Patient perception of topics such as waiting times for assessment and treatment has been previously identified as a significant factor in low patient satisfaction. Increased levels of information provision, including explanations of why waiting times for assessment and treatment occur, have been shown to improve patient satisfaction.2 In addressing the issue of communication and information giving it is important to remain cognisant that attendance to hospital is an irregular and unusual occurrence for most people which can be associated with considerable stress, confusion and anxiety.3–5
Background
The Picker Institute developed the AE concept. An AE is a clear, action-oriented, pervasive practice or set of behaviours that provides:
A basis for partnering with patients and their families.
Actions to ensure patient experience and improved outcomes.
An ongoing commitment to person and family-centred care.6 7
It has the specific aim of explicitly engaging patients and relatives at a local level so that they can influence and define what aspects of care quality and service are meaningful to them on a personal level. It also engages care practitioners in an ongoing commitment to adopting a patient-centred approach to QI that is judged to be feasible in day-to-day practice.8 This is in line with recent emphasis to move towards a more person-centred care approach to improving the delivery of care and the patient experience—as a balance against the overemphasis on clinician and disease-focused models of care improvement.9 10
The generation of AEs requires a reflective, co-design approach to gathering and acting on feedback from patients to enable them to express what is important to them.11 12 The use of an AE within the ED is, therefore, a potentially novel approach to enhance patient experience. Analysis of the strengths and weaknesses identified in the testing of this concept as a QI method should prove useful to other EDs and healthcare providers looking to adopt and implement this method to close the gap in taking a meaningful person-centred approach to QI.
The design and implementation of the project was orientated around the AE model provided by the Institute of Healthcare Improvement which was based on the original approach developed by the Picker Institute—both US-based institutions.8 The project was part of a larger multiprofessional, multicentre programme of testing of the AE concept which was led by the Safety, Skills and Improvement Research Collaborative based in NES and funded by the UK Health Foundation. The ED arm of the project was informed by earlier ‘proof-of-principle’ development work undertaken by NES which led to the redesign of the original criteria for generating AEs based on data collected from patients for the UK healthcare context.13
Our informal project theory of change was developed during early meetings involving our AE study team. It was surmised that via staff engagement in the AE concept of soliciting direct feedback from patients on their care priorities and then linking this to our QI design interventions would lead to improvements in patient experiences of service delivery in the short term. In the moderate to long term we theorised that this would lead to regular adaptation and implementation of the AE approach as a flexible person-centred QI method that could be applied to a range of quality of care issues highlighted by ED patients.
In an ED with approximately 98 000 patient visits annually the project team had to address the patient-identified issues with minimal impact on clinicians’ daily practice and provide maximum impact. Our first objective was to identify patient issues using the AE method. The key themes fed back from patients in our service revolved around communication and information provision on how the MIS operates. With the AE identified, the project team then had to design two sustainable interventions that could become embedded in the ED’s daily practice. The project method, QI interventions and AE style were then appraised for its effectiveness in meeting patients’ needs.
Design
The AE project was conducted over a 6-month period in a tertiary ED in NHS Greater Glasgow and Clyde Health Board. The (MIS) accounts for 41.2% of the patients treated in the ED, 81.2% of whom are discharged from the service. In collaboration with NES, the project team set out to identify issues patients would like to see improved . Patients were asked via a short semistructured questionnaire, ‘What should always happen in the Emergency Department?’ This was collected via convenience sampling. Questionnaires were distributed to patients at random to fill during their episode of care within MIS.
In response to the collected patient-led feedback the project team used iterative thematic analysis to generate measurable and feasible AE that could be implemented via a QI process. The prime theme running throughout our patient population’s feedback revolved around communication and levels and quality of information provision regarding our patients’ stay in the MIU.
Once the AE was identified the project team devised two interventions that acted on patients’ feedback and focused on enhancing patient understanding of MIU care provision. These interventions were then assessed to identify areas for improvement in project design and implementation.
