Article Text

Abstract
Patients with diabetes require access to systematic and ongoing care delivered by a team of healthcare providers. Despite national attention and well-accepted best practices, diabetic care, blood pressure and haemoglobin A1c (A1c) levels for patients with diabetes in our primary care setting were highly variable and below the Healthcare Effectiveness Data and Information Set (HEDIS) 75th percentile benchmark. From January 2015 to January 2016, 22% of patients with diabetes in our primary care setting had both blood pressure and A1c levels controlled and 23% had their annual diabetic care bundle completed, which includes A1c and blood pressure measurements, foot examination and nephropathy attention. Lack of standardised care algorithms, electronic health record documentation and education was identified. Lean Six Sigma methodologies were used to re-engineer the care that patients with diabetes receive. Key improvement initiatives focused on standardisation of accepted care practices through electronic templates, education and re-evaluation of patients to make 90-day, rapid cycle changes. Interventions were piloted in one primary care clinic then expanded to eight additional clinics. At the pilot site, the per cent of patients who completed the diabetic care bundle increased from 33% to 71% and the per cent of patients with diabetes with both A1c and blood pressure controlled increased from 31% to 43% (two-proportion test, p<0.01) postintervention. On rollout to eight additional clinics, the per cent of patients who completed the diabetic care bundle increased from 23% to 67% and the per cent of patients with diabetes with both their A1c and their blood pressure controlled increased from 22% to 41% (two-proportion test, p<0.01). After the interventions, nephropathy attention, A1c and blood pressure metrics exceeded HEDIS 75th percentile. Standardisation of accepted care practices for patients with diabetes improved compliance with diabetic care bundle completion and patient outcomes in the primary care setting.
- chronic disease management
- diabetes mellitus
- healthcare quality improvement
- primary care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Diabetes has been reported as the seventh leading cause of death in the USA.1 According to the Centers for Disease Control and Prevention, out of 30.3 million people in the USA, 9.4% of the population have diabetes.2 Risk factors for diabetes include smoking, being overweight or obese, physical inactivity, high blood pressure, high cholesterol and high blood glucose.3 Haemoglobin A1c levels are correlated with average blood glucose concentrations for the previous 3 months, approximately. Haemoglobin A1c testing is accepted by the American Diabetes Association (ADA) and WHO as a screening tool for diabetes diagnosis and management.4–6 Diabetes diagnosis is associated with higher expenditures compared with patients with no diabetes, and value-based reimbursement trends, merit-based incentive payment systems and Accountable Care Organization measures have shifted their focus to patient outcomes, including controlled blood pressure.7 8
The ADA defines diabetes as a ‘complex, chronic illness requiring continuous medical care with multifactorial risk-reduction strategies beyond glycaemic control’.9 Care provided to patients with diabetes is highly variable, even though standards of care are fairly well accepted.10 Systematic care provided by a team of healthcare providers is required for patients with diabetes.11
From January 2015 to January 2016, 39% of patients with diabetes in the health system’s primary care service had haemoglobin (A1c) levels in control, defined as A1c <7%, compared with the Healthcare Effectiveness Data and Information Set (HEDIS) 75th percentile benchmark of 43%.12 The per cent of patients with diabetes with controlled blood pressure, defined as <140/90 mm Hg, was 53%, compared with HEDIS 75th percentile of 73%. A limited number of specialists and clinical resources, patient-care fragmentation and rising costs challenged our system to improve ongoing diabetes care in our primary care network.
Bundling diabetic care, including measuring A1c and blood pressure levels, foot examinations and providing nephropathy attention, is one approach to provide systematic ongoing patient care. Compliance with diabetic care bundles and interventions recommended by the ADA is cost-effective and may reduce the risk of complications of care.13 14 Various models have integrated specialised clinics within primary care environments and management of diabetes at the primary care level is associated with improved patient outcomes.15–17
Computerised clinical decision support systems can be used to improve practitioner performance in disease management.18 Weber et al designed a primary care physician all-or-nothing bundle of diabetic care using electronic health record (EHR) tools including patient report cards, alerts for examinations that had not been completed and EHR decision support. The per cent of patients with A1c levels <7% increased from 32% to 35% and the per cent of patients with controlled blood pressure, defined as <130/80 mm Hg, increased from 40% to 44%.19 20 Jaffe et al implemented a hypertension programme that included evidence-based practice guidelines for pharmacological treatment and follow-up visits after medication adjustments, which was associated with improved hypertension control rates.21
The goal of this project was to develop a chronic care model for ongoing, continuous use within the primary care setting to improve diabetic performance consistent with HEDIS 75th percentile, increase the percentage of patients with diabetes whose A1c and blood pressure levels are controlled, as well as improve the percentage of patients who have their diabetic care bundle completed.