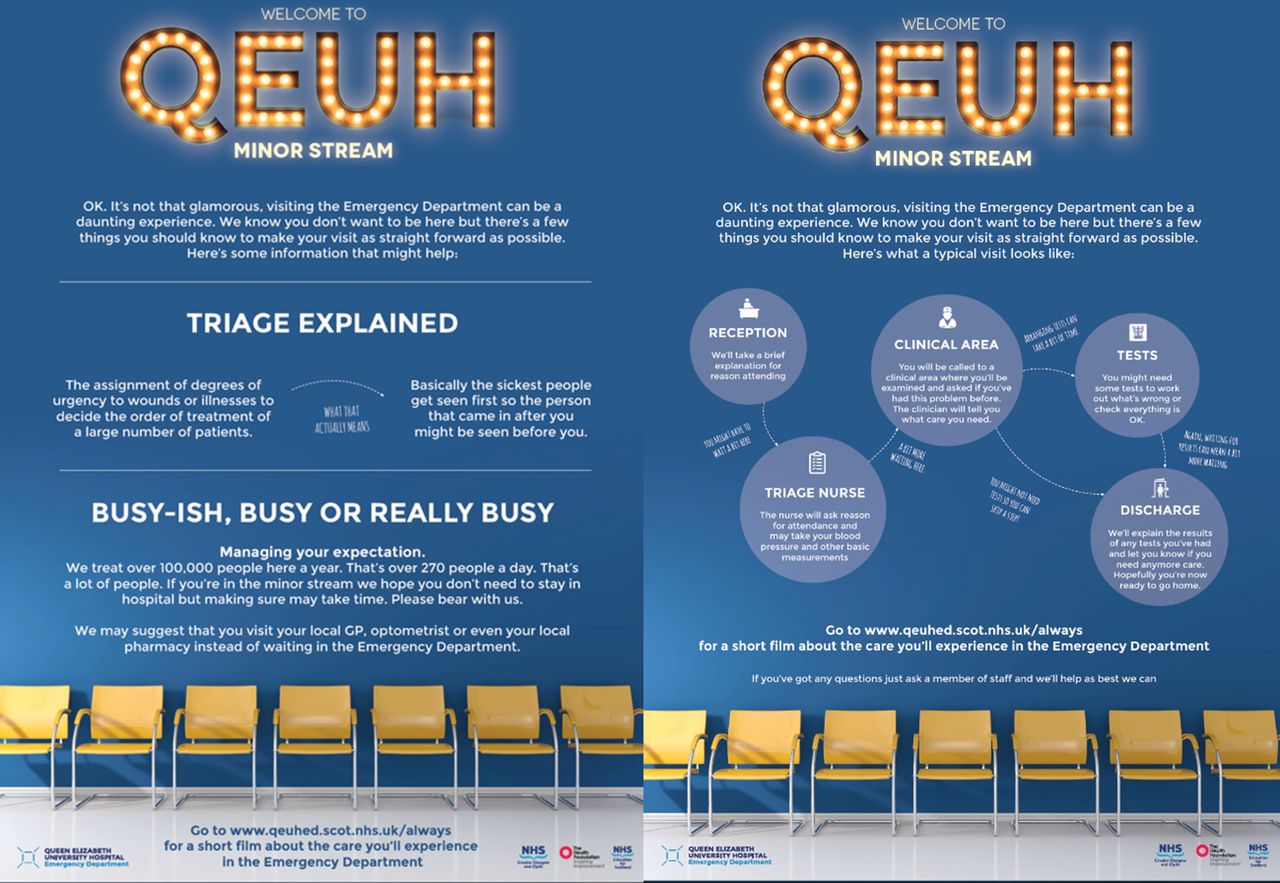
Intervention 1 consisted of a poster campaign (figure 1). The posters explained what the triage process entailed and the staff, tests or investigations that patients are likely to encounter during their visit. Poster content was developed and agreed by authors at subsequent project meetings in collaboration with a print design team. The posters were placed on walls at strategic locations within the ED and waiting room environments to maximise visibility to patients, carers and relatives attending. The layout and font style of the posters were deliberately designed to capture attention.