Methods
The study was performed in a primary care network with >100 providers in Illinois, USA, with a volume of 300 000 patient visits per year and 11 159 patients with diabetes on the provider’s panels in 2016. There were 6663 patients with an outpatient visit for diabetes or who were dispensed a diabetic medication, defined by the National Drug Code list for comprehensive diabetes care, between 1 January 2015 and 31 December 2016 through the primary care clinics.22 The project was piloted in a primary care clinic of 16 physicians and advanced practice nurses with 1422 patients who met inclusion criteria preintervention. A cross-departmental project team, comprising ambulatory leadership and frontline staff, including physicians, nurses, care coordinators and informatics, met weekly while planning and designing the improvement initiatives.
Annual diabetic care bundle completion was defined as (1) an A1c test, a blood pressure reading, a monofilament foot examination, a retinal eye examination and nephropathy attention either via protein urinalysis testing or an angiotensin-converting enzyme inhibitor/angiotensin II receptor blocker prescription, or (2) a chronic kidney disease/end-stage renal disease diagnosis, annual A1c test completion, A1c control, nephropathy attention and blood pressure control all below the 50th percentile when compared with HEDIS.12 23
Outside barriers prevented the ability to verify completed annual retinal eye examinations. The team was unable to accurately identify outside eye care providers and date of service. If an eye examination report was received then there was not a standard location for scanned documents in the EHR and information was not consistently documented, resulting in duplication of searches. Due to barriers in obtaining verification that patients had completed their annual retinal eye examination, retinal examinations were removed from the scope of the project.
Lean Six Sigma Define, Measure, Analyse, Improve and Control (DMAIC) methodologies were used to re-engineer the care that patients with diabetes receive. Six Sigma methodology focuses on decreasing defect rates and variation and was pioneered by manufacturing companies such as General Electric.24 Lean principles focus on eliminating waste and non-value added activities and companies rely on lean management principles for increased quality production and reliability, including Toyota.25 26 Although initially implemented in manufacturing, Lean Six Sigma tools can effectively aid service industries, including healthcare.27 Redesigning healthcare processes based on Six Sigma and lean thinking can significantly improve healthcare processes and outcomes, although additional studies are needed.28 29
The project team completed workflow process mapping and a Critical-to-Quality Tree to understand the current process and critical requirements. Design of optimal process flows identified several gaps and defects related to the current process (online supplementary figures 1 and 2). Analysis of these gaps using affinity diagramming and a five why analysis revealed barriers and ‘critical X’s’ to using the optimal path of care a patient with diabetes should receive (online supplementary figure 3). Critical factors included: (1) lack of a standardised care algorithm in treating a patient with diabetes including revisits, diagnosis criteria, clinical judgement gaps, when to refer and protocols for ordering, testing and monitoring patient labs; (2) variation in documentation and lack of standardised means of documentation within the EHR; and (3) lack of education for patients with diabetes including interoffice education and lifestyle modification changes. The project team used an Impact/Effort Matrix to evaluate the effectiveness of proposed interventions as it related to identified gaps and determine which interventions should be pursued (online supplementary figure 3). Provider and clinical staff were seen as key stakeholders in the improvement process; their buy-in to outlined improvements were critical for success and sustainability.
Supplemental material
Using guidelines established by the American Association of Clinical Endocrinologists and the American Association of Diabetes Educators (AADE), a standardised diabetic care algorithm was implemented.30 31 The algorithm focused on addressing lifestyle based on the AADE7 self-care behaviours, reducing risk, addressing education and setting patient goals.31 The algorithm illustrated the path to optional medication treatment for an A1c level of 6.5% and targets the goal of A1c under 7.0%. The algorithm focuses on rapid cycle changes with the patients along with key messages including setting patient goals and making changes when they are not met in order to improve results, as well as yearly completion of the diabetic care bundle (online supplementary figure 2). The algorithm of care still allows for provider clinical judgement in cases where clinical exemption for age, frailty, terminally ill patients, patient refusal and other circumstances where risks are outweighed by improved control.
Standardised EHR templates were built to reflect the algorithm and drive compliance. The templates act as decision support tools for providers and allow for focused change efforts on the front end. The template provides error-proofing in the needed care components of the diabetic algorithm. A pre-visit template was developed that includes recent visits and tests, upcoming examinations that are due, existing complications, home monitoring and lifestyle questions (online supplementary figure 4). A metabolic syndrome history of present illness template was created to standardise documentation of symptoms, lifestyle, medications, goals and chronic disease status (online supplementary figure 5). A metabolic syndrome CarePlan template was implemented to standardise documentation of diabetic education, medication, follow-up goals with timelines, diabetic bundle components, home monitoring, treatment goals and medication recommendations (online supplementary figure 6).
The team worked with Certified Diabetic Educators from the affiliate Weight Loss and Wellness clinic to develop two levels of diabetic education for clinical staff so that onsite, on-the-spot training could be provided to patients with diabetes. Level one education focused on immediate survival skills and patient understanding of the disease and its risks. Life style issues from the AADE7 Self Care Behaviours Framework were included.31 Level 1 education was completed through computer-based learning and competency checks in the primary care setting across all clinics. Level 2 education focused on behaviour change barriers and goal setting. Certified diabetic education was emphasised. However, timely and patient centric needs were recognised and lower levels of education were devised to fill the gaps and assist patients in the movement to the most comprehensive education possible. Level two education was completed through onsite learning sessions to all midlevel providers and also included diabetic screening recommendations, risk factors, diagnosis criteria and the ADA glycaemic control algorithm including how often diabetic care bundle components should be completed.
The standardised diabetic algorithm and EHR template were piloted simultaneously at the pilot site over the course of 4 weeks. In order to test the effectiveness of education in diabetes, a care coordination nurse was on site throughout the clinic in order to provide real-time education and survival skills to patients. Onsite support for care algorithm questions and EHR questions were continuous through the first week, with connections to those same resources remaining in a virtual state for the remainder of the pilot. To give providers real-time results, manual chart audits were completed on all patients assessed with diabetes and shared with providers on a weekly basis. Debriefings were held weekly throughout the pilot to share suggestions and changes needed to make any rapid cycle changes required in the EHR and workflow to aid providers.
The improvement phase of the DMAIC process occurred first at the pilot site, with full rollout across all primary clinics on statistically significant improvement at the pilot site. The designed work flow was a change in provider processes and required a heavy lift from physicians and midlevel providers. In order to gain provider buy-in, pilot site providers gave input into the improvement initiatives and to lead the way in improving care for patients with diabetes. After a successful pilot with improved processes, rollout to other clinics was initiated with eventual successes in patient outcomes.
Overview of the project and initial results were shared with senior leadership to gain buy-in and support. Communication of pilot results was sent to all providers and leadership throughout all clinics. Physician champions were identified and met with in order to gain buy-in and support at the provider level at every clinic. Training and education were completed for all providers and clinical staff involved in the interventions. Over the course of 3 weeks, the rollout of the algorithm and EHR template interventions occurred at the remaining eight primary care clinics. The same onsite support that was present during the pilot was used throughout the rollout. Suggestions and feedback were evaluated by the project team. Diabetic bundle completion and outcomes are shared with providers monthly.
The final improvement phase was error-proofing the improvement initiatives and elimination of old EHR templates as they pertained to diabetes. Diabetic bundle completion and outcome measures were analysed by two-proportion tests in Minitab before and after the intervention at the pilot site and eight primary care clinics. Bundle completion was measured immediately following rollout and diabetic outcomes, including A1c and blood pressure, were measured starting 3 months post rollout since haemoglobin A1c levels are correlated with blood glucose for the previous 3 months.4–6 A p value of <0.05 was considered significant. This project was reviewed by the local institutional review board. It was determined that this project was not research involving human subjects.