{kind=link}
Poster interventions.
Intervention 2 involved the implementation of a short 2.5 minute video which featured individual members of the multidisciplinary team ‘speaking to the patient’ and describing each interactive stage of the patient journey as part of a visual ‘walking tour’ of the MIU. The video was professionally developed for a small cost (£2000) and is accessed via patients’ own web-enabled devices. It can be viewed through the following link: https://vimeo.com/191127108.
Sample
The initial thematic data analysis to identify the AE was collected from 68 patients as a convenience sample attending the ED during March 2016.
A convenience sample of 100 patients completed questionnaires (split into 10 equal data collection episodes over a period of 1 month) prior to interventions during the period of August to October 2016. This sampling approach and recruitment were replicated for each intervention from October 2016 to January 2017.
Measurement
A short questionnaire was designed with four questions (box 1) and included a 5-point Likert scale ranging from ‘strongly agree’ to ‘strongly disagree’ for each question response (or ‘highly satisfied’ to ‘highly dissatisfied’ for question 4 as an additional measure of MIS information and communication performance). A free-text box was also included to capture qualitative feedback from patients on these issues and any other aspect of their care.
Questionnaire content
Were you provided with information about how we will provide care during your visit to the emergency department?
Do you understand how the emergency department delivers care?
Did staff keep you informed of your care within the emergency department?
How satisfied are you with the level of care you experienced today?
Questionnaire data were analysed using simple descriptive statistics (eg, frequency counts, percentages, means). Results are presented in terms of the individual and composite levels of positive agreement reported by respondents (ie, the percentage proportion of respondents indicating ‘strongly agree’ or ‘agree’ on the Likert scale for questions 1–3). For question 4, this is reported as the percentage proportion of respondents indicating a positive level of satisfaction (ie, those indicating ‘highly satisfied’ or ‘satisfied’ on the attitudinal response scale).
The initial primary outcome for the AE was measured via improvement in the composite results of questions 1–3. Using a composite result as a proxy for assessing AE performance provides a comprehensive and meaningful measure and indicator of any overall changes related to care improvement that could be influenced by a combination of staff behaviours and action, intervention 1 and intervention 2.
Quantitative data were presented in run charts to plot data trends over time and measure quantifiable changes in the MIU delivery of the generated AE. Qualitative data are presented by a key selection quotes from patients that reflect the scope and nature of feedback provided.
Strategy
The project used Plan-Do-Study-Act (PDSA) cycles for each intervention.
PDSA cycle 1: Our first intervention aimed to distribute informative posters throughout the main waiting area, subwaiting area and individual cubicles of the MIU.
PDSA cycle 2: Use of the posters and videos as an additional information source to address the AE. This was available for patients to view via weblinks on the intervention posters and via prompt cards distributed by triage nurses when the patient was first seen.
Results
Levels of positive agreement with the responses to question 1 increased from 80% at baseline to 88% after intervention 1 (n=100), the poster intervention, and to 92% after intervention 2 (n=100), the video intervention. Improvements were also recorded as indicated in levels of agreement responses to question 2 in terms of patient understanding of the ED process rising to 86% from 83%. For question 3, which related to information provision from staff, levels of agreement were more variable throughout the period of study compared with responses to other questions.
Consistent improvement was found when analysing the composite result for questions 1, 2 and 3, which is the proxy measure for the delivery of the AE, and where responses were directly related to information provision by staff or by the project interventions. The baseline of 82.2% for the composite result increased to 86.3% for intervention 1 and 88.8% by the end of intervention 2.
The variable results for question 4 throughout the process indicated that the interventions did not affect overall patient satisfaction within their care experiences. Decreased patient satisfaction was not found to be affected by periods of increased attendances within the ED when compared with the average number of patients per day over the project period. The average number of patients attending during the ED from July to December ranged from 8244 to 7753 per month with a daily minimum of 204 and maximum of 315.
Run charts exploring these statistics can be found in the online supplementary material.
Supplemental material
An exemplar selection of free-text comments (table 1) is reflective of overall feedback and is largely positive in terms of the interventions that were tested, and the care and service experienced by those patients responding, although there is room for improvement.
Sample of patient free-text responses
Lessons and limitations
This small study demonstrated that the AE concept can inform development of the design for educational interventions in the patient-facing MIS within a busy ED. This had a moderately positive effect on the patient experience with regard to improved information provision and increased understanding of how our ED works. The greatest improvement occurred in intervention 1, the poster campaign. The impact of the video in intervention 2 was limited in its implementation and potential availability.
The strengths of this study included the participatory co-design nature of the study and achieving our goal of involving both patients and staff in testing this novel process. The limitations of the study include the small size in terms of numbers of patients, and the lack of evidence for potential long-term sustainability of improvements reported or the AE improvement method itself.
The poster intervention was simple and sustainable and required limited resource. This intervention showed strong results overall and the patients felt more informed about the ED care process than previously. Information technology barriers in the intervention 2 study period required triage and reception staff to prompt patients to access the video on their own device rather than via hospital televisions or on the login page for patient Wi-Fi. This was particularly difficult to maintain in triage where staff were regularly swapped between roles.
It was essential to listen to concerns staff may have with an aspect of the project to address issues and prevent disillusionment with the process, particularly in a frequently dynamic and complex care setting like the ED.14 Collaborating and communicating with staff on the interventions and reasoning behind them was key in promoting a shared purpose and driving commitment to the project.15
The next steps for the AE team should be to further implement the video within the department’s practice via inclusion on the patient Wi-Fi homepage and waiting room television. This should maximise the impact of the video while ensuring sustainability and inclusivity of the project. This may be more effective than a prompting system which requires active participation from the patients to access information.
Seeking robust qualitative feedback of the intervention would further strengthen the approach. Accessible provision of the video in the waiting room for those with disabilities or non-English speakers would be advantageous but language barriers but would require further resources to provide a solution for. In these cases, the researcher administered the questionnaire and therefore there was a risk of response bias.
It is important that AE interventions are affordable in their application.16 Poster and video interventions incur a reasonable initial cost and have very low recurring costs.
These interventions are potentially sustainable within daily practice with low levels of staff involvement in maintenance after the initial project period. Once a degree of project sustainability is established there is potential for project spread.15 The informative poster interventions can be easily adapted and contextualised for use in other ED as the processes involved are broadly similar providing an ideal opportunity to disseminate the initial work. The current video intervention is specific to our ED but future iterations may be more generic and applicable to other care settings in the UK.
Conclusion
This study illustrated that the AE approach can be feasibly developed and implemented within an ED setting and aligned with a QI method. This process shows promise as means to drive person-centred QI to identify and deliver on priority care issues identified by patients as being of high importance to them in the MIU.
Our poster intervention has given sustainable positive benefits to our ED and strong potential for spread to other MIUs and other hospital departments. Overall, our findings indicate that further integration of the video campaign with hospital technology services such as video services and patient Wi-Fi login page is needed to maximise its efficacy to ensure greater coverage alongside spread and sustainability.
Acknowledgments
The authors offer sincere thanks to all the patients who kindly participated in the project; Daysix for producing the video and poster resources and Malcolm Gordon for critical review during the project. Finally, to NES Always Events team for involving the QEUH team in the project to enhance patient experience.
Footnotes
Contributors DJL contributed to the conception, design and drafting of the manuscript. CK contributed to the recruitment, data analysis and drafting of the manuscript. DT contributed to the recruitment and initial thematic review. SH and NL contributed to the conception and design of the study and critical review of the manuscript. PB contributed to the design, critical review and drafting of the manuscript.
Funding This project was partially funded by The Health Foundation.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Presented at This manuscript was presented at the RCEM scientific meeting and the abstract was published https://emj.bmj.com/content/34/12/A890.2.