Results
Providers reported a 10-patient learning curve to embed the updated workflow into their practice. During the initial transition, the clinic workflows and scheduling were slowed down. Providers adapted by limiting patients with diabetes scheduled back to back in the new workflow. Post implementation analysis was completed to examine provider office time spent with patients. No significant differences were noted in the study.
Postintervention at the pilot primary care clinic, the per cent of patients with A1c and blood pressure measured, a foot examination completed and nephropathy attention provided was significantly increased. The per cent of patients with A1c levels <7% increased from 39% (573/1469) to 50% (109/218) (two-proportion test, p=0.002) and the per cent of patients with blood pressure levels <140/90 mm Hg increased from 75% (1102/1469) to 83% (181/218) (two-proportion test, p=0.004), above the HEDIS 75th percentile benchmark (figure 1).

Diabetes performance at the pilot primary care clinic was improved postintervention (two-proportion test, p<0.01 for all pre/postcomparisons). The per cent of patients with nephropathy attention, A1c levels <7% and controlled blood pressure exceeded the HEDIS 75th percentile benchmark postintervention. HEDIS, Healthcare Effectiveness Data and Information Set.
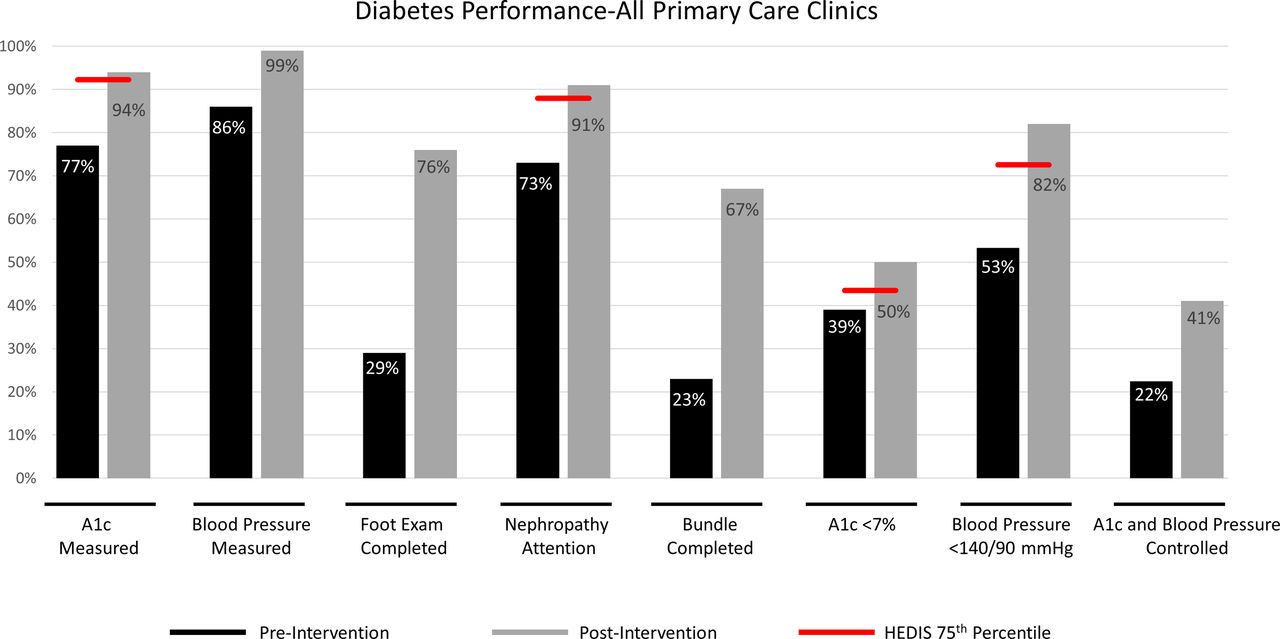
Similar to the pilot clinic, postrollout to all primary care clinics, completion of diabetic care bundle components and diabetic outcomes were improved. The per cent of patients with A1c levels measured increased from 77% (5131/6663) to 94% (474/504), above HEDIS 75th percentile (two-proportion test, p<0.001). In addition, the per cent of patients with nephropathy attention increased from 73% (4864/6663) to 91% (459/504), A1c levels <7% increased from 39% (2599/6663) to 50% (252/504) and controlled blood pressure levels increased from 53% (3532/6663) to 82% (414/504) (two-proportion test, p<0.001), all above the HEDIS 75th percentile benchmark (figure 2).
{kind=link}
{kind=link}
Diabetes performance at all primary care clinics was improved postintervention (two-proportion test, p<0.001 for all pre/postcomparisons). The per cent of patients with A1c levels measured, nephropathy attention completed, A1c levels <7% and blood pressure <140/90 mm Hg exceeded the HEDIS 75th percentile benchmark postintervention. HEDIS, Healthcare Effectiveness Data and Information Set.
Discussion
The interventions primarily focused on changes within the providers’ workflow. These interventions had significant results but did not eliminate the providers’ voice through clinical judgement. The team benefited from strong physician leadership and prior experience in process improvement work. The team was able to express views and perspectives of value in order to drive progress.
Lean Six Sigma is a powerful operation improvement method for today’s healthcare environment promoting gains in quality, safety, service and cost. This data-based approach aligns with the scientific method but requires strong interdisciplinary teamwork, real-time monitoring of results, and managerial and physician leader engagement and willingness to confront resistance to changing the status quo.
Diabetic bundle components and outcomes were significantly improved. In a previous study, implementation of an all-or-nothing bundle of diabetic care using patient report cards, alerts for examinations that had not been completed and EHR decision support, the per cent of patients with A1c levels <7% increased from 32% to 35%, a 9% improvement, compared with 39% to 50%, a 28% improvement in our study. Weber et al reported that the per cent of patients with controlled blood pressure, defined as <130/80 mm Hg, increased from 40% to 44%, a 10% improvement, compared with 53%–82%, a 55% improvement in our study.19 However, a direct comparison cannot be made due to differences in controlled blood pressure definitions.
A limitation of this project is that interventions were limited to one primary care health system and results cannot be generalised. Additionally, knowledge of staff education was not formally tested. Patient-specific diabetic knowledge gaps were not formally measured but were based on the clinical assessment by the provider. Use of electronic tools in the EHR for all primary care clinics post intervention was 46% and compliance with the utilisation of standardised documentation tools continues to be pursued to further improve patient outcomes.
The project aim was to improve patient outcomes in blood pressure and A1c control, focusing on a solution that would be sustainable over time. To maintain gains, a 3-pronged approach was used combining Lean Six Sigma, Change Management and Risk Management strategies. As part of the Lean Six Sigma methodology, a control plan was developed that focuses on monitoring compliance with the process to drive patient outcomes.
A team comprising clinic leaders and support staff monitors compliance with the use of dashboards. Results are shared monthly with all providers, leaders and staff. Leaders are asked to identify and share potential risks to the process and plans are developed to address identified risks as needed. Proactive rounding is completed monthly to identify and mitigate problems and provide support for required change, with continuous support given to late adopters and to address resistance. The team error-proofed the process with the elimination of old EHR templates to ensure use of the new forms.
Standardisation of accepted care practices for patients with diabetes improved compliance with diabetic care bundle completion and patient outcomes in the primary care setting. The success of improved outcomes through standardisation in clinical processes sets an organisational model and provider buy-in for application to other costly complex care issues including depression and congestive heart failure. Additional interventions are in progress to address deficiencies in the diabetic eye examination, point of care A1c testing and attendance at diabetes self-management classes.
Acknowledgments
Amber Bertetto, LPN, Carolyn Lawrence, RN, Ashley Wood CLSSGB, Chris Nienajadly, Barbie Gold, MSMOB, CLSSGB.
References
Footnotes
Contributors TK: contributed to study design, analysis and interpretation of data, drafting and revising the manuscript and study supervision. JR: contributed to study supervision and strategic oversight. MH, VD and GS: contributed to study design and physician buy-in. CJ: contributed to analysis of data and critical revision of the manuscript. AB, CL, AW, CN and BG: were part of the project team and significantly contributed to the success of the project. All authors reviewed the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.